
Abstract
Introduction
There is a growing body of evidence assessing the capacity for mobile phones to perform as tools to facilitate diagnosis and aid clinical management. The increasing resolution of mobile phone cameras accompanied with the portability, accessibility, and built-in Internet connectivity has resulted in a device that is well positioned to capture and transmit medical images. Additional benefits include a relatively low cost of image acquisition and the widespread patient access to these devices. In addition, the following are key benefits when using mobile health (m-health) for medical imaging: 1. Connectivity—Internet connectivity inherent to smartphones suits them well for use in the health setting, allowing imaging to be transferred to central repositories easily. 2. Economics—When the cost of mobile phones is compared with that of dedicated medical imaging cameras, smartphones are far less expensive and can be used for various purposes. This allows financially feasible medical imaging in developing nations that may not otherwise be possible owing to cost limitations. 3. Applications (apps)—Specialized software loaded onto smartphones allow on-board processing of images specific to the task at hand and automate other needs such as image transmission.
The growth of smartphone-based imaging is evidenced by the dynamic market of available “apps,” which allow smartphone cameras to perform complex functions that previously would have required a dedicated computer.
Current-generation smartphones have excellent cameras that meet the standards of image quality requirements for medical photography. Even previous generations of mobile phone cameras that are commonly found in developing nations are adequate for certain diagnostic purposes in specialized disciplines. 1 Also, the high resolution of mobile displays has afforded the ability to assess clinically significant pathology. Adapters can also extend the use of these devices, for example, to mount the smartphone onto other devices such as microscopes 2 and ophthalmic slit-lamps. 3 Furthermore, there is a strong interest in m-health medical imaging in rural and remote areas where access to specialist services may be limited. 4 –6
A review of the current evidence was carried out to identify the capabilities and concerns regarding the use of mobile phones in the field of medical imaging.
Materials and Methods
Structured Review
A structured review of the literature was conducted to identify articles pertaining to the use of m-health for medical imaging (Fig. 1). For the purposes of this review, m-health devices were defined as devices that have wireless communication capability, run software apps, and are portable, which mostly consisted of mobile phones (including smartphones) and associated adapters. Articles were deemed eligible if they explored the use of m-health for medical imaging.
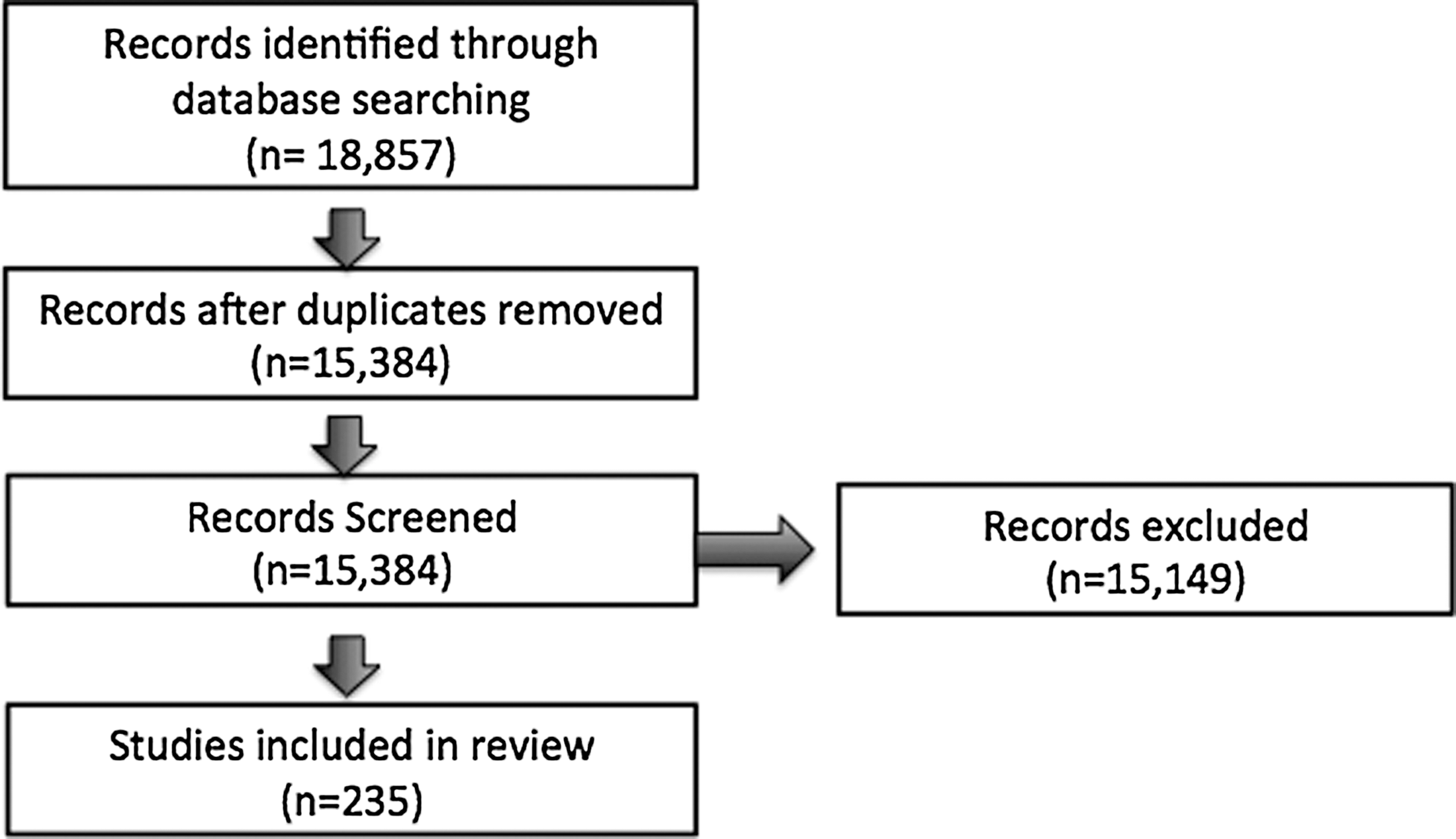
Flow diagram of the review process.
