
Abstract
Introduction and Background
Specialized cardiac critical care is a central component in the management of critically ill, neonatal, pediatric, and adult patients with congenital and acquired heart disease. Scarcity of dedicated cardiac intensive care units (CICUs) with specialized medical staff is a widespread problem in developing countries with the pressing need to advance their level of expertise in the management of complex congenital heart disease. 1,2
Telemedicine is a relatively new tool, emerging as a valuable alternative to alleviate these deficiencies, providing expedited access to the opinions of qualified specialists from high-performance centers, and enabling education.
Telemedicine has been applied to adult critical care extensively and, to a lesser degree, to pediatric critical care for several years now. It is estimated that approximately 10% of all adult intensive care unit beds in the United States are currently being serviced by telemedicine. 3 In adult care also, there is a growing body of evidence suggesting a telemedicine-assisted system can be associated with improved patient outcomes, especially if applied in a systematic way and incorporating it as a part of a quality project. 4 There are fewer reports related to the use of telemedicine in pediatric intensive care units and the pediatric cardiology setting, with some of them related to critical care consultation or to rural isolated populations. 5 –8
We started an international telemedicine service in pediatric cardiac critical care (PCCC) (electronic CICU [e-CICU]) with one center in Colombia in 2010, and our initial experience was recently published, reporting positive results of a postintervention survey filled out by participating remote medical staff. 9 However, little is known about the optimal method of a telemedicine service delivery in the international setting.
This study was designed with the primary goal of describing our expanded experience with e-CICU with four participating hospitals in Latin America from July 2011 to June 2013, in anticipation for possible prospective interventions during a second phase of our program.
Materials and Methods
Physicians from the Heart Center at Children's Hospital of Pittsburgh (CHP) of the University of Pittsburgh Medical Center provided telemedicine services to four hospitals in Latin America: Center A (started in September 2011), Center B (started in May 2011), Center C (started in February 2013), and Center D (started in March 2010).
This study was conducted between July 2011 and June 2013. The Institutional Review Boards of all institutions approved this study separately.
Centers' Characteristics
All institutions are high-complexity-level reference centers with full intensivist coverage. Centers A, B, and D include an extracorporeal life support program. CHP is a state-of the-art children's hospital with 289 licensed beds. It has a 36-bed pediatric intensive care unit and an independent 12-bed CICU. Centers' characteristics are described in Table 1.
Centers' Characteristics
Dedicated cardiac intensive care unit.
Pediatric intensive care unit.
ICU, intensive care unit.
e-CICU: Work System
Our current e-CICU provides telemedicine service with structured meetings on a daily basis; the number and type of patients per meeting are selected by local physicians at each hospital. Meetings took place between local physicians at each center and one or two physicians from our e-CICU, both being native Spanish speakers. Support from the cardiothoracic surgery, interventional cardiology, and transplant team was requested whenever needed. Because of the constraints of an international telemedicine setting, our model of service does not currently allow physicians from CHP to access electronic medical records from remote centers. Nonetheless, information related to technical aspects of the telemedicine encounters as well as relevant patient data was documented in a prospectively collected database (e-CICU database) implemented by one physician from CHP and stored with restricted access within our intranet. Telemedicine hardware and technical information have been already described elsewhere. 9
Data Collection
De-identified data were retrospectively collected from our e-CICU database. We included specific telemedicine information such as remote institution, date and time of session, consultation type (first versus follow-up), connection quality, assessed information (clinical data, X-ray, monitor, electrocardiogram, echocardiogram, etc.), activities during teleconsultation, patient status (preoperative, postoperative, or medical), diagnosis, surgical procedure, and provided recommendations. All patients registered from July 2011 to June 2013 were included.
