
Abstract
Telecardiology provides mobility for patients who require constant electrocardiogram (ECG) monitoring. However, its safety is dependent on the predictability and robustness of data delivery, which must overcome errors in the wireless channel through which the ECG data are transmitted. We report here a framework that can be used to gauge the applicability of IEEE 802.11 wireless local area network (WLAN) technology to ECG monitoring systems in terms of delay constraints and transmission reliability. For this purpose, a medical-grade WLAN architecture achieved predictable delay through the combination of a medium access control mechanism based on the point coordination function provided by IEEE 802.11 and an error control scheme based on Reed–Solomon coding and block interleaving. The size of the jitter buffer needed was determined by this architecture to avoid service dropout caused by buffer underrun, through analysis of variations in transmission delay. Finally, we assessed this architecture in terms of service latency and reliability by modeling the transmission of uncompressed two-lead electrocardiogram data from the MIT-BIH Arrhythmia Database and highlight the applicability of this wireless technology to telecardiology.
Introduction
Typically, a patient in cardiac arrest has 240 s before permanent brain damage occurs. A hospitalized patient who is able to alert medical staff can generally be resuscitated within 30 s. However, it usually takes a couple of minutes for medical personnel to react, and it may take several seconds just to detect some physiological conditions. For example, at a typical resting heart rate of 50 beats/min, detecting a missed beat takes approximately 1.5 beats or 1.25 s; a premature ventricular complex takes approximately 3 beats or 2.5 s to detect, whereas a step change from 60 to 120 beats takes around 10 s to detect (such rate changes occur in paroxysmal supraventricular tachycardia). These observations imply that the latency of a real-time wireless electrocardiogram (ECG) monitoring system should not be greater than a few seconds. 1 –3 It must also transmit data with extremely high reliability, and the dropout rate should not exceed a few seconds per day. 4,5
Several wireless technologies are available for ECG monitoring, but nearly 50% of hospitals have already implemented IEEE 802.11 wireless local area networks (WLANs), 4,6,7 and over 30% more are expected to introduce them in the future. 8 However, it is challenging to satisfy medical quality of service (QoS) requirements with an IEEE 802.11 WLAN because of its error-prone physical layer and unpredictable medium access control (MAC). Furthermore, a WLAN can have a high rate of data collisions between sending nodes, leading to frequent retransmission and unpredictable delays, together with jitter, which is likely to disrupt real-time continuous patient monitoring. These issues need to be addressed before the vision of wireless healthcare can be fully realized.
We note that the MAC layer of a WLAN, as described by IEEE 802.11, 9 is separated into MAC and logical link control (LLC) sublayers: we exploit this separation to create an effective solution to this problem. We contend that predictable ECG transmission can be achieved by the use of point coordination function (PCF) mode for medium access, which is included in IEEE 802.11. The PCF provides a bounded delay because it uses a centralized polling scheme in which a single access point (AP) acts as a point coordinator. If a group of devices is coordinated by the PCF, then the channel access times are divided into beacon intervals, each of which is composed of a contention-free period and a contention period. The point coordinator maintains a list of registered devices, which are polled during the contention-free period in the order in which they are listed. When a device is polled, it receives permission to transmit data with a maximum length. Thus the contention period can determine the maximum duration of contention-free period needed to accommodate all transmitting devices.
The LLC protocol controls the errors that are sure to occur on wireless links. The method of error control that is used must provide acceptable reliability, uniform throughput, and a bounded delay, if it is to achieve the QoS necessary for real-time ECG monitoring. To achieve these goals, we introduce forward error correction into the LLC protocol, based on Reed–Solomon (RS) erasure codes, which are linear block codes in a finite Galois field (GF). If α is an element of order n in GF(q), then n is the smallest positive integer such that αn
=1, where 1 is the multiplicative identity for the field. The set of all vectors (c
0, c
1, … ,cn
–1) in (GF(q))
n
such that
RS coding can be made more effective by using a two-dimensional array buffer called an error control block (ECB), shown in Figure 1. Packets containing data, each of length L bits, are read into this array in rows, and RS coding is applied along its columns. The number of packets in each row of the buffer, M, determines the extent of data interleaving. 10 A high value of M disperses consecutive packets into different code words, which improves performance in the presence of time-varying shadowing. However, this comes at the cost of increased buffer requirements and buffering delays at the receiver. The amount of storage required is nML bits, although a second buffer is required in the receiver to store new packets while the preceding block is taken from the first buffer and decoded.

