
Abstract
Introduction
Chronic disease is an increasingly important issue for individuals and healthcare organizations across Canada. The economic and social challenges of managing complex chronic diseases are substantial and becoming steadily more pressing. 1 These problems are especially profound in remote, rural, and small urban areas, where hospitalization and mortality rates tend to be higher. 2 There are many determinants of health, and this discrepancy cannot be attributed to a single cause. However, lack of access to health services is generally recognized as a contributing factor. The ongoing shortage of health human resources in rural and remote regions forces patients to travel long distances to access care, the challenge of which may be compounded by inclement weather and limited mobility. 3
One way of improving access to care is through “telehealth”: “[…] the use of secure information and communications technologies […] to deliver healthcare.” 4 In some regions, home telehealth has attained widespread use for chronic disease management; the United States, for instance, has introduced a national program for Veterans. 5 Examples of home telehealth include remote monitoring systems, self-management applications for mobile devices, and videoconferenced medical appointments. Enabling patients to access care from home has the potential to improve health outcomes, reduce healthcare costs, and support patient self-management. 3
Home telehealth has been promoted at both the federal and provincial levels as a strategy for managing the anticipated challenges to the healthcare system that will accompany an aging population. 6 Achieving equitable and accessible home-based healthcare was identified as a key priority for Canada at the turn of the millennium. 6 High-quality research is needed to determine the extent to which telehealth can facilitate these goals. It is equally important to ensure that the information gained through this research is accessible to policy makers and other knowledge users.
To this end, we conducted a narrative synthesis of the literature on home telehealth for chronic disease management. A team of policy makers, managers, and practitioners was involved in defining the scope of evidence and type of information required for practical and informed decision-making. In this article, we focus on one of four broad research questions that guided the review: “What is the evidence on the effectiveness of home telehealth in chronic disease management?”
Materials and Methods
Composition of the Review Team
The review team included both researchers and “knowledge users,” including representatives of several British Columbia health authorities. These individuals were active in defining research priorities and providing consultation to the researchers. Their contributions to the review team ensured that research remained accessible and relevant to policy makers and others with direct involvement in healthcare planning and delivery.
Defining the Study Question
The term “chronic disease” encompasses a vast range of conditions. In order to reduce heterogeneity and increase the usefulness of this research to knowledge users, we limited our literature search to six chronic diseases selected by knowledge users in early meetings: asthma, cardiovascular disease, chronic obstructive pulmonary disease, diabetes, renal disease, and stroke. These conditions were identified as especially relevant to provincial health priorities. However, we recognize that our use of these diseases to represent chronic disease in its entirety may limit the applicability of our findings. The exclusion of arthritis, mental health disorders, and hypertension may be particularly controversial (here they were excluded except where comorbid with one of the six previously named conditions). The precise reasons for omitting these conditions from our analysis—a decision that entailed prolonged debate—varied. A common factor, however, was their perceived dissimilarity with the other target conditions in regard to management needs, pathophysiology, and/or structure of care delivery services.
For the purposes of this project, “telehealth” was defined as ‘the use of information and communications technologies to deliver health services and transmit health information over both long and short distances.” Examples of such information and communications technologies include videoconferencing, Web conferencing, text messaging, and digital image transmission. Consultation with our knowledge users led us to exclude interventions that used only stationary telephones.
Database Searches
The review team worked with a qualified and experienced health librarian to develop a search strategy. The EMBASE, Medline, CINAHL, Web of Science, and PAIS databases were searched for material relevant to the priority research questions and with a focus on one of the chronic diseases listed above. The search was built around three concepts: home telehealth, chronic disease, and economics. The exact search terms used differed in each database in order to take full advantage of variations in indexing methods. Searches excluded material in languages other than English or French and were restricted to the time period 2005–2010. Academic publications, white papers, and gray literature were all considered eligible for inclusion, provided an original research element was present. Systematic reviews were also included. Case studies, technology reviews, and articles without abstracts were excluded. Full details of the search strategy can be obtained from the authors upon request.