Surgical procedures were classified according to Risk Adjustment for Congenital Heart Surgery (RACHS-1) categories. This method allows for discrimination in mortality risk according to surgical complexity, with 1 being the group with the lowest and 6 being the one with the highest anticipated mortality, respectively. 10
Survey Development
At the end of the study period an anonymous survey was conducted investigating the acceptance and general perception among remote physicians in contact with our e-CICU. A questionnaire consisting of 30 points grouped in seven main questions written in Spanish by a native Spanish speaker was created and sent electronically through an Internet-based survey tool (SurveyMonkey®, Portland, OR). We evaluated acceptance through the assessment of the following categories: general satisfaction, perception about work system quality, impact on medical practice, and perception about the system usefulness. To evaluate work system quality, we queried about audio and video quality, mobility of the system, lack of signal interruption, promptness of response, and time spent in teleconsultation. We asked the following specific areas in which telemedicine may have changed medical practice: diagnostic approach, medical treatment, and surgical treatment. Telemedicine usefulness was assessed in the following aspects: CICU, patient outcome, and staff education. Usefulness in the CICU was evaluated through perception about telemedicine impact in CICU quality of care, medical staff, and daily activities workflow. To evaluate perception on telemedicine usefulness in patient outcome, we queried about impact on patient survival, privacy, prevention of medical errors, and family satisfaction.
Data Analysis
SPSS (Chicago, IL) Statistic version 19 software was used for statistical analysis. For survey analysis, mean and standard deviation for each domain were calculated according to a 5-point Likert scale, with 1 being the lowest and 5 being the highest value. Continuous variables are expressed as mean and standard deviation or median and range when appropriate. Categorical variables are reported as frequencies and percentages. For comparison among centers, we conducted an analysis of variance test (with Bonferroni's adjustment) for continuous variables and chi-squared or Fisher's exact test for categorical variables where appropriate. We used the Kruskall–Wallis test to evaluate differences in RACHS-1 distribution between centers.
Results
From July 15, 2011 to May 31, 2013, 1,040 consultations were conducted for 476 patients, with a mean of two consultations per patient (range, 1–21) and a median of one.
Patient Characteristics
By institution, 43.3% of the patients were from Center B, 29% from Center D, 16.4% from Center A, and 11.3% from Center C. The mean age of patients was 28 months (range, 1 day–31 years), with a median and mode of 5 and 4 months, respectively, and 56% of patients were males. The most frequent diagnoses by patient were ventricular septal defect (8.2%), atrioventricular canal (7.6%), cardiomyopathy (6.7%), hypoplastic left heart syndrome (6.5%), and transposition of great arteries with ventricular septal defect (6.1%). Of the consultations, 63.8% were postoperative congenital heart disease patients, 27% were preoperative management, and 9.2% related to medical management. The RACHS-1 distribution of patients who were subjects of teleconsultations is shown in Table 2 and Figure 1. Other cardiovascular surgeries not considered in this classification were hybrid procedures (2%), heart transplant (2%), ventricular assist device/extracorporeal membrane oxygenation (ECMO) (0.6%), and congenital diaphragmatic hernia repair (0.5%). The distribution of patient status at encounter was significantly different among centers (p<0.01) (Table 3 and Fig. 2). The RACHS-1 distribution among centers is described in Table 4.