Construction of an error control block for block interleaving, and the packet arrangement inside the error control block for block interleaving.
The RS erasure decoding process can be logically split into three computational components. 11 The first component decides whether to try correcting the erasures in a code word. The second component builds the corresponding syndromes that are required to perform the erasure correction loop. This loop contains the third component, which is repeatedly invoked to correct each erasure in the code word. As a result, the time required to decode a code word for different numbers of erasures in a code word can be predicted as shown in Figure 2, where ti is the time required by the ith component of the RS erasure decoder to process a codeword. Because the RS decoding time is not constant, jitter occurs, and its magnitude is the difference between the delays in the arrival of data in any two consecutively decoded ECBs at the upper transport layer.
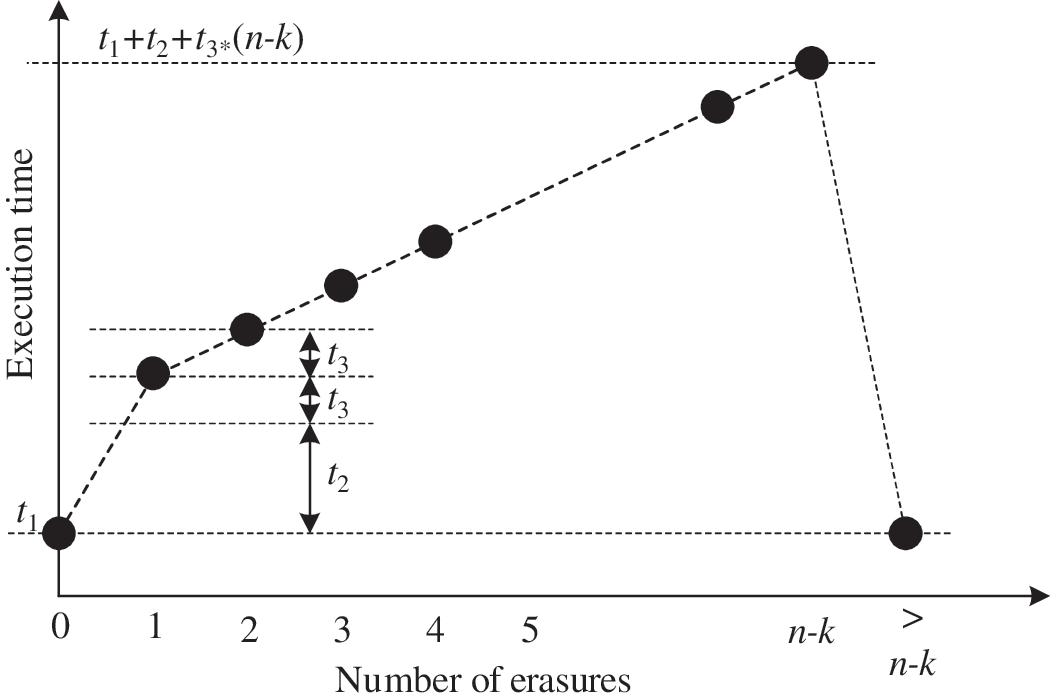
Computation times for decoding code words containing different numbers of erasures: ti (i=1, 2, 3) is the time taken by the ith component to decode a code word containing a single erasure.