Critical Appraisal
The research team categorized studies according to the Oxford Centre for Evidence-Based Medicine (OCEBM) 2011 levels of evidence. (For a comprehensive overview of this system, please refer to Howick et al. 7 ) In this system, studies are classified as Level 1–5 according to their ability to provide “the likely best evidence.” 7 Level 1 and Level 5 studies were excluded from this review through our original screening process. All remaining studies were therefore Level 2 (individual randomized trial), Level 3 (nonrandomized controlled cohort/follow-up study), or Level 4 (case-series, case-control studies, or historically controlled studies).
The OCEBM Levels were used in conjunction with an instrument to assess quality of execution and reporting (Appendix 1). This instrument was developed by the research team but drew on the framework presented in Zaza et al., 8 although time and resource limitations necessitated a more abbreviated process. Sampling method, dropout rates, blinding, and interpretation of data were among the criteria considered. A study was downgraded one OCEBM level if it received a “weak” (≤3) execution/reporting score. This practice is sanctioned by the Oxford Level guidelines.
Data Extraction
In the first stage of screening, studies were classified as qualitative, quantitative/mixed methods, or systematic review. A different review process was used for each subgroup of results. Systematic reviews were retained for reference purposes but not subjected to systematic data extraction. Qualitative studies were reviewed for information on patient and provider experiences. This information was summarized through thematic analysis. A standardized coding sheet (Appendix 2) for use with articles on quantitative and mixed-methods studies was developed after preliminary review of the evidence. Information extracted included data on population characteristics, intervention design, clinical and economic outcomes, and patient and provider experiences.
Results
Scope of Literature
