
Abstract
Introduction
Over the past century, advances in public health and medicine have improved life expectancy of the public in developing and developed countries. Evaluations of the provision of health services have been focused on mortality. 1,2 Health-related quality of life (QoL) of patients with preventive, caring, and curing interventions has been investigated. 3 Utility-based methods of QoL are increasingly used as health outcome estimations. 4 These estimations integrate both survival and QoL to assess quality-adjusted life expectancy (QALE) and provide measures of outcome evaluations on the effects of medical care. 5,6 Although QALE methods have been implemented for healthcare evaluation in patients with acute diseases and chronic diseases, 7 little research has applied this concept for evaluating healthcare provision through the telecommunications system. 8,9 Furthermore, improvement in both access and health status for minority population groups and the population living far away from the medical centers is a major challenge and leaves a void in the literature. This study used the QALE method to assess health status changes of rural residents before and after introducing telemedicine health services.
In Taiwan, the universal National Health Insurance system was established in 1995. The government serves as a single insurer. Enrollees enjoy almost free access to healthcare with a small co-payment by most clinics and hospitals. Although the eventual goal of the National Health Insurance is to eliminate health disparities, high-quality medical care is difficult to access for remote populations, and medical resources are underdistributed in rural areas. Because of geographic barriers, telemedicine was introduced for remote areas, in Penghu County, for instance, to meet the specific healthcare demands in offshore archipelagoes in Taiwan from 1995 to 2004.
The area of telecommunications health services is relevant for the treatment of ill health and the provision of preventative medicine and medical consultation. Telemedicine is particularly applicable for the facilities available to physicians at remote sites to provide healthcare in rural areas, online continuing medical education for physicians in these areas, and special medical services for the elderly, the handicapped, and terminally ill patients at home. From 1995, the numbers of remote areas with telemedicine health services has continually risen. In 2004, there were 24 isolated areas. Penghu County was the county that had telecommunications health services over the whole period of 1995–2004. The 92,000 citizens in Penghu County are regarded as the population of concern.
After 2004, the research report conducted by the government sector indicated that the average cost of each telemedicine visit was around 800 U.S. dollars and was greater than that of each conventional health service event, which was around 740 U.S. dollars. The cost-benefit analysis cast doubt on the telemedicine system. 10 The provision of telecommunications healthcare is still in qualitative pilot experiments in the private sector. Based on Taiwan's experiences of telemedicine provision, this article aims to investigate how the introduction of a telemedicine system influenced rural residents' health status, which is measured by QALE changes.
Materials and Methods
Individuals or patients pursue life periods of utility. Utility depends on the quantity of living life longer and the quality of living life better. Survival function reflects the possibility of survival at different ages. Utility-based methods assign a value to a specific health status to represent the patient's QoL.
11
The values of 0 and 1, respectively, represent the worst and the perfect health status. Public health researchers regard life expectancy as a good proxy to reflect population health.
12
Applying utility-based methods,
2,4
this research quantifies population health status without concern of disease by the indicator of the life expectancy at birth and assigns the perfect health of the newborn population a weight of 1 as well as the worst health of those >85 years old a weight of 0. This assignment is in line with the concept of a previous study.
13
The older the population, the less the health stock, and the more the individuals are willing to pay for extending their lives. The QoL score of each person at age i across the population in the specific area is as follows:
The QoL decreases with increasing age. Based on the life table from the vital statistics of Taiwan for the population 0–85+ years, dividing the numbers of those dying by the stationary population yields the conditional death ratio and hence the survival ratio at age i of i:pi
. The cumulated survival ratio is calculated as Si
=pi
–1×Si
–1. Combining QoL with the survival ratio at different ages yields QALE in terms of quality-adjusted life years (QALYs)
14
:
The estimated QALYs are to evaluate the effectiveness and appropriateness of health policies regarding the effects of using telemedicine health services on the population's QoL. Research conducted under this aim addresses the fundamental issue about what differences telemedicine health services make by examining how many changes of QALE there are for rural residents after the introduction of telemedicine health services.