The upper-layer protocol reads out decoded data from the link-layer ECB. When the channel condition is good, RS decoding will not take long, and the decoded data will arrive sooner at the upper layer of the protocol. Conversely, when the channel condition is bad, RS decoding will take longer, and the decoded data will arrive late. This variation in RS decoding delay can lead to buffer underrun, causing service dropout. Rate control is therefore required to smooth these delay variations if we are to meet the data delivery requirements of ECG monitoring; this can be achieved by a jitter buffer. The size of the smallest buffer that can absorb the jitter caused by variations in RS decoding delay is determined by the maximum amplitude of the jitter, J
max, as shown in Figure 3, and this amplitude can be found as follows:
where P is the period between the arrival of successive ECBs, Tw
is the worst-case execution time, and Tb
is the best-case execution time for decoding a single ECB. These times can be expressed as follows:
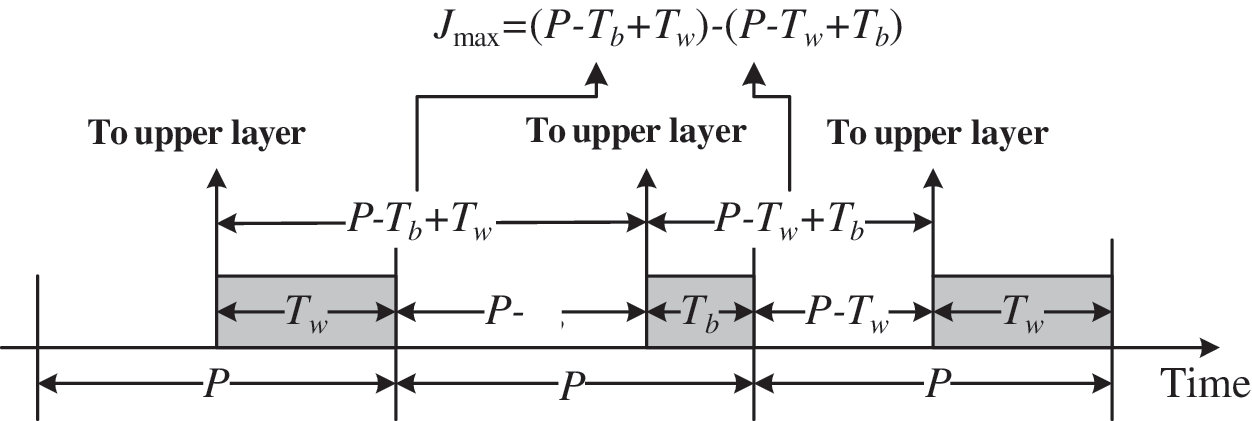
Jitter (J) due to variation in Reed–Solomon decoding time and the situation in which the jitter has its maximum amplitude. P is the time between the arrival of successive error control blocks.
where Nc
is the number of code words in each ECB buffer, which is ML/s, where s is the symbol length. Allowing for jitter, the required size of the buffer, B, can now be expressed as 2nML+J
max
μe
, where μe
is the ECG data-rate. The corresponding buffering delay D is then given by nML/μe
+Jmax
, and the resulting variation in initial service latency L can be expressed as follows:
where
In the remainder of this article, we will evaluate the reliability, latency, and applicability of the IEEE 802.11 WLAN-based architecture to telecardiology. We will now derive appropriate system parameters, including the level of block interleaving and the size of the jitter buffer needed to avoid service dropout, by measuring variations in transmission delay, and show that the required levels of reliability and latency can be achieved with this WLAN system architecture. This suggests that this wireless technology may have more general applicability in healthcare.
Materials and Methods
The aim of this simulation is to assess the robustness of the proposed WLAN architecture. Figure 4 shows a scenario in which a wireless network is used for remote ECG monitoring within a hospital. The configuration of ECG sensors used to collect cardiac signals from an ambulant patient will be chosen to meet medical criteria, and different setups require different numbers of leads. If there are Nr leads and if the signal from each lead is digitized at a rate of Ns samples per second with a resolution of Rs bits, then the resulting data traffic μe will be NrNsRs bits/s. The sampling frequency is typically between 300 Hz and 500 Hz, and the resolution of each sample is usually 12, 16, or 32 bits. 5 So, for example, if data are recorded by 12 leads at 500 Hz and digitized with a resolution of 16 bits, the resulting ECG stream has a data-rate of 96 kilobits/s. This stream is packed into frames (a frame denotes a physical-layer packet, which is not the same as a MAC/LLC-layer packet, even though a frame usually contains a single MAC/LLC-layer packet) and then sent to an AP in the hospital through a wireless channel.