In total, 34,353 references were retrieved by the literature search. After removal of duplicates, citations without abstracts, and documents with no apparent relevance to the research questions, 1,075 articles remained. One hundred eighty-six of these articles (representing 147 discrete studies) met our inclusion criteria and were reviewed in detail (Fig. 1). In this article, discussion is limited to the 137 quantitative and mixed-methods studies. All subsequent analyses (percentages, etc.) are based on this subset.
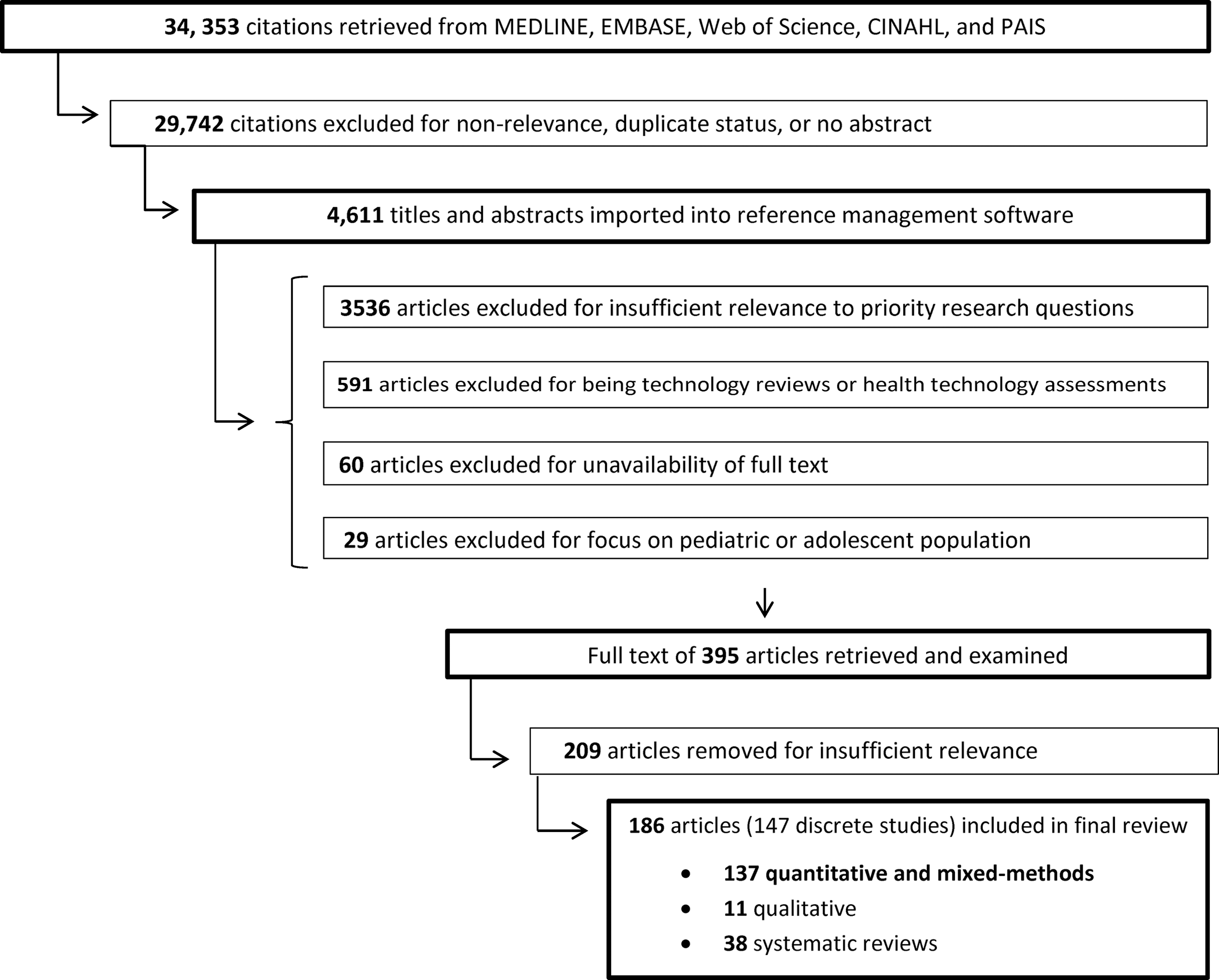
Search process.
Strength of the Evidence
Eighty-seven articles (64%) were classified as OCEBM Level 2, 16 as Level 3 (12%), and 34 as Level 4 (25%). Nineteen articles were subsequently downgraded a level for low execution/reporting scores. Most articles received an execution/reporting rating of strong (29 articles) or moderate (89 articles). The subgroups of studies of asthma, heart failure, and type 2 diabetes were consistently well executed and reported; the percentages of articles within these subgroups that were given strong or moderate ratings were 100%, 93%, and 90%, respectively.
Studies showed considerable variation in length and sample size. Duration ranged from 0.5 to 84 months, with 6- and 12-month durations the most common. Size of sample ranged from 7 to 6,184, with a mean of 268 and a median of 101. (Calculations are based on the number of participants included in the final analysis. When this number was not available [11 instances], the number enrolled was used. When multiple publications reported different outcomes for the same sample, the sample was counted once.) The largest studies were found in the type 2 diabetes and cardiovascular disease subgroups (mean sample sizes of 406 and 256, respectively).
Distribution by Chronic Disease
The majority of the literature focused on populations with type 2 diabetes or cardiovascular disease (particularly heart failure). These disease categories were further broken down when it became apparent that they included at least two subgroups of populations with distinct management needs (type 1 versus type 2 diabetes and heart failure versus coronary artery disease, respectively). There was a notable dearth of studies on renal disease patients (Fig. 2).