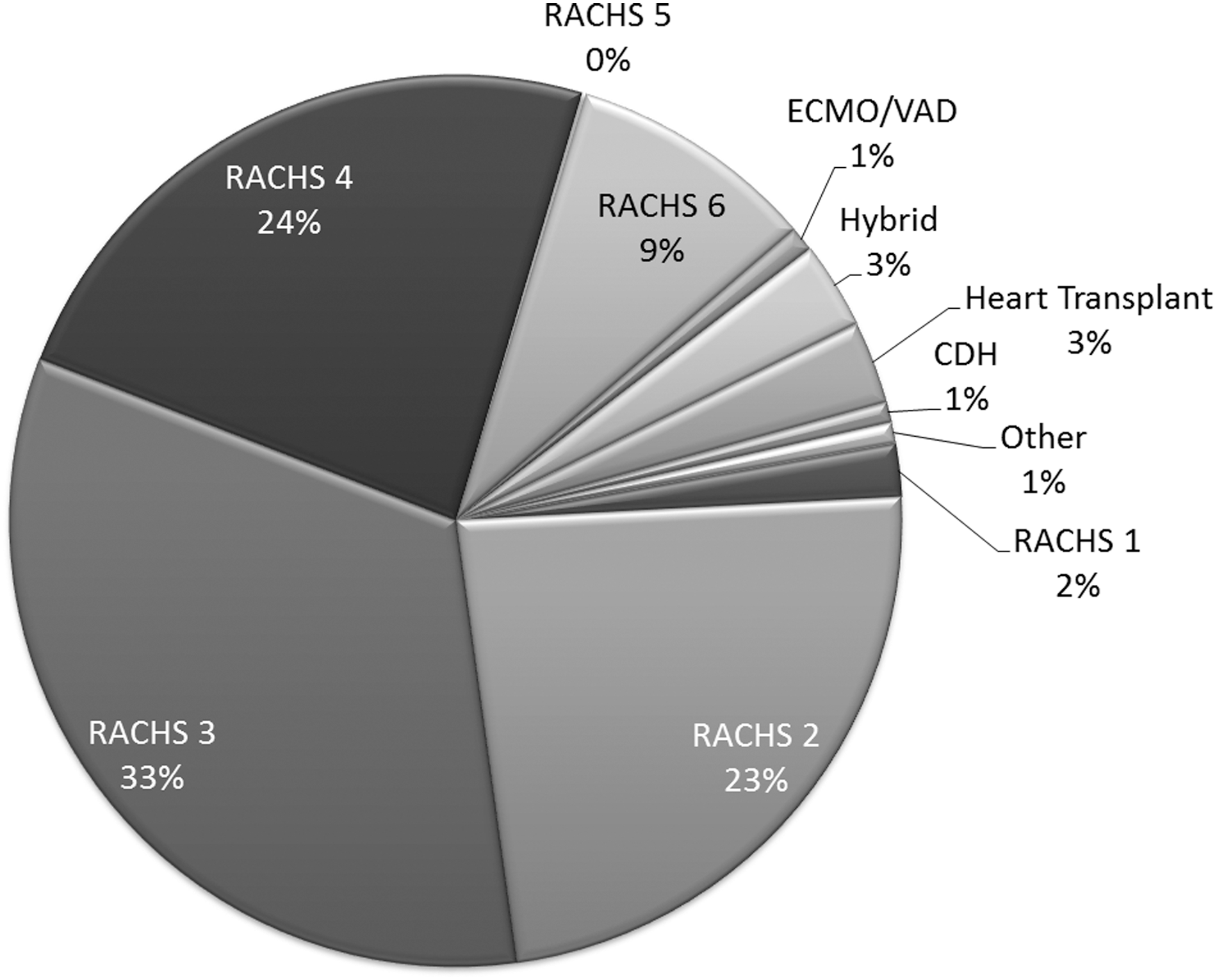
Type of procedure in surgical patients. CDH, congenital diaphragmatic hernia repair; ECMO, extracorporeal membrane oxygenation; RACHS, Risk Adjustment for Congenital Heart Surgery; VAD, ventricular assist device.
