
Abstract
Introduction
Telemedicine may help to improve access to care and treatment in elderly populations with chronic disease by providing guidance from health professionals at a distance. 1 The European Commission has recognized the potential of telemedicine for monitoring patients from their homes in the management of chronic obstructive pulmonary disease (COPD). 2
In addition, the demand for telemedicine solutions has increased, and patients may be more involved in their own treatment and thus take on a higher degree of self-management. 3 Systematic reviews have concluded that telemedicine may have an effect on the COPD patient's health-related quality of life 4 and the number of times patients attend the emergency department or hospital. 5
The current literature has not yet considered the importance of cognitive function in patients with COPD who receive telemedicine. 4,6 However, it is important to take differences in cognitive ability into account, as there is evidence that cognitive dysfunction may be a limitation in patients with severe COPD. 7 A systematic review concluded that cognitive function, especially memory and attention, is more impaired in these patients than in healthy controls, 8 and patients must understand simple instructions and be able to transform these instructions into concrete actions in order to benefit from telemedicine concepts.
In contrast, telemedicine-based treatment may offer some advantages over hospital admission. A hospital environment may cause cognitive decline, especially in elderly patients. A longitudinal population-based cohort study involving 1,870 elderly people concluded that in old age, cognitive functioning tends to decline substantially after hospitalization, even after controlling for severity of illness and cognitive decline prior to hospitalization. 9 Thus, telemedicine-based treatment in COPD patients' own homes may be associated with less impairment of cognitive function because hospitalization is avoided.
To our knowledge, the present study is the first to investigate whether cognitive performance in patients with severe COPD and a mild to moderate exacerbation is better after telemedicine-based treatment (virtual admission) than after conventional hospital admission.
Materials and Methods
Design of the Trial
This study was a substudy of the multicenter, randomized clinical trial the “Virtual Hospital,” which was conducted in Denmark from 2010 to 2012. Data from the larger study will be reported later elsewhere.
Participants
The Virtual Hospital study included patients admitted to a medical emergency department with COPD with exacerbation. Within 24 h, patients were randomized to continued treatment either in their own home using a telemedicine solution or in the hospital.
Patients were included if they gave informed consent, were at least 45 years of age, met the criterion of Global Initiative for Chronic Obstructive Lung Disease stages 3–4, 10 had an arterial pH of ≥7.35, could communicate and understand simple instructions, and could manage the devices and the telemedicine technology and it was estimated that they would require hospitalization for more than 2 days.
Patients were excluded if they had a need for noninvasive ventilation or treatment using a ventilator at the time of randomization, were severely obese (Pickwick's syndrome or immobility due to severe overweight), had other serious comorbidity such as unstable heart disease, diabetes, or known malignant disease, were noncompliant, had a temperature of >38°C, and/or had a need for intravenous antibiotics and if they were unable to give informed consent.
For the present substudy, patients were consecutively recruited from the Virtual Hospital study but with the following additional exclusion criteria: Mini Mental State Examination (MMSE) score below 24 points, current severe psychiatric disease, neuropsychological testing in the previous year, illiteracy, poor comprehension of Danish, severe visual or auditory disorder, or unwillingness to complete the follow-up.
Study Settings
The study took place at Frederiksberg University Hospital and Herlev University Hospital. It was approved by the appropriate ethics committee.
Randomization
After giving their written consent, patients were randomized using a computer-generated list of random numbers placed in numbered, sealed, and opaque envelopes so that the allocation sequence was concealed from the researcher. Patients were randomized 1:1 to the intervention group or the control group, using fixed random block sizes of 4 because of the number of patient computers available.
Intervention Group
Within the first 24 h of hospitalization, patients randomized to telemedicine treatment were trained in a secure environment to ensure that they were able to use the telemedicine equipment before leaving the hospital. Patients in the intervention group had to measure their own vital parameters and take the prescribed medicine.
First, a hands-on training session was held following a fixed education plan. This would allow the patient to become familiarized with and learn how to use the videoconferencing system and how to operate the medical equipment in case of an emergency situation. A health professional and a technician accompanied the patient home in order to install the telemedicine equipment. Second, a full retest took place in the patient's home to ensure that he or she was able to manage the videoconferencing system and the other devices correctly. The telemedicine equipment consisted of a touch screen (PC) and additional devices (pulse oximeter, spirometer, and thermometer) for monitoring of vital parameters. The patient was also provided with an oxygen condenser, a nebulizer, and medicine (antibiotics, prednisolone, bronchodilating agents [beta-2 agonist], and anxiolytics).