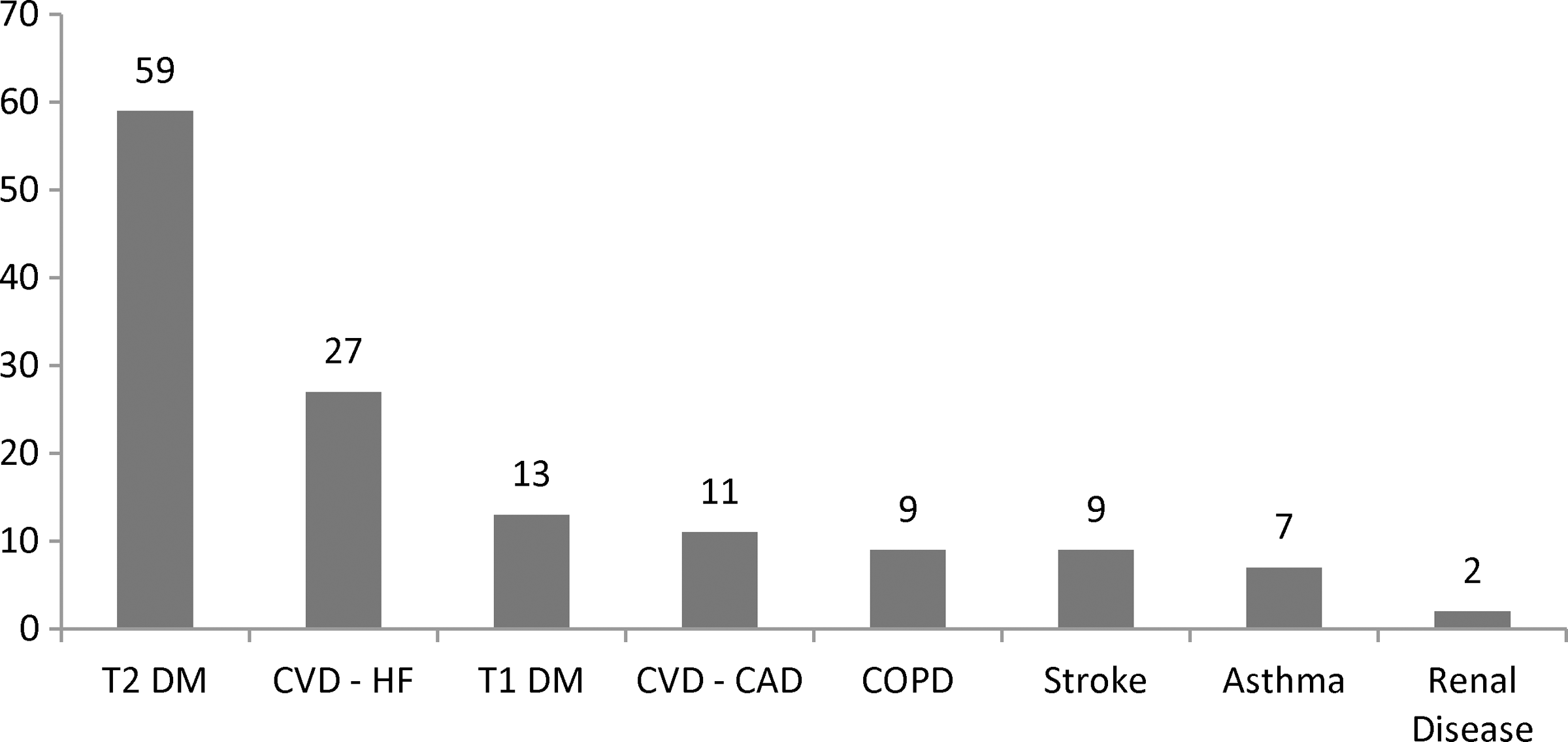
Articles retrieved. COPD, chronic obstructive pulmonary disease; CVD-CAD, cardiovascular disease (coronary artery disease); CVD-HF, cardiovascular disease (heart failure); T1 DM, type 1 diabetes mellitus; T2 DM, type 2 diabetes mellitus.
Outcomes
We collected data on patient outcomes, provider outcomes, and system outcomes. In this publication, we focus on patient outcomes: disease state, quality of life, and/or symptoms. Tables 1 –7 give a complete list of the 101 articles that reported these outcomes.
Asthma: Effects of Home Telehealth on Symptoms, Quality of Life, and Disease State
Age is given in years. A checkmark designates that the p value was not reported.
ACT, Asthma Control Test; AQLQ, Asthma Quality of Life Questionnaire; FEV1, forced expiratory volume in 1 s; NA, not applicable because of lack of control group (CG) or chosen measure; NR, not reported; OCEBM, Oxford Centre for Evidence-Based Medicine; SD, standard deviation; Sig Diff, significant difference between groups; Sig Eff, significant effect in telehealth group (TG).
Cardiovascular Disease (Coronary Artery Disease): Effects of Home Telehealth on Symptoms, Quality of Life, and Disease State
No symptoms outcomes were reported. Age is given in years. A checkmark designates that the p value was not reported.
Physical subscale mean scores only.