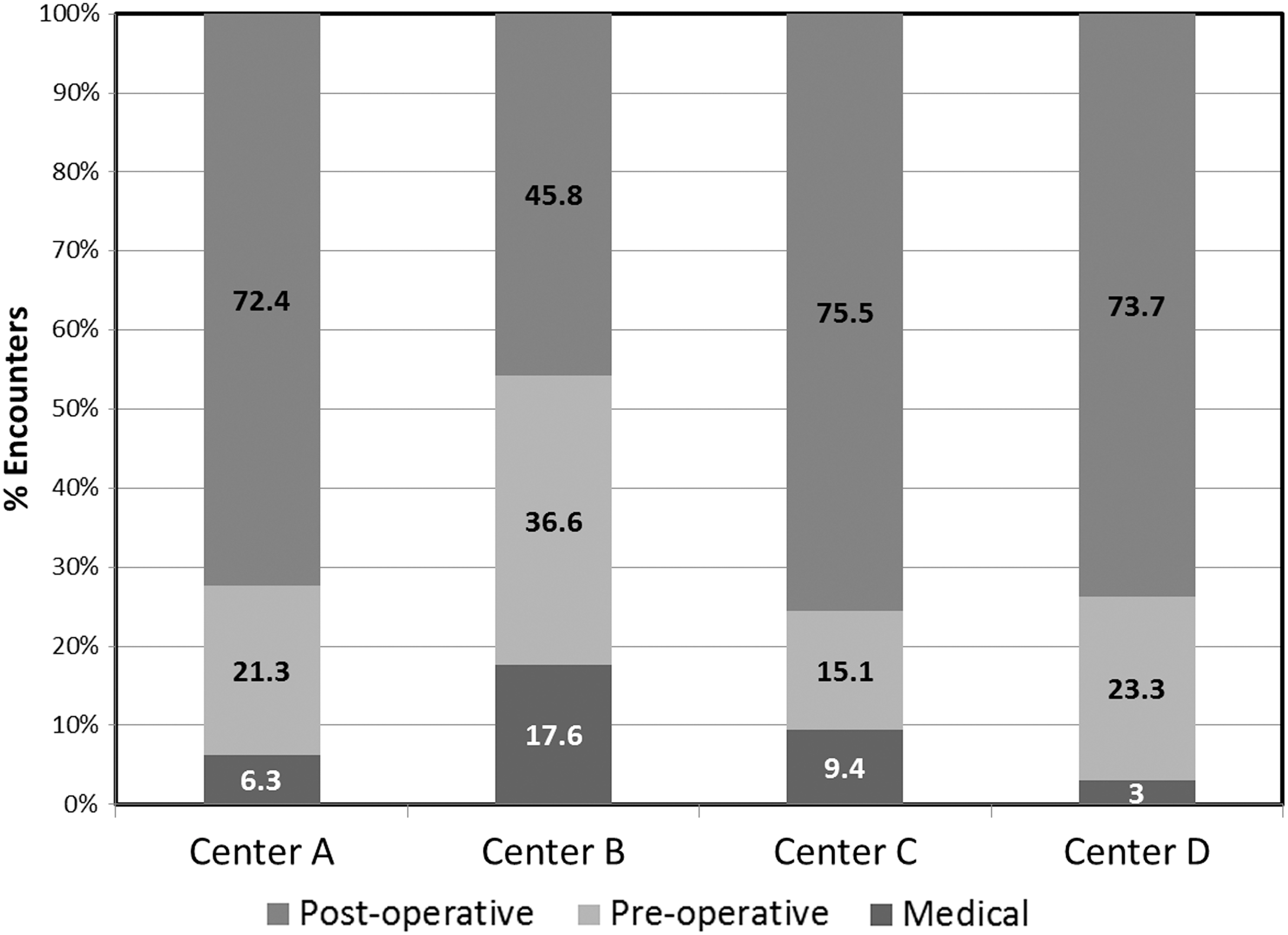
Patient status during teleconsultations by center.
Patient Distribution According to Surgical Status During Teleconsultations
CDH, congenital diaphragmatic hernia; ECMO, extracorporeal membrane oxygenation; OHT, orthotopic heart transplant; RACHS-1, Risk Adjustment for Congenital Heart Surgery; VAD, ventricular assist device.
Patient Status During Teleconsultations by Center
Data are number (%).
p<0.01 for chi-squared test.
Risk Adjustment for Congenital Heart Surgery Distribution During Teleconsultations by Centers
Data are number (%).
p<0.01 for Kruskal–Wallis test.
Characteristics of Telemedicine Encounters
A CICU physician from CHP participated in all the encounters. Other specialists attending to the telemedicine sessions included cardiac surgeons (19%) and neonatal intensivists (1%). Participation of our Cardiac Transplant Team was typically done in a store-and-forward fashion, and it was not tracked in our database.
The most frequent diagnoses during teleconsult are listed in Table 5. Associated factors commonly present during teleconsultation included pulmonary artery hypertension (14%), low cardiac output syndrome (13%), congestive heart failure (10%), acute kidney injury (5.4%), arrhythmia (4.5%), ventricular dysfunction (2.9%), trisomy 21 (2.8%), necrotizing enterocolitis (2.5%), sepsis (2.5%), stroke (2.4%), and intracardiac thrombus (1.3%).
