
Abstract
Introduction
Effective care for many acute and chronic illnesses requires continuous monitoring and self-management support for coordinating patient care. Mobile phones can be used to deliver health assessment, education, and other services, including reminders to patients between in-person encounters. The U.S. Department of Health and Human Services is actively exploring patient-centered, mobile health (m-health) technology, including mobile phones, as a tool for increasing both the quality and quantity of disease management to reach and support vulnerable underserved populations like rural communities. According to the Department, mobile phone use has increased exponentially with 302 million wireless subscribers in the United States and an estimated 5 billion mobile cellular subscriptions worldwide in 2010. 1
In 2009, a study conducted by the New England Healthcare Institute found that poor medication adherence results in increased disease severity, increased use of healthcare resources, high avoidable treatment costs, and thus poor health outcomes. 2 Estimates of poor medication adherence are reported to result in about $290 billion in unnecessary spending each year, which includes $100 billion in avoidable hospitalizations alone. 2 Several available behavioral and educational strategies have been shown to improve patient medication adherence. Mobile phone-based text messaging may prove to be a new and innovative way to communicate with patients and increase medication adherence. 3 Also, it is possible that this delivery of m-health services and patient use may be sustainable as it may be reimbursed by Medicare in the future. 2
Several studies have examined the usefulness of m-health technology services. A recent systematic review and meta-analysis from the Clinical Trials Unit of the London School of Hygiene and Tropical Medicine reported that the short message service appointment reminders have modest benefits in improving the healthcare delivery processes and that implementation of such reminders would be appropriate. 4 In a 3-month trial in a Chinese general hospital, patients were satisfied with and had positive attitudes about the individualized pharmaceutical care delivered via text messages to patients' mobile phones. 5 The text messages were used (1) to remind patients to refill their medications, (2) to serve as medication administration time alarms, (3) to deliver practical information about medicines (e.g., administration methods), and (4) to provide adverse drug reaction information. In another study, kidney transplant recipients, especially ethnic minorities, had a positive overall attitude toward an m-health remote system that can monitor medication regimen adherence and physiological parameters to improve long-term graft outcomes. 6 Other investigators evaluated the telephonic patient–pharmacist encounters that provided information on inhaler use technique and self-management to underserved rural asthma patients. 7,8 These studies showed the need to further demonstrate the role and value of telephonic pharmacist–patient interactions in resolving access barriers and improving patient care delivery. 7,8
M-health services like text messaging can promote safe medication use by improving the knowledge of pharmacists and patients, pharmacist–patient interaction, and pharmaceutical care. 7 Whether or not the value of m-health services has been proven, a growing segment of the U.S. population is becoming accustomed to certain m-health services and, perhaps, beginning to expect such services. 9 Mobile phones are increasingly becoming a service channel for pharmacies. 9 Walmart, CVS, Rite Aid, Walgreens, and Target have recently started offering mobile phone-based short message service alerts that make the process of filling new or refill prescriptions more convenient. 9 These large chains accounted for the majority of the U.S. prescription dispensing revenues in 2012. 10
Given resource constraints and access barriers experienced by rural healthcare providers and systems in the United States, m-health could be especially useful for coordinating care in this population. However, the demand for and attitudes toward m-health services in rural patient populations are unknown. The results of the current study will enable pharmacists and other providers gain a perspective about the rural population's access to and willingness to use m-health technology services in coordinating their healthcare. This information will help providers design and deliver patient-centered m-health interventions that could improve the patient's health outcomes (medication adherence and safe medication use behaviors) and patient satisfaction with pharmacy services.
This pilot exploratory study was designed with a purpose of evaluating the potential demand for m-health technologies in delivery of patient-centered services in rural populations. Responses to a survey were used to describe a rural patient population's access to mobile phones and willingness to receive m-health services for pharmacy-related and other health-related information.
Subjects and Methods
An anonymous, paper survey was completed voluntarily by patients visiting two pharmacies in rural Nebraska from August to October 2011. The 2-page survey collected data on patient demographics, health status, access to mobile phones, and willingness to receive (in terms of willingness to use and give time to) mobile phone-based pharmacy and other health services. Items from a previously validated, self-administered comorbidity questionnaire 11 were also included in the survey. The University of Nebraska Medical Center's Institutional Review Board reviewed and approved the study as “exempt” from human subject research requirements. Responses from the paper survey were entered into a Microsoft® (Redmond, WA) Excel® spreadsheet. All data analyses were performed using the statistical package Statistical Analysis Systems software SAS version 9.3 for Windows (SAS Institute, Inc., Cary, NC).
