
Abstract
Introduction
Approximately one in five U.S. adults continue to smoke. 1 Fortunately, many try to quit, 2 –4 and community-based brief cessation counseling is effective. 5 –7 Cessation programs delivered over the Internet and on cell phones have been successful. 8 –16 Text messages tailored to smoking habits and barriers to quitting have achieved high use (>50%), 17,18 encouraged quit attempts, and helped smokers cope with craving 11 –14 and relapse. 15
Multimedia, data-rich smartphones hold promise for delivery of cessation counseling. By proactively, unobtrusively, and confidentially reaching out, mobile services should gain smokers' attention quickly, deliver meaningful in-the-moment help, 19 –22 create a sense of urgency to respond, 19,20,23,24 and increase involvement in quitting. 25 Mobile applications also have the potential to mimic autonomous social support instrumental to quitting 26 –29 by creating a virtual relationship with accountability and emotional support. 20 However, in 2009, only 11% of iPhone® (Apple®, Cupertino, CA) cessation applications followed the U.S. Public Health Service's 2008 Clinical Practice Guideline for Treating Tobacco Use and Dependence; few directed smokers to effective treatments. 30 Research is needed on mobile applications that provide direct help to smokers, follow recommended guidelines, and do not simply refer to cessation services. 31
A small-scale randomized trial tested delivering cessation support over a smartphone mobile application, before embarking on a large community-based trial. The research questions explored in this pilot study were the following: (1) Would smokers use the application and rate it high on usability? (2) How many smokers receiving the application engaged in quitting, and how did use affect quitting? (3) How would the application compare with a text messaging program in usage and quitting? The mobile application was compared with a text messaging program because text messaging has been efficacious, is simpler to use, and is potentially less expensive and complicated to deploy to determine whether it is worth investing in a mobile application.
Materials and Methods
Sample
Adult U.S. smokers (n=102) 18–30 years old were recruited on Google Adwords, Facebook, and Adbrite advertising systems in 2010 (advertising cost, $47 per enrollee). Young adults should be most adept at using smartphones. Of smokers expressing interest (n=357), 187 screened by telephone were eligible (i.e., current smokers, interested in quitting, U.S. resident, and English proficient); 126 completed the consent form and pretest online, and 102 (28% of interested smokers; 54% of eligible smokers) signed a cell phone contract and were randomized (Fig. 1). Treatment effects were of primary interest, so we focused on confidence intervals (CIs): a sample of 100 would yield a two-sided 90% CI of ±0.163 for a difference in proportions of 0.40 versus 0.50 and ±0.141 for 0.20 versus 0.30.