Using Eq. 2, we further adjust the population of concern's QoL by incorporating the factor of different life expectancy at birth as follows:
Equation 3 reflects that the population living in the area with longer life expectancy at birth has a higher QoL than the population living in the area with shorter life expectancy at birth. Eighty-five cases for persons with life expectancy at birth from 85 years to 0 years are picked from the population of concern and the index population and regarded as a national example to illustrate the proposed methods. For understanding the need of telemedicine provision over the population's entire lifetimes, we calculate the log value for the survival ratios of both the index population and the population of concern as follows
4
:
Subjects
Based on vital statistics data from the Ministry of Interior in Taiwan, for the 92,000 people in Penghu County, the life expectancy at birth increased from 75 years in 1995 to 78.18 years in 2005. The residents living in Penghu County remained nearly constant, and they are regarded as the population of concern. By comparison, in Taipei, the capital of Taiwan, 2,663,000 people had a life expectancy at birth of 79.11 years in 1995, and 2,622,000 people had a life expectancy at birth of 81.79 years in 2005. Residents living in Taipei access clinics and hospitals easily and are regarded as the index population.
Research Method
This research aims to examine how many QALY changes occur with telemedicine health services in rural areas. Combining the index population with the population of concern, this study further investigates the evolution of the relative survival ratios along with telemedicine over the populations' entire lifetimes. Research results are discussed along with the policy implications.
Data Description
The data of variables of life expectancy at birth and the death ratio across populations were collected and published as the vital statistics of Taiwan from the Ministry of Interior. Incorporating the data with Eqs. 1 –3, we calculate QALE at different points in time by Excel® (Microsoft®, Redmond, WA) spreadsheet application.
Results
The QALE calculation presents results for the population of concern before and after introduction of health services through the telecommunications system. The shaded area in Figure 1 indicates that the population of concern had 34.56 QALE in 1994 before the introduction of the telemedicine system. The shaded area in Figure 2 shows that the same population had 37.47 QALE in 2005 along with telemedicine health services. Providing telemedicine health services increased the QALE of the population of concern by 2.91 QALYs.

Quality-adjusted life expectancy (QALE) in the population of concern in 1994. QoL, quality of life.
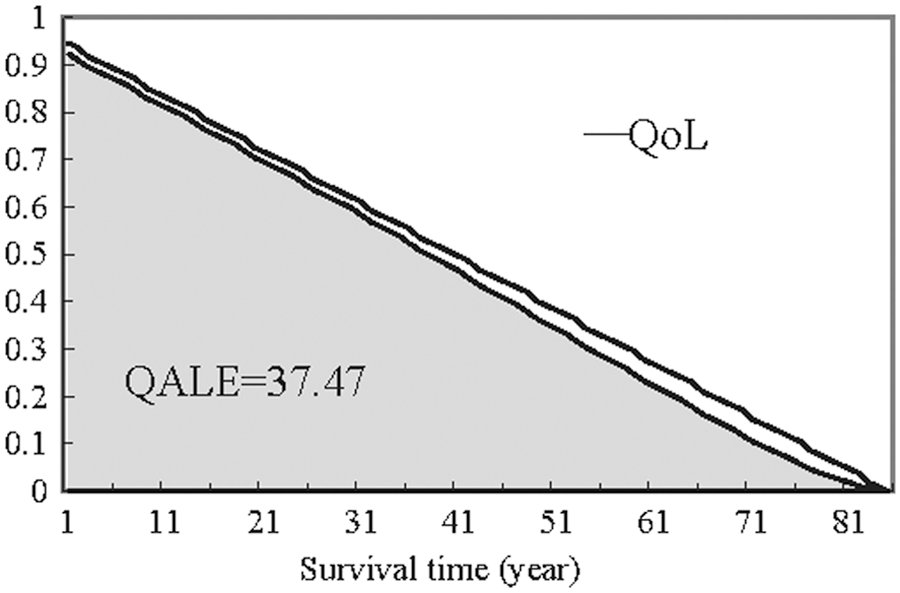
Quality-adjusted life expectancy (QALE) in the population of concern in 2005. QoL, quality of life.
Figure 3 presents the log value of survival ratios for the population of concern and the index population 0–85+ years in 1994 and 2005, representing, respectively, the year before and after introduction of telemedicine, as mentioned above. The survival ratios of the population of concern are lower than those of the index population in 1994 because the log value of the survival ratios is negative. Introduction of telemedicine health services has increased the rural residents' survival ratios significantly. The survival ratios of the population of concern 0–50 years of age are higher than those of the index population at the same age in 2005. The survival ratios of the population of concern >65 years decreased faster and are less than those of the index population >65 years by at least 7% and 3%, respectively, before and after the introduction of telemedicine health services. It appears that the needs for telemedicine health services increase along with the aging of our society in rural and underserved regions.