Frequency of Diagnoses During Teleconsultations
Assessed information
Besides clinical history, evaluated information included chest X-ray (n=763 [73.4%]), patient (n=654 [63%]), monitor (n=649 [62.4%]), echocardiography (n=489 [47%]), electrocardiogram (n=248 [23.8%]), angiography/hemodynamics (n=87 [8.4%]), and other diagnostic studies (n=48 [4.6%]). The information assessed during teleconsultations was significantly different among centers (p<0.05) (Table 6).
Assessed Information During Teleconsultations by Centers
Data are number (%).
p<0.05 for Fisher's exact test.
CAT, computed tomography; MRI, magnetic resonance imaging.
Activities during telemedicine encounters
Other than discussion of medical history, activities included diagnostic study interpretation (n=757 [72.8%]) and real-time interventions (n=239 [23%]). In 49 teleconsultations (6%) a different diagnosis was suggested based on interpretation of cardiac or imaging studies.
Real-time interventions were defined as any diagnostic or therapeutic activities performed according to tele-intensivist recommendations and taking place during such encounters. In total, 268 real-time interventions were performed, and their frequency was different among centers (Table 7).
Real-Time Interventions During Teleconsultations by Centers
Data are number (%).
p=0.01 for Fisher's exact test.
The most frequent real-time intervention was echocardiography in 220 teleconsultations (82%), and others included cardiac rhythm-electrophysiology such as cardioversion, pacemaker settings adjustment, or adenosine in 18 (7%), ventilatory support adjustment in 11 (4%), pharmacologic therapy in 11 (4%), and ECMO manipulations in 8 (3%).
Recommendations
In total, 2,183 recommendations were given for 476 patients. They were related to pharmacologic therapy (n=740 [33.5%]), surgery (n=379 [17.4%]), new echocardiographic study (n=214 [9.8%]), diagnostic catheterization (n=126 [5.7%]), change in ventilator parameters (n=115 [5.3%]), interventional catheterization (n=81 [3.7%]), and cardioversion (n=6 [0.2%]), among others. Additionally, 70 (3.1%) ECMO-related recommendations were made.
The most frequent recommendations related with surgery were re-intervention/re-exploration in 43, pulmonary artery banding in 25, hybrid approach in 20, and Blalock–Taussig shunt in 19 teleconsultations.
There was a significant difference in recommendations given related to diagnostic study suggestion, echocardiographic re-evaluation, surgery, interventional catheterization, and ECMO adjustment among centers (p<0.005).
Survey Results
The survey was sent to 9 physicians at Center A, 9 at Center B, 25 at Center C, and 8 at Center D. The response rate was 44.4% in Center A, 88.8% in Center B, 44% in Center C, and 50% in Center D. Two of the surveys were incomplete. The main results of the satisfaction survey are shown in Table 8 and Figure 3.