A user-friendly interface had been developed in order to minimize complications, and a finger touch on the screen immediately connected the patient to a 24/7/365 call center organized by the hospital. Daily ward rounds were performed by a physician in the call center. The telemedicine equipment and devices were removed on the day of discharge. Discharge criteria were at least 4 h of uninterrupted sleep during the night, no decrease in forced expiratory volume in 1 s (FEV1), hemoglobin oxygen saturation (SAT) >90% without oxygen or with usual oxygen supply, clinically stable, and improved condition during the period of admission.
Control Group
Patients in the control group stayed in the hospital until the discharge criteria were fulfilled, and they received the same medical treatment as the intervention group, according to existing guidelines for treatment of acute exacerbation. 10 The pharmacological treatment, the oxygen therapy, the daily ward round with a physician, and the opportunity to contact healthcare professionals 24 h/day were the same in both groups during the period of admission.
Data Collection and Follow-Up
Because of the patients' poor condition during an acute exacerbation, we were not able to assess our primary outcome (cognitive function) before the condition had stabilized. Cognitive function was therefore assessed in both groups 3 days after discharge and at follow-up 6 weeks after discharge.
Cognitive Outcome
Neuropsychological test batteries consist of many single tests, each giving several variables, either scores or time measurements. There is a distinct lack of information on the strategies for screening for cognitive impairment in patients with COPD, but memory and attention, and also speed, coordination, and learning abilities, are variables known to be reduced in COPD patients. 7,8 However, when we initiated this study, it was necessary to decide which variables should be considered for evaluation of cognitive function in patients with COPD. We therefore chose the International Study of Post-Operative Cognitive Dysfunction (ISPOCD) test battery, which includes the above variables. The ISPOCD test battery had already been translated into Danish and validated for sensitivity in elderly Danish patients undergoing surgery. 11 High test–retest reliability coefficients have been obtained, and the learning effects are minimized because the test exists in two parallel versions. 12
The battery comprised the following tests: (A) the Visual Verbal Learning Test, based on Rey's auditive recall of words, was used for assessment of memory 13 ; (B) the Concept Shifting Task, based on the Trail-Making Test from the neuropsychological test battery of Halstead and Reitan, consisted of three subtests measuring cognitive speed and flexibility 14 (time to complete Part C and the number of errors were recorded); (C) the Stroop Color Word Interference Test, which measures attention and cognitive speed under simple and complex conditions 15 (we recorded the time and number of errors made in Part 3); and (D) the Letter-Digit Coding, based on the Symbol Digit Substitution task in the Wechsler Adult Intelligence Scale. 16 The sessions were done in the patient's home, and only the patient and investigator were present. Each test was performed in a standardized way by the Principal Investigator, who was trained to conduct the test. Parallel versions of the tests were used after 6 weeks.
Sample Size
We considered 13 s to be a relevant difference in the time taken for Part 3 of the Stroop Color Word Test because this was the difference detected between healthy controls and a population of elderly individuals 1 week after surgery. 17 The standard deviation (SD) was estimated to be 20 s. Based on these results, we calculated that 120 patients should be included in the analysis for a 15% risk of a type-II error (with a significance level of 0.01 and 85% power). With an expected dropout rate of 20%, the total number of patients enrolled should be 150.
Statistical Methods
For assessment of the primary outcome (cognitive function), the performance in the cognitive tests was compared between the intervention group and the control group 3 days after admission, according to the seven test variables with correction for multiple comparisons. Continuous data were compared with t test or Mann–Whitney rank-sum test as appropriate. Probability values <0.05 were considered to be statistically significant. All subjects were analyzed in the groups to which they were randomly allocated according to intention-to-treat analysis. In supplementary analyses, we investigated changes in cognitive function from 3 days to 6 weeks after discharge. For assessment of correlation between sociodemographic data and cognitive test results in the total study population 3 days after admission, Spearman's rank test was used. All data management and analyses were performed with Statistical Package for the Social Sciences (SPSS) software version 19.0 (IBM, Armonk, NY).