Results
The majority of the 24 respondents (Table 1) were 19–40 years old (52%), female (88%), married (63%), with >$35,000 annual income (55%), with excellent to very good health status (63%), with no comorbidities (83%), with ≤$100 monthly medication expenses (80%), with private insurance (78%), and living within 5 miles of their pharmacy (71%). Only 17% (4/24) respondents reported one or more comorbidities.
Summary of the Characteristics of Survey Respondents (n=24)
About 95% (20/21), 81% (17/21), 73% (16/22) and 55% (11/20) of respondents self-reported access to a mobile phone, voice mails, text messaging, and mobile phone applications, respectively (Fig. 1). Of the 67% (16/24) respondents who rated importance of m-health services, the majority (75%, 12/16) reported that m-health services are important to them. Respondents were asked separately about their willingness to receive mobile phone messages prerecorded by their doctor(s) and by their pharmacist(s): 65%, 57%, 52%, and 48% of 23 respondents expressed their willingness to receive a doctor's prerecorded prompt for appointment reminder, disease information messages, medication use/self-care messages, and symptom monitoring messages, respectively. In addition, 70%, 63%, 61%, 54%, and 50% of 24 respondents expressed a willingness to receive a pharmacist's prerecorded message prompt requesting patient contact with the pharmacy, new/refill prescription reminders, possible medication problem alerts, review and monitoring of medication use, and information on self-managing medication use or preventive healthcare (immunizations and health screenings), respectively. Of the 44% (7/16) respondents who were willing to give time for m-health services, 83% were willing to give 15 min, and 17% were willing to give 30 min every month.
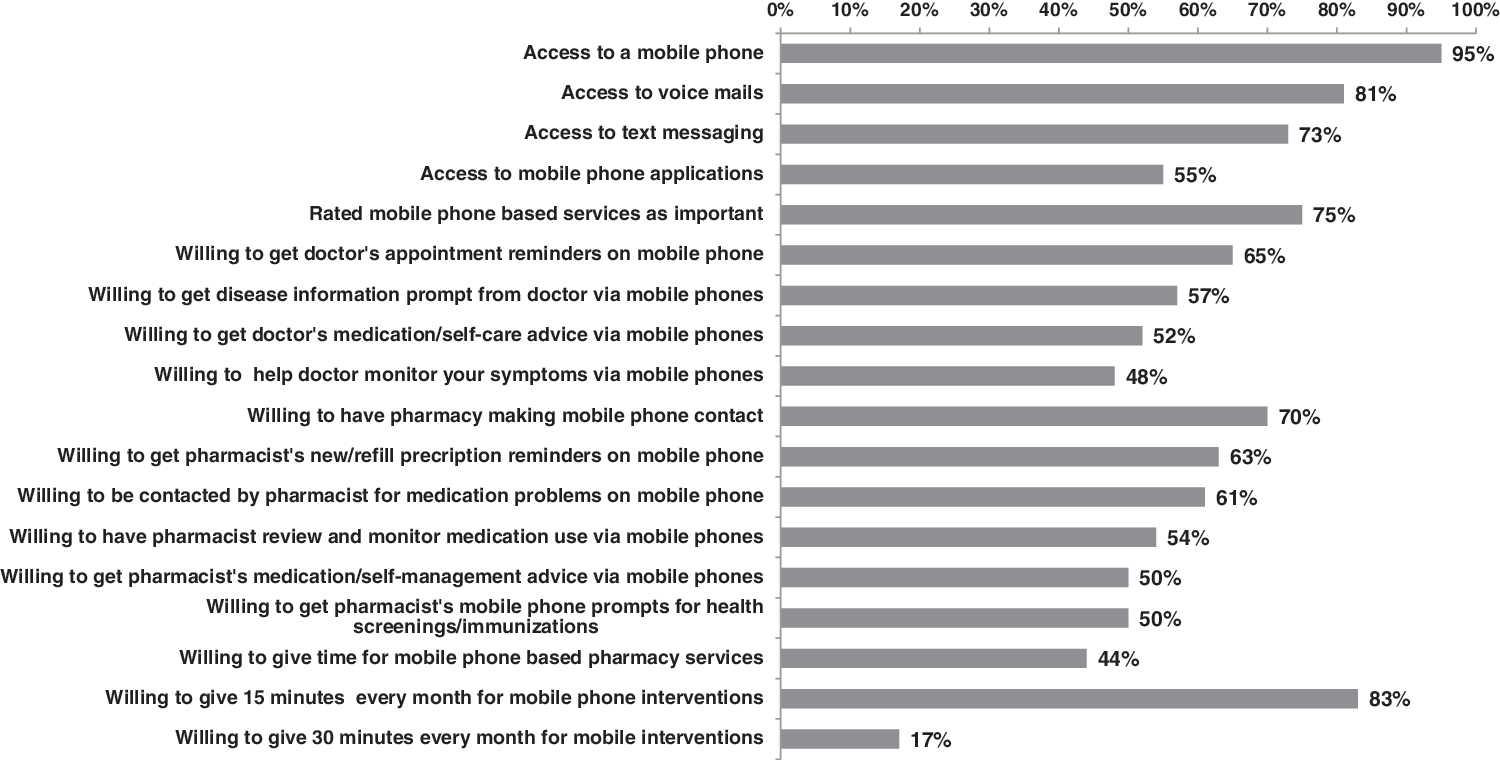
Rural patients' access to mobile phone technologies and willingness to receive mobile health services from doctors and pharmacists.
Discussion
This is one of the first studies to demonstrate that the majority of rural patients rated mobile phone-based services as important (75%) and that about half are willing to receive m-health service prompts from doctors and from pharmacists to monitor and coordinate their care. Survey respondents who were young and healthy based on their self-reported health status, having access to health insurance and convenient access to a pharmacy (71% lived within 5 miles of their pharmacy), had positive attitudes and were willing to give time for m-health services. When rural patients' uses of various mobile technologies were compared, their access to mobile phones was the highest, followed by their use of voicemails, text messaging, and, finally, mobile applications. This finding could be a consequence of the recent growth of m-health applications. One report has predicted that in 2017, worldwide m-health market revenue will total $26 billion. 