“The evaluation of parameters reflecting quality of life (MOS/SF-36) showed no modification in 8/15 patients and an improvement in 2/15 patients in group B, while there was a worsening in 7/15 patients and an improvement in 1 patient in group C (p<0.05).” 21 ,p.9
ECG, electrocardiogram; EuroQoL, a standardized instrument used to measure health-related quality of life; HADS, Hospital Anxiety and Depression Score; ICD, implantable cardioverter-defibrillator; MOS SF-36, Medical Outcomes Study Short Form Health Survey (12-item/36-item); NA, not applicable due to lack of control group (CG) or chosen measure; NR, not reported; OCEBM, Oxford Centre for Evidence-Based Medicine; SD, standard deviation; Sig Diff, significant difference between groups; Sig Eff, significant effect in telehealth group (TG).
Cardiovascular Disease (Heart Failure): Effects of Home Telehealth on Symptoms, Quality of Life, and Disease State
Age is given in years. A checkmark designates that the p value was not reported.
Improvement in diet and medication symptoms only.
For one of eight subscales.
Bodily pain and vitality subscales only.
For 8 of 21 items.
For 2 of 12 items.
ECG, electrocardiogram; EHR, electronic health record; EuroQoL EQ-5D, a standardized instrument used to measure health-related quality of life; HFSDS, Heart Failure Symptom Distress Scale; KCCQ, Kansas City Quality of Life Questionnaire; MLHFQ, Minnesota Living With Heart Failure Questionnaire; MLQ, Minnesota Living Questionnaire; NA, not applicable due to lack of control group (CG) or chosen measure; NR, not reported; NYHA, New York Heart Association; OCEBM, Oxford Centre for Evidence-Based Medicine; SD, standard deviation; SF-12, 12-item Short Form; SF-36, 36-item Short Form; Sig Diff, significant difference between groups; Sig Eff, significant effect in telehealth group (TG); SPRS, System Problem Rating Scale; VO2, volume of O2.
Chronic Obstructive Pulmonary Disease: Effects of Home Telehealth on Symptoms, Quality of Life, and Disease State
Age is given in years. A checkmark designates that the p value was not reported.
On seven of eight subscales. Scores were significantly lower in the telehealth group (TG) on the General Health subscale when controlling for key variables.
CCQ, Clinical Chronic Obstructive Pulmonary Disease Questionnaire; EuroQoL EQ-5D, a standardized instrument used to measure health-related quality of life; FEV1, forced expiratory volume in 1 s; HADS, Hospital Anxiety and Depression Score; NA, not applicable because of lack of control group (CG) or chosen measure; NR, not reported; OCEBM, Oxford Centre for Evidence-Based Medicine; RPE, Rating of Perceived Exertion; SD, standard deviation; SF-36, 36-item Short Form; Sig Diff, significant difference between groups; Sig Eff, significant effect in TG; SGRQ, St. George's Respiratory Questionnaire.
Diabetes (Type 1): Effects of Home Telehealth on Symptoms, Quality of Life, and Disease State
No symptoms outcomes were reported. Age is given in years. A checkmark in parentheses designates that the p value was not reported.
For four of eight subscales.
DQLQ, Diabetes Quality of Life Questionnaire; HbA1c, glycated hemoglobin; NA, not applicable because of lack of control group (CG) or chosen measure; NR, not reported; OCEBM, Oxford Centre for Evidence-Based Medicine; SD, standard deviation; SF-12, 12-item Short Form; SF-36, 36-item Short Form; Sig Diff, significant difference between groups; Sig Eff, significant effect in the telehealth group (TG).
Diabetes (Type 2): Effects of Home Telehealth on Symptoms, Quality of Life, and Disease State
Age is given in years. A checkmark designates that the p value was not reported.
For 15 of 17 items.
Systolic only.
Females only.
For three of eight items.
BMI, body mass index; BP, blood pressure; HbA1c, glycated hemoglobin; HRQoL, Health-Related Quality of Life; NA, not applicable due to lack of control group (CG) or chosen measure; NR, not reported; OCEBM, Oxford Centre for Evidence-Based Medicine; PAID, Problem Areas in Diabetes; SD, standard deviation; SF-36, 36-item Short Form; Sig Diff, significant difference between groups; Sig Eff, significant effect in the telehealth group (TG); SMS, short message service.
Stroke: Effects of Home Telehealth on Symptoms, Quality of Life, and Disease State
No symptoms or quality of life outcomes were reported.