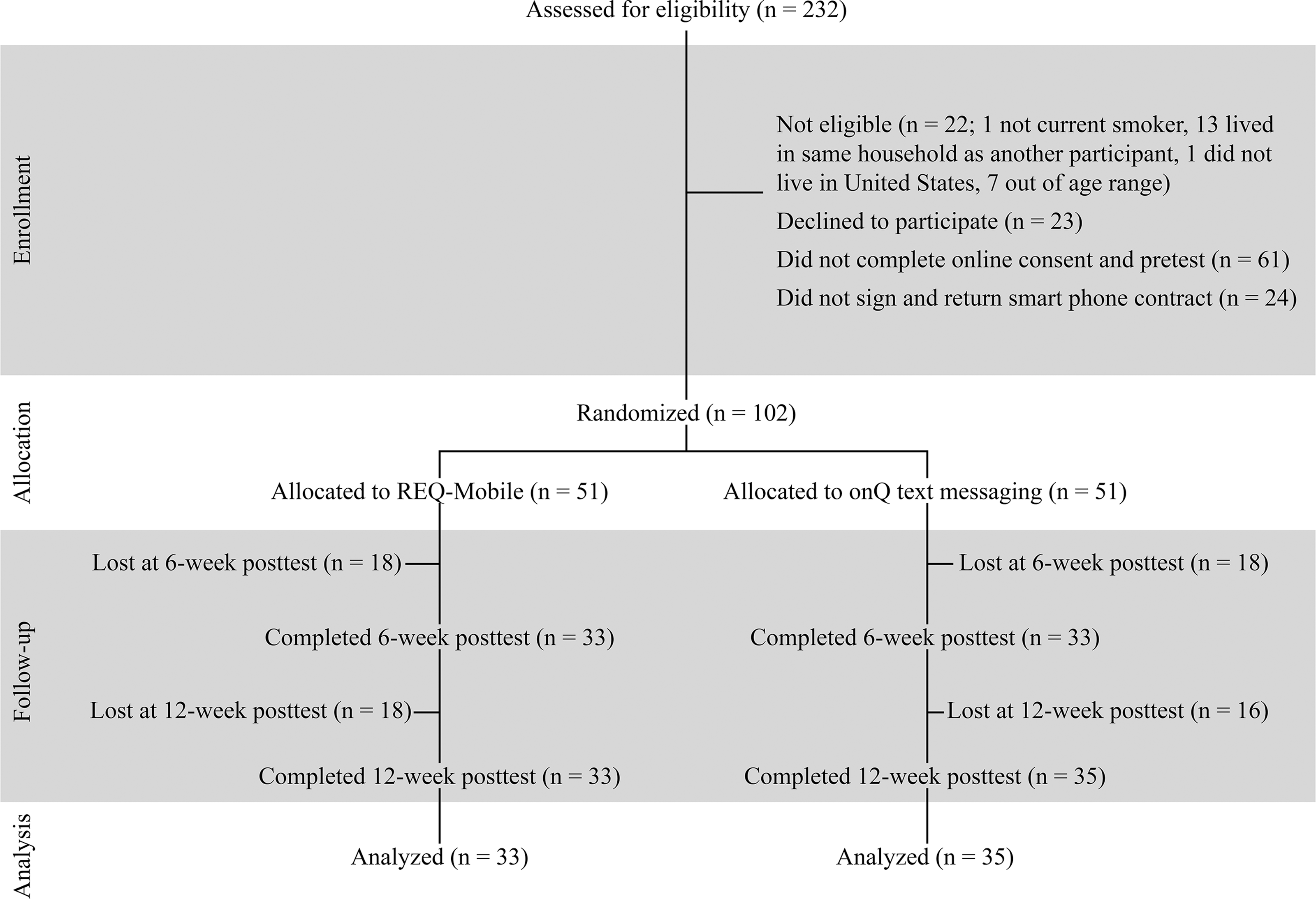
CONSORT diagram for randomized trial.
Onq Text Messaging System
The onQ text messaging system 32,33 had 1,126 messages managed by the Quit Coach expert system 34 –36 and sent to the text inbox. Messages were grounded in social cognitive theory 37 and a modified version of the transtheoretical model 38 and designed to increase/sustain motivation and enhance self-efficacy across four phases of quitting (without a quit date, with a quit date, quit for <1 week, and quit for 1–4 weeks). Messages suggested tasks to plan, set, and maintain a quit date, cope with cravings and relapse, and consolidate a nonsmoking lifestyle (see Borland et al. 32 and linked files on the journal's Web site for more details).
Real e Quit Mobile Smoking Cessation Application
The Real e Quit mobile application (REQ-Mobile) ran on Windows Mobile 6.1 or higher smartphones. When the application was produced, Android® (Google, Mountain View, CA) handsets did not exist, and Apple's policy limited the number of phones that could be used in a study. Smokers received short messages from onQ slightly revised for REQ-Mobile in an e-mail-like inbox. Audio phase-transition messages were delivered to enhance comprehension. 39 Additional features were designed to perform tasks advised in onQ messages, based on the Quit Coach theoretical framework. Smokers could create lists on (1) reasons for and (2) benefits of quitting and plans for coping with (3) challenging situations and (4) stressful circumstances, listen to 13 audio testimonials from former smokers, and read 16 short support documents (e.g., benefits of quitting, strategies for stopping, using nicotine replacement therapy [NRT], coping with withdrawal). They could set a quit date and update the expert system. The short messages directed smokers to quitting tools, and 56 messages encouraged them to use the study Web site to view additional resources on smoking cessation. Once smokers quit for more than 1 week, they were shifted to onQ because maintenance counseling was not programmed into REQ-Mobile owing to limited funds.
Two rounds of formative testing of REQ-Mobile with smokers 18–30 years old (59% female) confirmed usability. In Round 1 (n=17), 76–100% of smokers completed 11 tasks. After REQ-Mobile was revised, 90% of smokers in Round 2 (n=10) completed seven of nine tasks, and completion times decreased. In both rounds, smokers rated REQ-Mobile favorably.