Definition of Cognitive Dysfunction
In the literature, there is a lack of consensus regarding the definition of cognitive dysfunction in COPD patients. The studies included in two systematic reviews 7,8 had a large variation in the batteries of cognitive tests used but lacked a clear and explicit definition of dysfunction that is appropriate for patients with COPD. We chose a definition used in a former study investigating older Danish patients undergoing surgery, which was based on the ISPOCD test battery by Jensen et al. 18(p. 2791) Cognitive dysfunction was defined as the occurrence of at least two of seven possible deficits. The seven possible deficits were two possible deficits in each of tests A, B, and C and one possible deficit in test D (see section above on Cognitive outcome).
For the two error scores, a deficit was defined in our study as four or more additional errors out of 16 possible in test B and five or more additional errors out of 40 possible in test C (Part 3). For the remaining five variables, a deficit was defined as 40% deterioration. We compared the result obtained 3 days after discharge (after exacerbation) with the result at 6 weeks, assuming that the performance at 6 weeks represented baseline performance when the patient's lung function had recovered.
Results
Patient Population and Allocation
Between June 15, 2010 and January 30, 2012, 647 consecutive patients admitted to the hospital with a respiratory diagnosis were assessed for the “Virtual Hospital” trial. In total, 424 patients had a main or secondary diagnosis of COPD; of these, 117 met the inclusion criteria. Fifty-nine patients (50%) refused to participate: 22 patients gave no reason, 10 patients refused because of anxiety because of their acute condition with an exacerbation, 16 patients were too tired and needed assistance with physical care and feeding, 6 patients did not want to participate because they were anxious about the telemedicine concept or because it made them feel stigmatized, and 3 patients did not want to participate for other reasons. In total, 58 patients (50%) agreed to participate in the “Virtual Hospital” trial and were randomized. Of these 58 patients, 5 were excluded because they had an MMSE score of less than 24 points, 3 refused to participate in this substudy, and 6 were excluded for other reasons. Thus, 44 patients were included in the present study: 22 in the intervention group and 22 in the control group (Fig. 1).
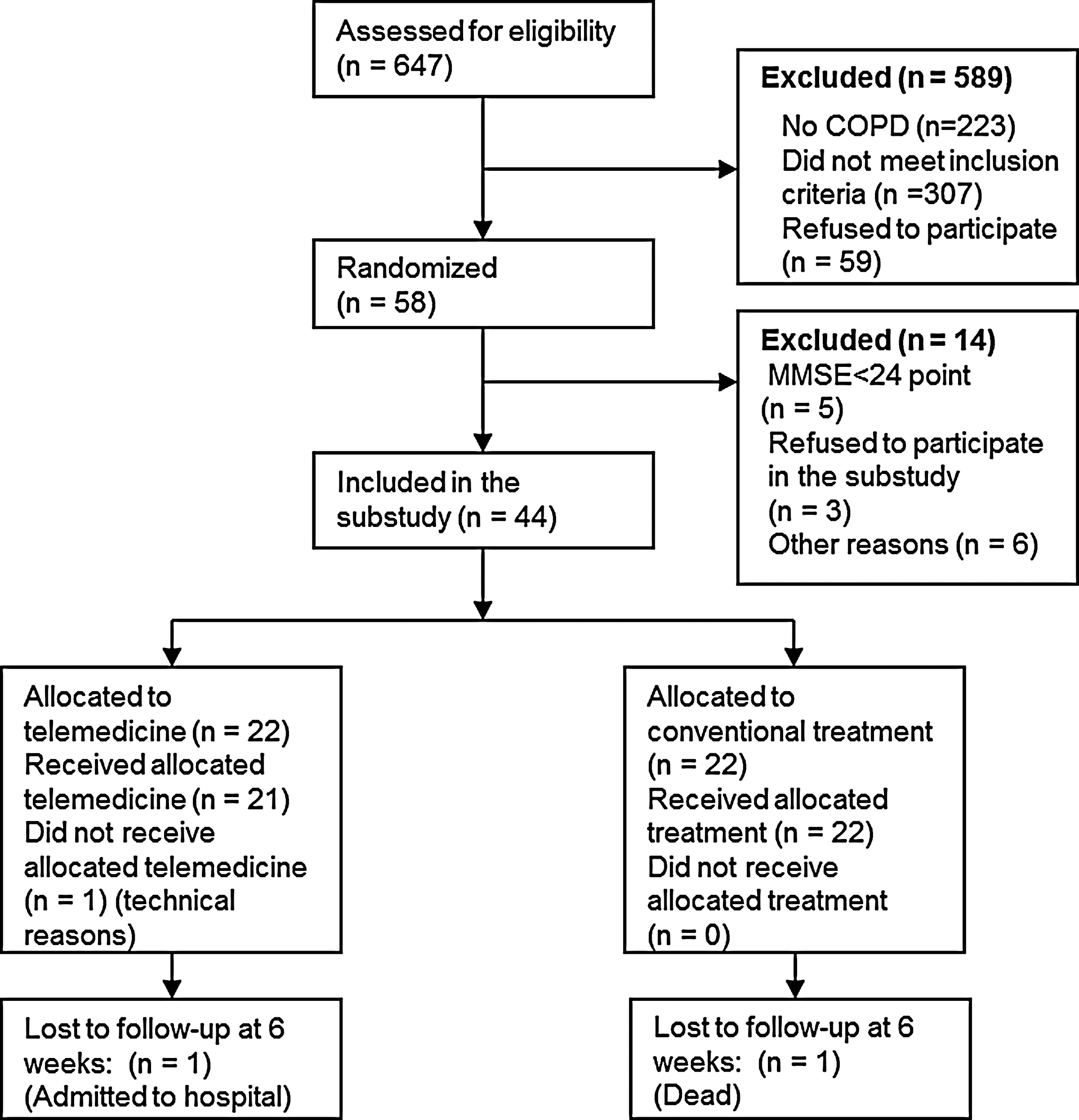
Flow diagram. COPD, chronic obstructive pulmonary disease; MMSE, Mini Mental State Examination.