12 Thus, the trend toward use of m-health applications is likely to increase with the growth and popularity of smartphones and related m-health applications. The demand for m-health applications is not surprising considering that the majority of the respondents to this survey were young and healthy (based on self-reports of good to excellent health status).
Limitations and Future Research
Nonresponse bias, due to the small sample size of this pilot study, self-selection bias, and missing data could have affected our findings. Nonrespondents may be patients not interested in m-health technologies and could have contributed to selection bias. Potential demand for m-health-based pharmacy services in urban areas exists, but our study was limited to patients visiting rural pharmacies. Hence, these survey findings cannot be generalized to apply to other rural and urban pharmacies or to patients in regions other than the Midwestern United States. Further research would be required to evaluate the access to mobile technologies and attitudes toward m-health in these other populations. Older adults are more likely to have chronic diseases and could benefit from m-health-based pharmacy and other health services. Because the majority of our respondents were young adults, further research is needed to determine whether older adults are as willing to receive and give time for m-health services that may be complex to use. Lastly, this study examined patients' perspective only. The views of the pharmacists and other providers on designing and implementing such services and the perspectives of insurance payers on providing coverage for these services were beyond the scope of this study but are areas for future research.
Conclusions
As one of the first to demonstrate a potential demand of rural patients for m-health (including pharmacy) services, this pilot study suggests that rural patients have access to mobile phones and may be willing to use and give time to m-health technology services. Further research is needed in using the novel use of health information technology via m-health services to deliver and coordinate transitions in patient-centered care in the United States, including rural communities.
Footnotes
Acknowledgments
We thank the two rural pharmacies in Albion, NE, that helped collect survey data from patients visiting their pharmacies as well as the patients who volunteered to complete the surveys. We would like to acknowledge Cindy Schmidt, MD, MLS, at the McGoogan Library of Medicine from the University of Nebraska Medical Center who reviewed our article and provided editorial assistance.
Disclosure Statement
No competing financial interests exist.