Procedures
A randomized pretest–posttest two-group design was conducted in 2010–2011. After consenting online, participants completed the pretest online at the study Web site. Half were then assigned to REQ-Mobile, and half were assigned to onQ, using an online randomization program. The uniform random number generation function in SAS software (SAS Institute, Cary, NC) was used to generate random pairs assigned to treatment or control (i.e., block size of 2). Pairs were loaded into the study Web site without revealing them to the investigators and used sequentially to assign participants who completed the pretest. A smartphone with 3 months of unlimited phone, text, and data service was mailed to all study participants. If study requirements were met, smokers could keep the phone and receive a fourth month of service. Project staff explained how to use the assigned service. All participants first had to log on to Quit Coach, located on the study Web site, and complete a brief assessment, separate from the pretest, to initialize the mobile programs. Participants in both conditions could return to the study Web site to read longer tailored advice from Quit Coach and read longer support documents than were available on either onQ or REQ-Mobile. Smokers could request a free 2-week course of nicotine patches. All smokers were invited by e-mail to complete follow-up questionnaires online at 6 and 12 weeks.
Measures
Questionnaires
At pretest, 6-week posttest, and 12-week posttest, smokers reported smoking status (i.e., smoked every day or some days and 30-day prevalence), readiness to quit, nicotine dependence (i.e., cigarettes/day, time to first cigarette, and difficulty not smoking around other smokers), quit attempts in the past year, quitting self-efficacy, smoking by significant other and five closest people, and home smoking rules. At 6 and 12 weeks, continued smokers reported their likelihood of quitting in the next 6 weeks, whether they had set a quit date, and if they had tried to quit since the pretest. Participants not smoking reported how long ago they quit, if they had smoked since quitting (and if so, 7-day smoking prevalence), likelihood of smoking again, self-efficacy for staying abstinent, and use of cessation aids. Smokers assigned to REQ-Mobile and who had used it evaluated its usability at 6 weeks. 40 Nonusers were not asked about usability for they had no experience with the mobile application. Smokers provided demographics, Internet experience, use of mobile phones, and health status.
Smoking abstinence was assessed in four ways. At both posttests, point-prevalence abstinence on the day interviewed was indicated by a declaration of quitting. At 6 weeks, 7-day point-prevalence abstinence was defined as not smoking since quitting or in the past 7 days (one smoker who quit <1 week ago and not smoked since was considered abstinent). At 12 weeks, 30-day point-prevalence abstinence was defined as not smoking in the past 30 days and declaring a quit, and continuous abstinence was defined as also not smoking since quitting.
Usage
Use of REQ-Mobile and onQ was obtained from the Web servers, which recorded the number of messages sent and opened, the use of REQ-Mobile quitting tools through the first week after quitting, and number of messages sent and text responses returned to onQ.
Statistical Analysis Procedures
Comparisons between REQ-Mobile and onQ were performed by chi-squared and logistic regression in SAS software. Spearman correlations estimated the relationship of program use to quitting. Controlling for mobile phone experience and use of NRT did not change the outcomes. Effects of loss to follow-up were probed by analyzing abstinence by those completing posttests and then with all cases assuming those lost still smoked. The alpha criterion was p=0.05 (two-tailed).
Results
Profile of the Sample
Table 1 gives the sample profile. Randomization balanced groups on all demographics and pretest smoking status except income (Table 1). Most participants were successfully followed up (65% at 6 weeks; 67% at 12 weeks; 56% completed both posttests) (Table 2), with no differences in demographics (p>0.05), condition (p>0.05), or use of interventions (p>0.05). Follow-up in the REQ-Mobile group was marginally less than in the onQ group.
Demographic Characteristics and Smoking Status by Experimental Condition
Number of Participants Followed Up by Use of Mobile Smoking Cessation Services
Research Question 1: Use and Usability of Cessation Services
Overall, 60% (n=61 of 102) of smokers used the allocated service. In the REQ-Mobile group, 61% of smokers (n=31) opened the inbox, and these smokers did so an average of 26.0 times (standard. deviation [SD], 30.3), received 128.5 short messages (SD, 61.9), and opened just over 76 short messages (Table 3). Short support documents were used most, testimonials and list-making tool less, and quit date screen least. Use was highly intercorrelated (Table 3). With onQ, 59% of smokers (n=30) used the service, receiving on average 107.8 text messages (SD, 71.8; mean, 5.2 text messages sent to onQ during [SD, 3.6]). The Web server also recorded that many smokers revisited the Quit Coach program on the study Web site: revisits to the Web site, 73% (n=55 of 75; n=27 REQ-Mobile, n=28 onQ), mean of 5.2 revisits; revisits to Quit Coach, 26% (n=18 of 68; 8 REQ-Mobile, 10 onQ), mean of 2.7 revisits.
Mean Use of REQ-Mobile Application Tools, Intercorrelation (Spearman r) of Use of Various Tools, and Correlation of Tool Use with Smoking Abstinence by Smokers Allocated to the REQ-Mobile Group Who Used the Mobile Application and Completed the 12-Week Posttest (n=18)
p<0.05.
p<0.01.