According to the protocol of the Virtual Hospital, the 22 patients in the intervention group should be admitted to their own home within 24 h. The actual mean time from admission until return home was 21.19 (SD 6.64) h.
Patients in the intervention group tended to be younger and had a significantly higher MMSE score, whereas a higher number of patients in the control group had 10 years of basic schooling and education at the university level (Table 1).
Baseline Demographic and Clinical Characteristics
FEV1, forced expiratory volume in 1 s; MMSE, Mini Mental State Examination; SAT, hemoglobin oxygen saturation.
After 6 weeks, FEV1 had improved in both groups to 1.2 L in the intervention group (p=0.05) and 1.0 L in the control group (difference nonsignificant). SAT had improved in the intervention group from 94% to 96% (p=0.001). There was no change in SAT in the control group.
Losses and Exclusions
There was only one deviation from the protocol. Because of technical problems with the telemedicine equipment, we had to keep 1 patient in the hospital, and this patient did not receive the intervention. According to the intention-to-treat principle, we analyzed the patient in the intervention group. At follow-up after 6 weeks, cognitive outcome could be determined in 21 patients in both groups (Fig. 1).
The 59 patients who did not wish to participate in this study were not significantly different from the enrolled patients regarding age (71 [SD 9.2] years versus 70 [SD 10.6] years) and percentage predicted FEV1 (30% [SD 11.6%] versus 33% [SD 12.5%]). However, a much higher proportion of women than men declined participation (81%), whereas the proportion of women who participated was 59%.
Cognitive Outcome
Patients in both groups were tested approximately 3–4 days after discharge (i.e., on average 9 days after admission [p=0.93]; mean, 8.8 [SD 1.3] days in the intervention group and 8.9 [SD 1.7] days in the control group). The mean time elapsed at the 6-week follow-up was 49 (SD 7) days for the intervention group and 47 (SD 7.9) days for the control group (p=0.46).
The performance in all seven neuropsychological test variables (Table 2) tended to be better in the intervention group allocated to virtual admission both 3 days and 6 weeks after discharge, but the difference was not statistically significant (even less after Bonferroni's correction for multiple comparisons).
Outcome in Patients Undergoing Virtual Admission Versus Conventional Hospital Treatment
Data are mean (standard deviation) values.
p values were calculated with the Mann–Whitney rank-sum test.