INR, international normalized ratio; NA, not applicable because of lack of control group (CG) or chosen measure; NR, not reported; OCEBM, Oxford Centre for Evidence-Based Medicine; SD, standard deviation; Sig Diff, significant difference between groups; Sig Eff, significant effect in the telehealth group (TG).
Disease state
Tables 1 –7 give the full results. Eighty-eight articles reported on disease state, here defined as “physiological indicators of disease.” The measures used to assess disease state varied by disease and by study. We grouped these measures into seven outcome categories in order to facilitate analysis (Table 8). Note that some measures fell into more than one category. Blood pressure, for instance, was used as an indicator of clinical stability in heart failure patients. In populations with diabetes, it was generally taken as a measure of general health or risk of complications. In 65 articles, more than one measure of disease state was used. In total, there were 199 instances in which a measure was used to assess the effects of home telehealth on disease state. Some instances included both within- and between-group analyses, whereas others had only one of the two:
Measures of Disease State
Measures were grouped into seven outcome categories.
Includes total cholesterol and triglycerides. Excludes instances in which only low-density lipoprotein or only high-density lipoprotein cholesterol was reported.
COPD, chronic obstructive pulmonary disease; CVD (CAD), cardiovascular disease (coronary artery disease); CVD (HF), cardiovascular disease (heart failure); FEV1, forced expiratory volume in 1 s; HbA1c, glycated hemoglobin; INR, international normalized ratio; NYHA, New York Heart Association; T1 DM, type 1 diabetes mellitus; T2 DM, type 2 diabetes mellitus.
• Within-group analysis. In 93 instances (46.7%), significant improvement in the telehealth group was reported. 9 –60 No significant change was observed in 65 instances (32.6%). 9,11,15,16,20,22,25,29,31 –35,38,43,45,47,51,53,56,61 –77 Within-group changes or the significance values thereof were not reported in 18 instances (9.1%). 15,33,37,44,66,71,78 –82,94 In the remaining 23 instances (11.6%), within-group changes were not assessed because of the measure used (for example, annual mortality rate in a 1-year study). 15,19,27,34,50,83 –93
• Between-group analysis. A significant difference between groups was observed in 61 instances (30.7%). 9 –12,15,17 –29,32 –34,37,39,40,42 –44,46,48,50,52,54,55,59,60,71,74,76,78 –81,85 –88,93,94 In all cases but one, 19 the difference favored the intervention group. In 90 instances (45.2%), there was no significant difference between groups. 9,11,13 –16,19,21,25 –27,32 –34,37 –43,46,50,52,53,55,56,60 –62,64,66 –73,75,77,83,84,86,89 –93 In eight instances (4%), the result of this comparison was not reported. 9,26,37,54,60,64 In 40 instances (20.1%), there was no comparison group. 17,18,20,22 –24,30,31,35,36,39,45,47,49,57,58,63 –65,76,82
Quality of life
Tables 1
–7 give the full results. Thirty articles reported on quality of life. Articles were included in this count if they reported use of validated quality of life measures and or if the instrument was unspecified or unvalidated but was identified by the article's authors as a quality of life measure. Ten articles reported use of more than one quality of life measure. In total, there were 41 instances in which the effects of home telehealth on the quality of life of chronic disease patients were assessed: • Within-group analysis. In 20 instances (48.8%), significant improvement in the telehealth group was reported.
34,40,58,59,61,95
–103
No significant change was observed in 12 instances (29.3%).
13,20,26,75,94,98,104
–106
(However, Whitten and Mickus
106
reported a significant difference favoring the control group on one of eight subscales of the 36-item Short Form when controlling for key variables.) This comparison was not reported in eight instances (19.5%).
21,62,80,83,91,107,108
In the remaining instance, the type of analysis used meant that this comparison was not applicable.
44
• Between-group analysis. A significant difference between groups was observed in nine instances (22%).
34,44,59,62,75,80,96,107,108
In all cases, the difference favored the intervention group. In 23 instances (56.1%), there was no significant difference between groups.
13,26,40,59,84,94,95,98,99,101
–106
In five instances (12.2%), the results of this comparison were not reported.
21,61,91,100
In four instances (9.8%),
20,58,97
there was no comparison group (Whitten et al.
58
used two separate measures).