Smokers who used REQ-Mobile and were followed up at 6 weeks (n=16) evaluated its usability favorably. They considered it simple (75%), reliable (75%), useful (75%), easy (69%), designed for them (69%), satisfying (69%), and easy to learn (69%). Most felt confident using it (63%), did not need help (69%), and would likely use it frequently (94%). Evaluations were less positive on REQ-Mobile being straightforward (63%), consistent (56%), and well integrated (56%). Most smokers (75%) rated it overall as user-friendly.
Quitting Behavior
Of the 63 smokers who initialized REQ-Mobile or onQ, 97% set a quit date. A majority of posttest completers reported a quit attempt at 6 weeks (53%) and 12 weeks (99%; 66% of all cases [i.e., lost=no attempt]) and declared they were abstinent (point-prevalence abstinence) at 6 weeks (53%) and 12 weeks (66%; 44% of all cases). However, 9% were struggling to maintain abstinence at 6 weeks because only 44% reported 7-day point-prevalence abstinence. At 12 weeks, 37% (25% of all cases) of smokers reported being abstinent when assessed by 30-day point-prevalence abstinence, but continuous abstinence was lower (32% completers; 22% all cases). No participant still smoking at 12 weeks reported a quit attempt (i.e., no relapsers).
Use of both services was positively correlated with quitting among completers at 12 weeks (n=68). More smokers who used either program reported 30-day point-prevalence abstinence (47%) than nonusers (20%; p=0.03; odds ratio=3.30; 95% CI 1.03, 10.56; p=0.04; use by type of service interaction p>0.05) but not continuous abstinence (used, 40%; not used, 20%; p=0.10; odds ratio=2.47; 95% CI 0.77, 7.94; p=0.13; use by type of service interaction p>0.05).
Quitting Behavior by Experimental Condition
Significantly more onQ smokers had quit at 6 weeks than REQ-Mobile smokers (Table 4). OnQ smokers were at significantly later readiness to quit phases, remained abstinent for longer, and were using NRT more compared with REQ-Mobile smokers, but these differences were less apparent at 12 weeks (Table 4).
Differences in Percentage of Smokers Quitting (95% Confidence Intervals), Readiness to Quit, Length of Time Since Quitting, and Use of Nicotine Replacement Therapy Between REQ-Mobile Application and onQ Text Messaging Conditions
Effect size was computed as h=2 arcsin(√p 1) − 2 arcsin (√p 2).
In some cases, the 95% confidence intervals for the quitting measures overlap, but the difference between conditions is statistically significant. This can occur because confidence intervals are calculated based on the subsample within a condition and are conservative, whereas the statistical test is calculated based on the larger entire sample. 72
Effect size on readiness to quit variable was estimated by converting responses to two categories: “have quit” versus all other responses combined.
Effect size on nicotine replacement therapy (NRT) variables was estimated by converting response to two categories: “more than 2 weeks” versus all other responses combined.
More frequent use of REQ-Mobile was positively associated with greater abstinence at 12 weeks (number of REQ-Mobile sessions, 30-day point-prevalence abstinence Spearman rank r=0.40, p=0.02 and continuous abstinence r=0.35, p=0.04; number of onQ text messages sent, 30-day point-prevalence abstinence r=0.28, p=0.14 and continuous abstinence r=0.31, p=0.09).
The number of times each REQ-Mobile quitting tool was used, assessed individually, was positively correlated with 12-week abstinence (Table 3). Both absolute and relative use (i.e., proportion each feature was used) showed that the list-making tool was positively correlated with success. Spending relatively more occasions listening to audio testimonials was associated with less abstinence; the positive correlation with opening short messages may be an artifact of taking longer to quit.