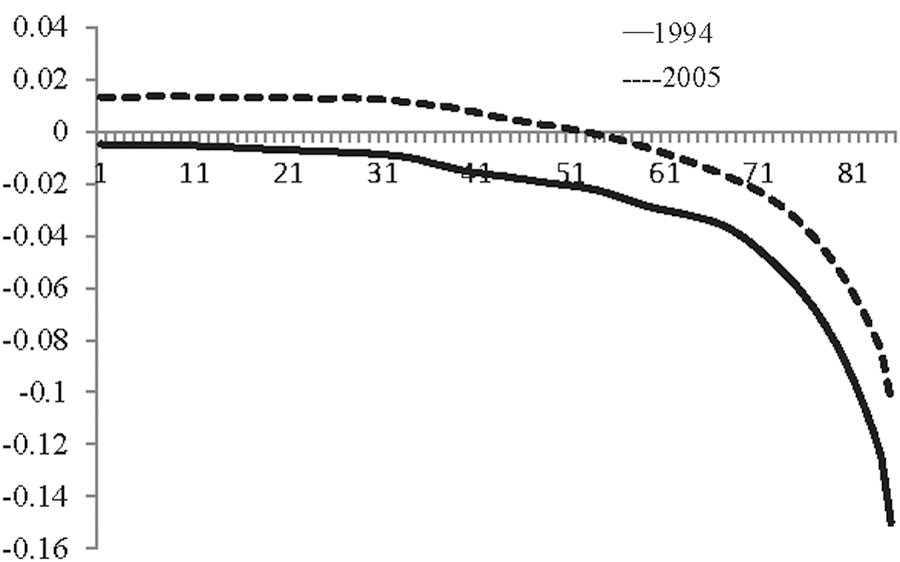
Log value of the survival ratios for the population of concern relative to the index population in 1994 and 2005.
Discussion
Healthcare provision aims to enhance health and improve the QoL. Rapid increases in healthcare spending affect government health programs. This research explores a different approach to give the implication that the society should be concerned with the accessibility of health services for persons living far away from medical centers. Based on the QALE performance of health services provided through the telecommunications system, telemedicine can possibly solve the difficulties of deficiencies in medical resources in rural areas. Furthermore, Figure 3 shows that the provision of telemedicine for the remote aging population in rural areas is an increasingly important variable in healthcare utilization.
Although QALE methods have been implemented on the outcome measures of medical care, 6,7 little research has applied this concept for assessing health impact through telemedicine. 8,9 Based on the QALE method, this study has quantified the influences of telecommunications health services on rural residents' health status. Research results fill in the void in the literature and provide assessments on the improvement in both access and health status for minority and remote citizens.
Not only public health efforts, such as sanitation and vaccination, but also medical care improved the population of concern's life expectancy and QALE over the period of 1995–2004. People living in Penghu County were less likely to see a doctor and had lower use of National Health Insurance system outpatient and inpatient care. 15,16 Telemedicine plays an important role in health improvement. However, socioeconomic factors, such as improvement in economic prosperity, increased education, less exposure to risk factors of tobacco and alcohol, good nutrition, and clean water, possibly dilute the health effect of introduction of telemedicine healthcare. Thus, our results must be interpreted with some caution.
Telemedicine has enormous potential. People living in rural areas, where it is not convenient or feasible to access a hospital, have increasing needs for telecommunications healthcare. The introduction of telemedicine system is not to replace healthcare available through traditional clinics and hospitals but to provide necessary healthcare when distance is involved. Distance often delays proper treatment for a patient in need of urgent care. 17,18
The growing population of the elderly in Taiwan and the developing as well as developed economies, coupled with increasing life expectancies, mean that there will likely be increased future demand for telemedicine to alleviate mobility problems, especially in rural areas, commonly faced by elderly individuals. This research has emphasized the influences of telemedicine provisions on the changes of QALE and the interrelationship implications of variations in survival ratios with urban and rural populations in policy-relevant forms of guidance.
Footnotes
Disclosure Statement
No competing financial interests exist.