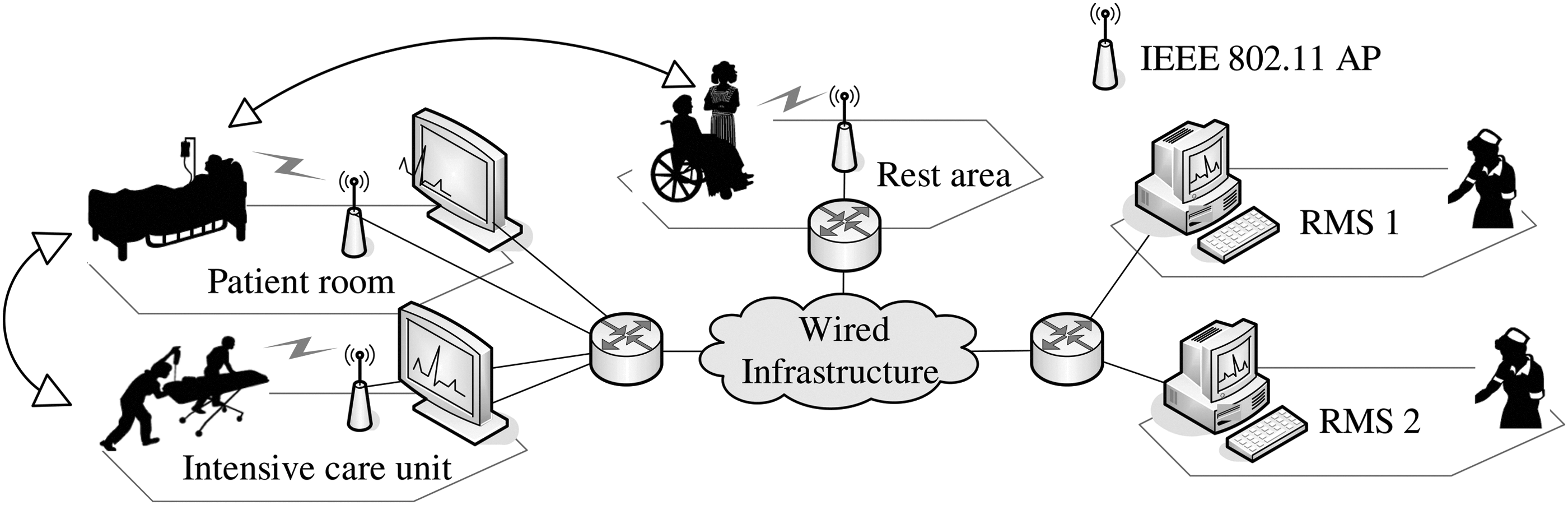
Scenario for the application of wireless technologies to electrocardiogram monitoring within a hospital, as well as the associated network architecture. RMS, remote monitoring station.
We simulated the behavior of frame errors that arise in data transmission on the sort of fading channel that we expect to find between an ECG sensor and its AP, using the threshold model suggested by Zorzi et al.
12
These authors have shown that the Markov approximation is a good model of the frame error process over a fading channel for a wide range of modulation schemes, frame lengths, and error correction capabilities. The wireless channel is described using two independent parameters, q and r, where q is the probability that the transmission of the ith frame is unsuccessful, given that the (i – 1)th frame was transmitted successfully, whereas r is the probability that the ith frame is successfully transmitted, given that the (i – 1)th frame was not. The threshold of flat Rayleigh fading relates these parameters as follows:
where ɛ is the steady-state frame error rate (FER) and F is the fading margin. Now, the value of r can be calculated as
The term ρ is the correlation coefficient of two samples of the complex Gaussian fading process and is equal to
In this study, we presumed that an ambulant patient would be traveling at a speed υ of between 2 km/h and 5 km/h, and we varied the FER experienced by a wireless device attached to his or her body to between 0 and 0.03. Each such device sends ECG signals in slots assigned by the PCF in a round-robin manner, so that consecutive frames sent by each device are interleaved. Table 1 lists the corresponding Markov parameters for the channel conditions we considered.
Markov Parameters Used in the Simulation
FER, frame error rate.
The AP relays the ECG frames that it receives across a wired backbone infrastructure to the remote monitoring station (RMS), or some other location in the hospital, where they are filled into the ECB reserved for RS erasure decoding. (RS erasure decoding can be performed in either the AP or RMS, but it does not affect the results because a wired network delivers data much more reliably than a wireless network so that all data losses can be attributed to the wireless network without significant inaccuracy. We assume that decoding is performed at the RMS because legacy 802.11-based APs do not provide such functions.) We used the same forward error correction control parameters as Agashe et al.,
15
including the RS codes (16,12), (16,13), and (16,14); the symbol length s was set to 8 bits, and the number of packets in each row of the buffer (M), which determines the level of block interleaving, was varied between 1 and 8. Table 2 shows values of ti
for a sample implementation of the RS erasure decoder (available at
Execution–Time Profiles on an ARM11-Based Platform Operating at 400 MHz
RS, Reed–Solomon.