Discussion
This study confirmed that a smartphone mobile application could be successfully deployed and that most smokers had considerable interest in its advice. Although the sample may have been highly motivated, smokers provided highly favorable evaluations of REQ-Mobile's usability (although the subsample that used it and completed follow-up may be more favorable than nonusers or noncompleters). It was as popular as text messaging by usage. Smokers received slightly more messages from REQ-Mobile than onQ, perhaps because they took longer to quit and fewer were abstinent at 6 weeks, a finding of concern. REQ-Mobile's short messages were the most popular feature probably because they were the gateway to other features; short support documents were popular, too, perhaps because of simplicity. The less-popular list-making tool required more effort. Audio testimonials were used less, as in another study. 41
Mobile cessation services can encourage quitting. Nearly all smokers set a quit date during the study. Although the sample's selectivity may have influenced the quitting base rate, more than one in five smokers had continuously quit at 12 weeks, more than achieved in other studies, 8 –10,42,43 including text messaging. 11 –13,16 It must be pointed out that many smokers returned to use the online Quit Coach, so some of the apparent success of mobile cessation services could be due to the online content. Smokers may expect flexibility in interfaces as wireless connections and cloud computing expands mobility across devices, eliminating barriers of availability, 44 location, 45 function, 46 connection speed, and marketplace fragmentation. 47
REQ-Mobile, with added interactive features, seemed to move smokers less quickly to initiate quitting than onQ. Use of it was associated with quitting, but both could be a consequence of motivation. Unlike many existing iPhone cessation applications, 30 REQ-Mobile was built on theoretical models 34 –36 and directed smokers to use effective treatments. 48 –55 Its continuous, real-time, mobile nature 19,56 should have integrated cessation support into smokers' communication environments more than other cessation services (e.g., group sessions, telephone, Web site) when and where they need it. This could have increased involvement with the counseling and quitting, 19,20,23 –25 and provided social support for quitting. 20,26 –29
Even with the seemingly apparent advantages of mobile applications, the onQ program appeared to produce more successful quitting, a finding that needs further exploration. The most plausible explanation is simplicity. Smokers are often ambivalent about their smoking and quitting, 57 so are easily discouraged or distracted from making quit attempts. Simplicity predicts adopting new products 58 and complexity interfered with another mobile cessation program. 15 It should be noted that REQ-Mobile smokers were switched to onQ messages after having quit for 1 week (because of lack of project funds for programming this phase), which may explain why this superiority of onQ declined from the 6-week to 12-week follow-up. It is also possible that smokers were new to smartphones and mastered them over time, improving REQ-Mobile's impact at 12 weeks. Furthermore, smokers may have monitored their text inbox, where onQ messages were sent, more routinely than REQ-Mobile's private inbox. The free phone provided to all participants may have been a second phone for some smokers. Thus, smokers needed to monitor two inboxes, an extra step that may have allowed them to ignore messages and read them in batches (76 messages were opened in 26 REQ-Mobile sessions). However, REQ-Mobile (but not onQ) displayed a notice on the main screen every 15 min when its inbox contained unread messages to prompt more immediate reading, but integrating REQ-Mobile's inbox with the normal text messaging inbox might be improve it. Thus, quitting trajectories should be tracked when studying mobile technologies. Less plausible is that the difference could have arisen because randomization failed or groups were nonequivalent on income.
Some components of REQ-Mobile seemed to support quitting more than others. Theoretically, the list-making tool should have enhanced motivation and self-efficacy for quitting, but more motivated smokers may have been most willing to use it. What combination of content, involvement, and motivation makes any tool effective needs further exploration. Setting a quit date can be an important step toward initiating a quit. 59 Some smokers spontaneously, successfully quit, 60,61 but this may be less common among younger smokers. 62 Audio testimonials did not appear useful, perhaps because their content was inappropriate or they distracted smokers from other important tasks. They might be eliminated to simplify the mobile application. This suggests caution when considering using social media, which is dominated by user-generated content, for they may divert smokers from more useful cessation content.
This study had several strengths and limitations. Strengths included recruiting smokers throughout the United States and balancing differences with randomization. However, the small sample limited statistical power. Self-reported abstinence is over-reported, 63 –65 but randomization to two active interventions should have equalized this bias. Prescreening and free phones may have recruited highly motivated smokers, limiting generalizability to populations such as quit line callers, or for free stuff (although the high quit rates suggest this is unlikely).
Mobile applications may be effective for brief community-based smoking cessation, as smartphone ownership increases (half of U.S. mobile phone users use applications 66,67 ). Future efforts are needed on how to direct smokers to use applications, 31 a challenge for all cessation counseling. 5,7,15,68 –71
Footnotes
Acknowledgments
This project was supported by grant CA107444 from the National Cancer Institute.
Disclosure Statement
D.B.B. is an employee of Klein Buendel, Inc, a for-profit company. D.B.B.'s spouse is the sole owner and President of Klein Buendel. D.B.B. is a member of Wedge Communications LLC, a technology transfer company that has licensed the REQ-Mobile mobile application. R.B. was responsible for developing the onQ and Quit Coach programs, but he holds no commercial interest in them. E.P.B. is an employee of Klein Buendel, Inc., and a member of Wedge Communications LLC. J.H.S. is an employee of Klein Buendel, Inc. D.E.Z. has no competing financial interests.