When we applied our definition of at least two of seven possible deficits, compared with follow-up at 6 weeks, 9 patients (40%) in the intervention group and 9 patients (40%) in the control group had cognitive dysfunction 3 days after discharge. We found that there was a significant correlation between age and four out of seven variables in the cognitive test battery, but there was no significant correlation between the cognitive test variables and FEV1, percentage predicted FEV1, SAT, or MMSE (Table 3).
Correlation Between Sociodemographic Data and Cognitive Test Results in the Total Study Population 3 Days After Admission (n=44)
Data are Spearman's rank correlation coefficient (p value).
FEV1, forced expiratory volume in 1 s; MMSE, Mini Mental State Examination; SAT, hemoglobin oxygen saturation.
Discussion
Our objective was to investigate whether cognitive performance is better after telemedicine-based treatment than after hospitalization in patients with severe COPD and exacerbation. There were no significant differences in cognitive performance between the groups, and there were signs of improvement in both groups from 3 days to 6 weeks, but none of the improvements was significant. However, 40% of our patients in both groups had cognitive dysfunction after exacerbation, which is four times higher than in a study using the same definition in elderly high-risk patients 12 weeks after coronary artery bypass grafting (9.8%). 18 When comparing with another study, 19 investigating cognitive function in a healthy elderly population, with a mean age of 70 years, patients with severe COPD and exacerbation had inferior performance in all the cognitive tests used.
The high incidence of cognitive dysfunction after exacerbation could be related to low SAT, and an association has been found between severity of COPD and cognitive dysfunction in patients with severe COPD. 8 In the present study, we found no significant correlation between SAT and cognitive test results (Table 3). This may be explained by the high values of SAT seen in both groups at the time of testing (Table 1).
The patients in the intervention group tended to be younger than those in the control group, and there was a correlation between age and four out of seven cognitive tests. This may explain why outcome tended to be better in the intervention group (Table 3).
Patients with an MMSE score of <24 points were excluded from this substudy, and the intervention group had a higher MMSE score than the control group, but we found no significant correlations between MMSE score and cognitive test results in our population, with a mean MMSE score of 28 points (Table 3). Self-management increases COPD patients' involvement in their disease, 20,21 and patients in a home telecare system may be empowered to perform better self-care, 22 but we should be aware of the challenges faced by an older pretechnological population such as elderly COPD patients. 4 Sanders et al. 23 recommended more detailed information and time for discussion on introduction to telehealth, in order to give patients the opportunity to discuss their expectations.
Sources of Bias
The present study had a high degree of internal validity in terms of patient selection and the number of patients who were available for follow-up; only 1 patient was lost from each group. However, some limitations should be taken into consideration. The inclusion rate was lower than predicted; 50% of the patients refused to participate, but we decided that the inclusion would be time-driven and would continue until the planned 18 months of inclusion had ended. We only succeed in including 44 patients. Thus, there is a substantial risk of type-II error, and the present study must be regarded as being preliminary.
It must also be acknowledged that neither the patients nor the tester was blinded, and the patients in the virtual group may have achieved better performance in the tests because of a Hawthorne effect, whereby subjects improve or modify an aspect of their behavior that is being experimentally measured simply in response to the fact that they know they are being studied. 24 In addition, a practice effect from repeated testing within a short period of time could have affected the test results in both groups. 19
Cognitive dysfunction may be of limited clinical importance, and the ability to carry out activities of daily living is not well assessed during neuropsychological testing. This is because there still is a distinct lack of information on the strategies for screening for cognitive impairment in patients with COPD and also for patients included in a telemedicine set-up with a high degree of self-management. Therefore, there is some uncertainty as to whether the selected test measures were relevant for these patients, and this could probably explain why we did not find any correlation between neuropsychological tests result and the patients' health-related quality of life in telemedicine-based treatment groups. 25
Conclusions
There were no significant differences in cognitive performance between the telemedicine-based group and the conventional hospital group. Patients with severe COPD suffering from mild to moderate exacerbations were able to manage the telemedicine-based treatment despite the reduced cognitive function often seen in COPD patients. However, practitioners operating with telemedicine solutions should be aware of COPD patients' reduced cognitive function when considering solutions with a high degree of self-management.
Footnotes
Acknowledgments
This study was supported financially by the Tryg Foundation and the Health Insurance Foundation, both of which are noncommercial.
Disclosure Statement
No competing financial interests exist.