Simulation Parameters
Finally, we analyzed the reliability of a two-lead ECG monitoring system using the proposed WLAN architecture. For this purpose, we used the MIT-BIH Arrhythmia Database, 16 which has been widely used to assess the performance of ECG-related schemes. 2 This database contains 48 half-hour excerpts of two-channel (or two-lead) ambulatory ECG recordings obtained from 48 subjects studied by the BIH arrhythmia laboratory. Recordings were digitized at 360 samples/s per channel, with 11-bit resolution over a 10 mV range, which corresponds to a data-rate of 3,960 bits/s in each channel. Data packets from both channels were multiplexed before transmission, and the resulting ECG data-rate μe was (=2×360×11) 7,920 bits/s.
In summary, to evaluate our WLAN architecture, we obtained error traces of frames transmitted over a wireless channel by simulating the PCF in the MAC sublayer using the channel error model we explained [condition (1) in Fig. 5]. These traces were subsequently fed to the RS erasure decoding simulator [condiiton (2) in Fig. 5]. Residual packet errors after RS decoding and their locations, generated by the simulation, were applied to a trace from the MIT-BIH Arrhythmia Database [arrow (3) in Fig. 5]. Finally, the reconstructed ECG signals were evaluated [arrow (4) in Fig. 5].
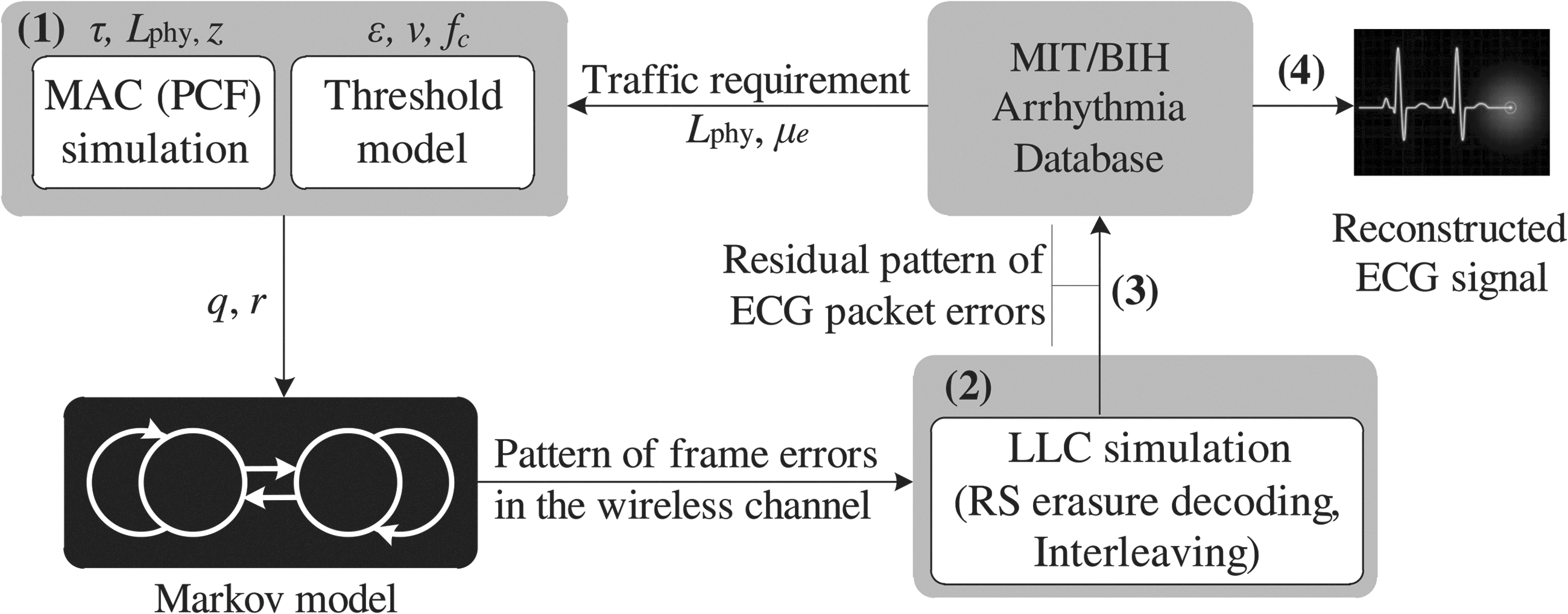
Simulation structure for quality of service evaluation. ECG, electrocardiogram; LLC, logical link control; MAC, medium access control; PCF, point cooredination function; RS, Reed–Solomon.