Symptoms
Tables 1
–7 give the full results. Six articles reported on symptoms. One article used two measures to assess symptoms.
34
Dansky et al.
66
reported on a study of two telehealth groups and one control group. This resulted in a total of eight instances in which the effects of home telehealth on symptoms of chronic disease were assessed: • Within-group analysis. Significant improvement was seen in the telehealth group in four instances
34,66,96
(Dansky et al.
66
included two telehealth groups using different monitoring programs). No significant change was observed in two instances.
34,109
The result was not reported in one of the remaining instances,
44
and the p value was not reported—although the result favored the intervention group—in the last instance.
108
• Between-group analysis. A significant difference between groups was observed in four instances.
34,44,66,96
In all cases, the difference favored the intervention group. In one instance, the p value of the outcome (favorable to the intervention group) was not reported
108
; in three instances, there was no significant difference between groups.
34,66,109
Discussion
Limitations
This review had several limitations. One is its currency. Our initial search was limited to publications from 2005 to 2010 (inclusive). In July 2012, we conducted a final follow-up search for highly relevant studies published after 2010. This search was intended to fill gaps in the literature and to allow us to incorporate any major developments that had occurred since our initial searches. However, it was not as comprehensive as the initial searches, and the data extraction process was abbreviated. It is possible that a more thorough review of post-2010 material would have altered our findings, particularly given the speed at which home telehealth has developed. We observed a marked increase in the rate of publication. In our initial search, the number of publications that we accepted into our review was, on average, 34.5 per year searched. The follow-up search yielded an average of 86.5 publications per year. Although it is possible that this is due to improvements in indexing, or perhaps more widespread adoption of preferred terms, the simplest and most probable explanation is increased research.
Another limitation of this review is the fact that members of the review team worked independently to screen, code, and assess the quality of the articles retrieved. This limitation was mitigated to the extent possible: clearly defined criteria were used; reviewers consulted with each other on an ongoing basis to discuss questionable articles; and periodic exercises in double-coding were used to improved inter-rater consistency. However, this remains a limitation.
Finally, it is possible that not all relevant articles were included in this review. Although we strove to be as comprehensive as possible in our initial search, references without abstracts were ultimately excluded, as were those for which full text could not be retrieved.
Analysis
In the studies we reviewed, home telehealth was as or more effective than usual care in improving disease state, quality of life, and symptoms in patients with chronic disease. This was true despite wide variations in study design, target population, and technology of choice. Patients using telehealth experienced significantly greater improvements than control group patients in disease state, quality of life, or symptoms in 38.8% of comparisons from Level 2 studies and over 30% of comparisons from all studies.
However, we cannot confidently identify the circumstances under which such improvements are most likely to occur. We found relatively little research in this area; most studies focused not on how or why telehealth worked, but on whether it worked. The exceptions were found primarily in studies of diabetes, the chronic disease with the most extensive body of evidence, and particularly in publications associated with the 5-year IDEATel program. This may reflect the large initial sample sizes needed to achieve acceptable confidence intervals for subgroup and multiple regression analyses.
Researchers who have investigated factors influencing the success of telehealth interventions have considered such variables as uptake, 93 the intensity of the intervention, 61,78 and the moderating effects of sex, 19 baseline glycated hemoglobin, 15,52 self-efficacy, 110 and depression. 111 More extensive use of this type of analysis has the potential to yield both clinical and economic benefits. The results would enhance policy makers' ability to apply existing research by enabling them to make a more informed assessment of the generalizability of a study's results to their target population.
Another limitation of existing research is the frequent exclusion of patients with comorbidities, who comprise roughly 30% of all Canadian seniors (>65 years of age) with chronic conditions and account for 40% of senior healthcare use. The exclusion of these individuals from study populations may result in under- or overestimates of the benefits of home telehealth to individuals and the healthcare system. We also observed a high level of variation in the level of details that authors provided in their descriptions of “usual care”; in some articles, usual care was undefined. More thorough reporting of usual care also has the potential to enhance our understanding of the mechanisms by which home telehealth interventions are successful.
Footnotes
Acknowledgments
This project was supported by the Canadian Institutes of Health Research (
Disclosure Statement
No competing financial interests exist.