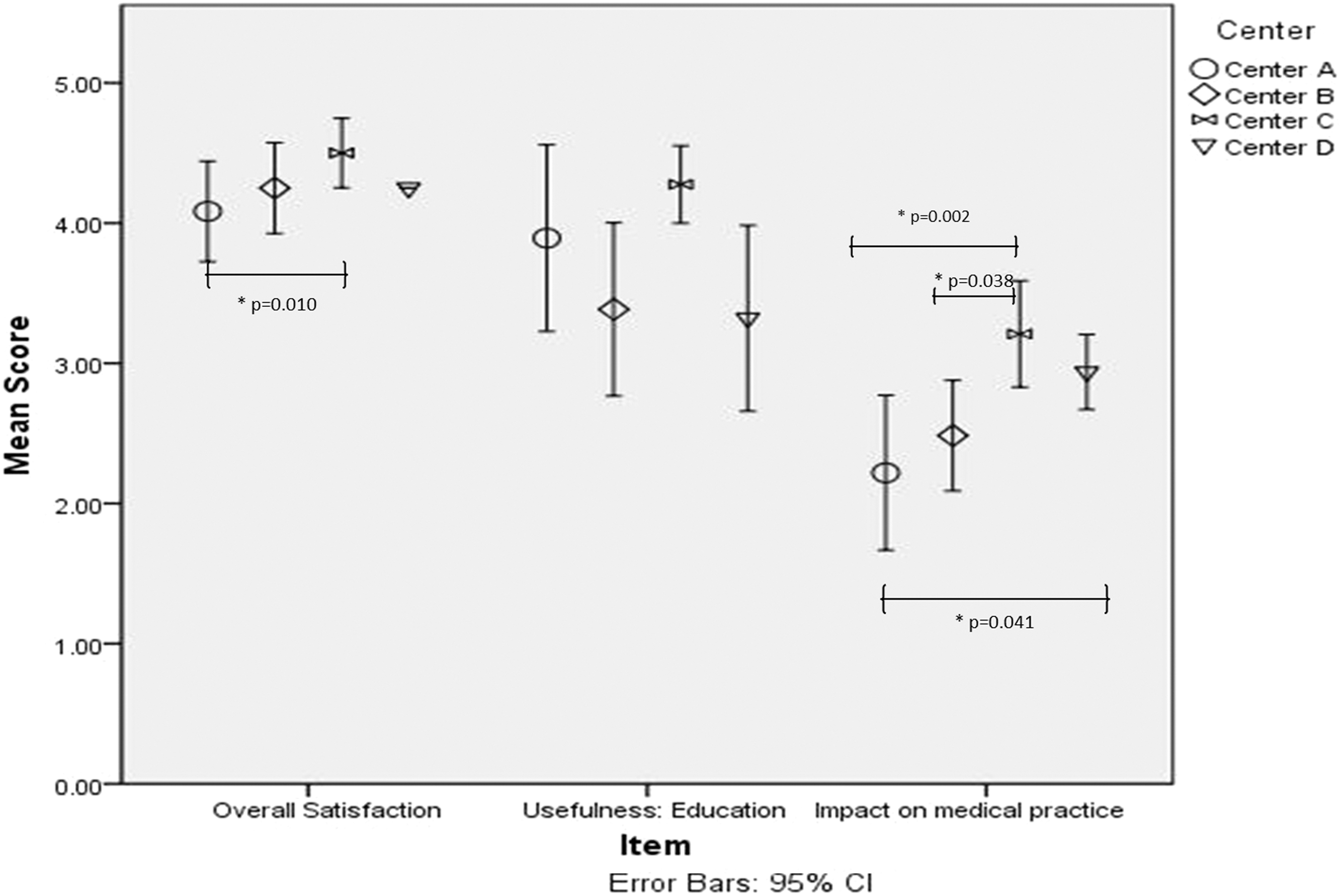
Multicenter satisfaction survey results: comparisons among centers. Error bars are 95% confidence interval.
Multicenter Satisfaction Survey
p<0.05 for analysis of variance.
Significant difference from the other centers.
CICU, cardiac intensive care unit; SD, standard deviation.
Survey participants
Twenty-two (81.5%) of the responders were specialists, and 5 (18.5%) were fellows. Of the responses, 40.7% were from Center C, 29.6% from Center B, and 14.8% from Centers A and D each.
Overall satisfaction
A large majority (96%) of responders were satisfied or very satisfied with the telemedicine service with a level of 4.27±0.18. There was a significant difference of overall satisfaction among centers (p=0.01), with Center C reporting the highest overall satisfaction.
Telemedicine work system
Telemedicine work system quality mean score was 4.36±0.37. Of the responders, 58% rated the promptness of response and time dedicated by the tele-intensivist to each case as very high. Among centers there was no significant difference about perception of work system quality (p=0.09).
Impact on medical practice
Physicians reported they changed their clinical practice sometimes in relation to the telemedicine encounters (mean, 2.7±0.61, with 5=always); this behavior was different among centers (p=0.002). Specific areas in which telemedicine may have changed clinical practice at remote centers were evaluated. Change in surgical management had the highest frequency (mean, 3.4±0.83), followed by change in hemodynamic support (3.3±0.84), diagnosis (2.9±1.02), mechanical ventilation (2.7±0.78), renal therapy (2.6±0.91), and sedatives and analgesic management (2.6±0.85).