Results
Figure 6 shows the residual rate at which uncorrupted packets arrive at the RMS, after RS decoding for different values of the block interleaving parameter M, and at the worst channel condition that we considered (i.e., ɛ=0.03 and υ=2 km/h). Figure 6 shows the average, maximum, and minimum rates over 100 simulations, each of which processes around an hour's worth of ECG data. Basically, transmission reliability improves with the level of block interleaving, but, eventually, performance saturates when the value of M becomes large so that almost all the error bursts can be interleaved. We can see that values of M larger than 4 produce acceptable transmission reliability.
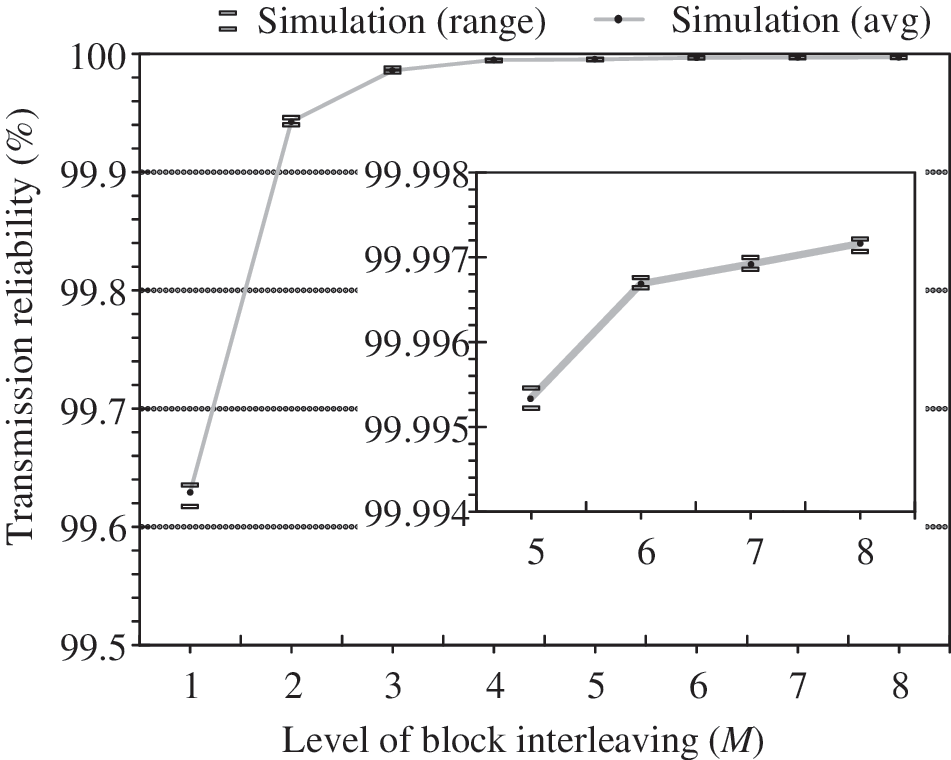
Transmission reliability in the worst case.
The QRS complex of the ECG corresponds to the heart rate of a patient, and a missing QRS complex increases the RR interval. If there is no error control, then the reconstructed ECG signal may not show some QRS complexes, as seen in Figure 7b. Attenuated waveforms of this sort may be misinterpreted by cardiologists as the symptoms of an atrioventricular block. We see that the missing QRS complexes are restored when error control is applied (Fig. 7c). As the value of M increase, the reconstructed signal looks more and more like the original ECG signal (Fig. 7a), increasing the chance of an accurate diagnosis.