Telemedicine usefulness
Overall, responders considered telemedicine useful in the CICU (mean score, 3.86±0.60); this perception was similar among centers (p=0.57). According to remote physicians, daily workflow activities were interrupted sometimes by the telemedicine encounters (mean, 3±1.3).
Telemedicine was considered useful in improving patient outcomes (mean score, 3.8±0.51), and there was no difference among centers (p=0.60). Physicians considered telemedicine useful for education (mean score, 3.7±0.71), and this perception was significantly different among centers (p=0.027), with 9 of 11 responders from Center C using telemedicine frequently for education.
Discussion
International telemedicine is recognized as a challenging endeavor, and some of the widely associated barriers to the development of an international program include legal, financial, and cultural factors, as well as infrastructure. 11
There is already reported experience, including our own, related to regional or international telemedicine in the pediatric cardiology field, as well as in the pediatric critical care setting. 4,9,12 Nonetheless, to our knowledge this is the first reported experience of multicenter international telemedicine related to PCCC and is the largest series of telemedicine use for ECMO advice.
An ideal model for telemedicine service delivery in the international PCCC setting has not been described. Ideally, a consistent approach should be used for centers with similar organization, skill level, and patient epidemiology.
According to our findings, most of the teleconsultations were provided to postoperative patients with complex congenital heart disease (RACHS-1 categories 3–6), and this seems appropriate given that management of these patients is more challenging for remote physicians.
Most of the recommendations given were related to pharmacologic therapy, diagnostics, and surgery. This coincides with the areas where physicians reported telemedicine had frequently changed their clinical practice.
We found significant differences in general RACHS-1 distribution, type of patient during consultation, and resource utilization among centers, perhaps reflecting differences in attended populations as well as different needs depending on the state of development of each cardiovascular center. The nature of this study does not allow us to make firm causal associations related to this question. Even so, we consider an ideal telemedicine consultation in the international PCCC setting is one in which advice is given with sufficient appraised patient information, representing a potential area for improvement along with the development of specific telemedicine formats for each center.
Our survey showed also differences among centers in overall satisfaction, perception about telemedicine usefulness in education, and change in medical practice. Given these findings, we believe a single model of telemedicine service delivery in the international setting is not feasible, and the work system should be adapted to recognize differences among centers in terms of organization, patient population, skill level, and needs.
Study Limitations
Given the nature of the study and the subjective quality of a survey, we are unable to ascertain any effect on patient outcomes. As staff acceptance and perceptions about our e-CICU can vary over time, future surveys will be needed to track these changes for quality improvement purposes. Finally, as in any satisfaction survey, a bias could exist with a preponderance of responders among those with positive perception about the service.
Conclusions
An international, multicenter telemedicine program in PCCC is technologically and logistically feasible. Differences in staff composition, resource utilization, and perception among centers should be considered when planning for future, prospective interventions.
Footnotes
Acknowledgments
We would like to thank the physicians who participated in the study and those who collaborated in our program development: at Children's Hospital of Pittsburgh, Brian Feingold, Jacqueline Kreutzer, Sara Mendoza, and Victor Morell; at Fundación Valle de Lili, Marcela Granados, Walter Mosquera, Jaiber Alberto Gutiérrez, Gabriel Santiago, and Juan Fernando Vélez; at Fundación Cardiovascular, Víctor R. Castillo, Alvaro Duran, Leonardo Salazar, Norma Serrano, Javier Idrovo, Claudia Flores, and Javier Castro; at Clínica Cardiovascular Congregación Mariana, Mónica Guzmán, Jorge Zapata, Rafael Lince, and Luis H. Diaz; and at Hospital Infantil de México Federico Gómez, Iñaki Navarro, Lourdes Marroquín, Alejandro Bolio, and Sergio Ruiz.
Disclosure Statement
No competing financial interests exist.