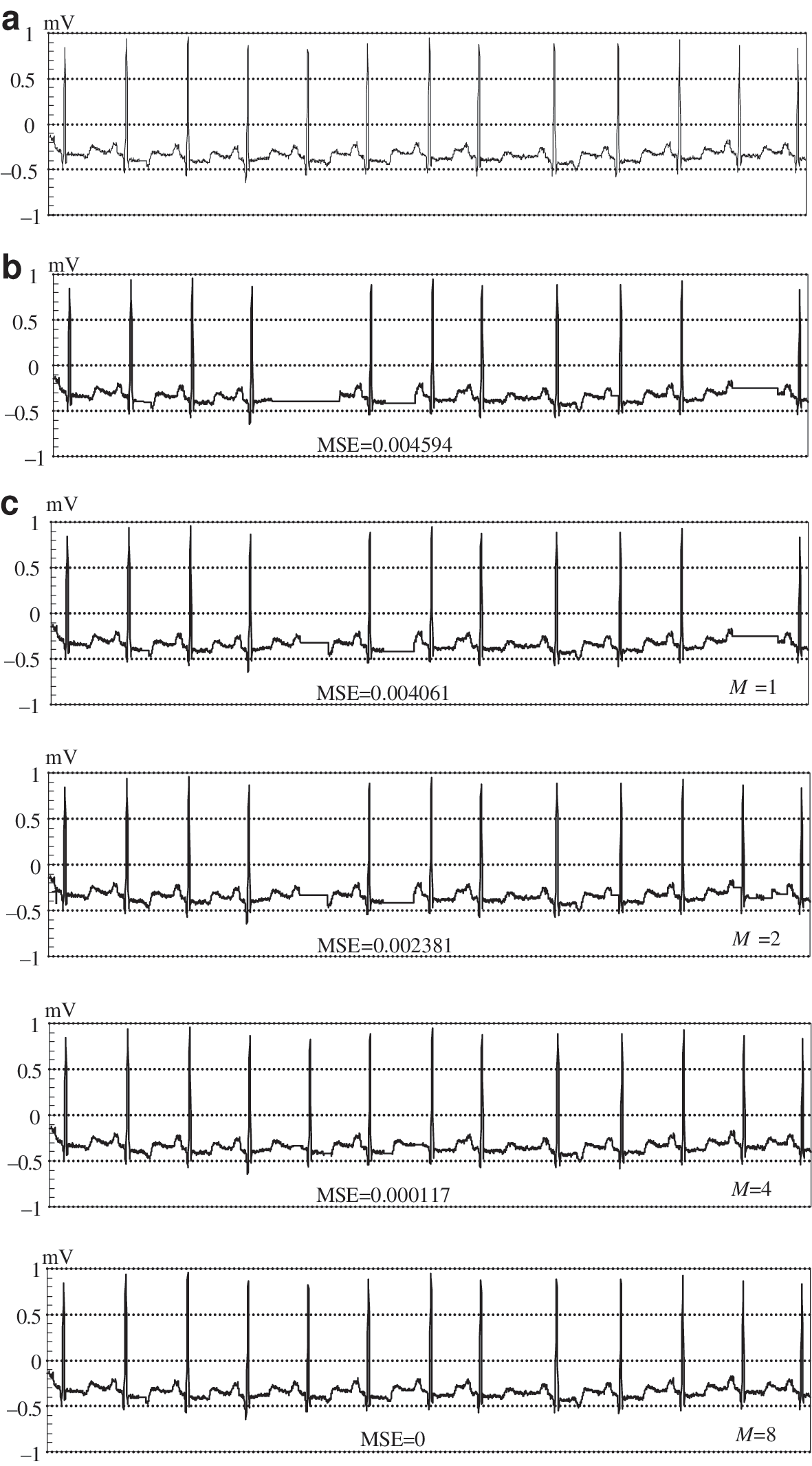
Analysis of an electrocardiogram signal from a modified limb II lead over an interval of 10 s. This example was selected because of the presence of significant error bursts (ɛ=0.03, υ=2 km/h, record number: 100):
We quantified the improvement resulting from error control by evaluating the mean-square error (MSE) as the value of M increased. The MSE over a time interval t can be expressed as
Mean-Square Errors of Reconstructed Electrocardiogram Signals for the Selected Data Streams from the Database
LLC, logical link control.
Table 5 illustrates the effect of patient mobility on average MSEs over a half-hour of reconstructed ECG signals, again averaged over 100 simulations. The FER was set to 0.03, the interleaving factor M to 4, and patient speed again varied between 2 km/h and 5 km/h. We expected the correlation properties of the fading process to depend on mobility (i.e., because consecutive frames are likely to exhibit an increased correlation as the speed of a mobile object declines, causing longer bursts of errors). This is indeed what happens: for a given FER, the MSEs of the reconstructed ECG signals increased as the speed of the patient decreased, as shown in Table 5.
Mean-Square Errors of Reconstructed Electrocardiogram Signals over a Half Hour for a FER of 0.03 (M=4) and Varying Patient Mobility
We have shown how the quality of the reconstructed ECG signal improves dramatically with the level of interleaving. However, this has a cost in terms of memory requirement and buffering delays, as illustrated in Table 6. The upper bounds
Memory Requirements, Buffering Delays, and Worst-Case Latency of the System for Different Levels of Interleaving and Two Workloads
Buffering delay and worst-case initial service latency are in seconds.
The workload of the ECG application increases when more detailed information is obtained from the patient by the use of more leads, sampling the ECG data at a higher frequency, a higher resolution, or some combination of these. Table 4 shows how the worst-case latency was affected by an increased workload. The increase in data-rate means that each ECB is filled sooner, and the buffering delay is reduced, and hence also the maximum initial latency.
Discussion
General requirements for patient monitoring using WLANs have been discussed by several authors, 5 –8,17,18 who examined different scenarios and requirements and proposed appropriate systems and architectures. In particular, Baker et al. 4 and Baker and Hoglund 8 reviewed the aspects of IEEE 802.11 wireless technology that affect its suitability for medical telemetry, as well as issues related to its implementation in hospitals.
Kang et al. 19 proposed a novel IEEE 802.11 WLAN architecture suitable for wireless ECG transmission, with a focus on channel errors, and showed that their proposed architecture can provide sufficient reliability for medical-grade services. However, timing aspects were not considered in this work, even though they are crucial determinant of the safety and sustainability of ECG monitoring. That is why this study reports an architecture for wireless health monitoring applications based on IEEE 802.11 standards that has a predictable delay, as well as ensuring service reliability. We believe that this is the first systematic investigation of the applicability of WLAN technology to ECG monitoring systems in terms of delay constraints and transmission reliability. Nevertheless, this study has certain limitations that need to be addressed.
First, we believe that there have not yet been sufficiently comprehensive measurements of wireless channel conditions in medical environments. Measurements from 3.1 to 6 GHz were carried out at Oulu University Hospital for ultra-wideband applications. 20 However, most commercial low-power wireless systems still operate in the industrial, scientific, and medical 2.4 GHz band. Future IEEE 802.15.6 body area network systems for wearable devices may also operate in this band. A straightforward solution is to use available channel models for indoor scenarios at 2.4 GHz. 21,22 However, their parameters are very sensitive to the propagation environment. 23 Channel measurements in a hospital at 2.4 GHz have been reported 24 but were limited to propagation within a ward, and wider mobility was not considered. De Francisco 25 has recently proposed indoor channel models at 2.4 GHz for hospital environments, which take account of patient mobility, but the application of these channel models is controversial because they have not yet been assessed across a large number of hospitals. In this study, we used the channel error model due to Zorzi et al., 12 which was designed for general mobile environments, because we plan consider ECG monitoring at longer ranges within a hospital and also outdoors. We acknowledge the need for a more realistic channel model that explicitly represents propagation across different spaces within a hospital.
Second, we need to consider the operation of both the data-link layer and the transport layer, which performs its own error and flow control functions. Changes in parameters in the lower layers may affect processes in the upper layer and thus determine the performance of the entire system. Therefore, a cross-layer design is preferred.
Finally, conventional QoS metrics such as FER and MSE may be insufficient to evaluate the QoS level of medical applications. The most critical concern in medical-grade QoS is whether the data actually presented to medical personnel can be interpreted correctly and lead to an accurate diagnosis. In the future, we plan to assess the effectiveness of our adaptive framework in a practical setting. We would like to design QoS metrics for wireless ECG transmission that can accurately evaluate the extent to which the features of an ECG signal that contribute to an accurate diagnosis are preserved during wireless transmission.
Conclusions
Pairing healthcare with wireless transport requires a thorough understanding of the particular medical application, the detailed functions and capabilities of the wireless technology, and safety requirements. Within this context, we have considered IEEE 802.11 WLANs as a candidate wireless technology for telecardiology and proposed an architecture to enhance the QoS of wireless ECG monitoring in terms of service predictability and reliability. The architecture that we propose incorporates protocols for MAC and error control that can guarantee reliable and deterministic packet delivery, thus contributing a major component to a safe wireless ECG monitoring service. We have considered key design issues such as mobility and the resulting high rate and bursty nature of frame errors, which are inherent characteristics of wireless environments. Our results demonstrate the potential of IEEE 802.11 WLANs in safety-critical medical applications.
Footnotes
Acknowledgements
This work was supported in part by the MSIP (Ministry of Science, ICT & Future Planning), Korea, under the ITRC (Information Technology Research Center) support program (NIPA-2014-H0301-14-1044) supervised by the NIPA (National ICT Industry Promotion Agency), and Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the MSIP (NRF-2013R1A1A1059188).
Disclosure Statement
No competing financial interests exist.