We searched the following electronic databases: Medline, EMBASE, The Cochrane Library, and Web of Science. A list of key words used for the search strategy can be found in Supplementary Appendix S1 (Supplementary Data are available online at
Results
In total, 18,857 articles were identified through the combined search strategy. After removal of duplicate articles and screening for relevance, in total, 235 articles were identified that were of relevance, spanning from 2002 to August 2013 (Supplementary Appendix S2).
Study Characteristics
The first article identified of relevance was published in 2002. Throughout the years, there has been a steady increase in the number of publications in the field (Fig. 2).
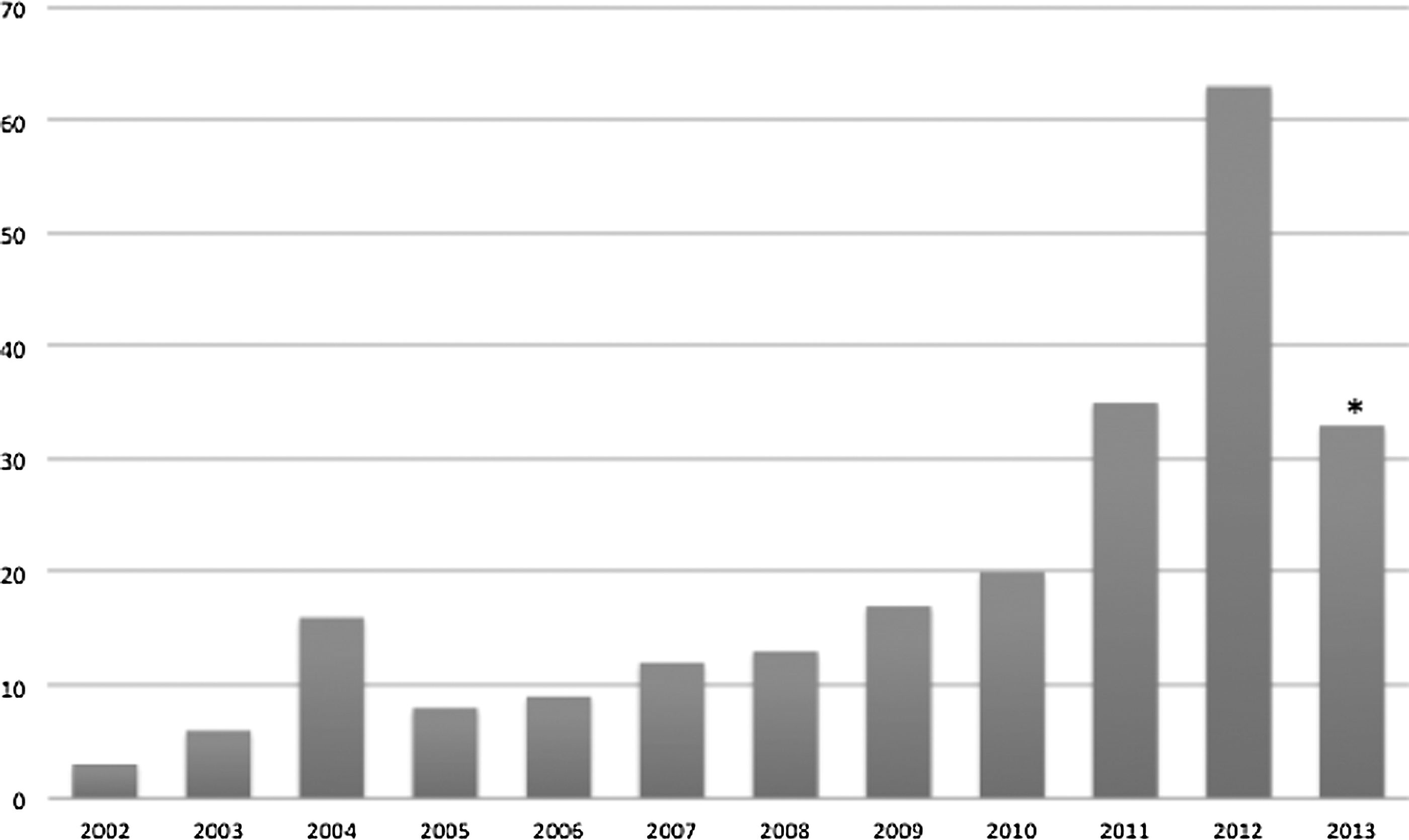
Number of mobile health (mHealth) imaging articles published in peer-reviewed medical journals per year. *The year 2013 only includes data until June 2013.
Of the 235 articles identified, 185 articles were specific to medical/surgical subspecialties, with 50 articles not specific to any subspecialty. A breakdown of articles by specialty is seen in Figure 3.
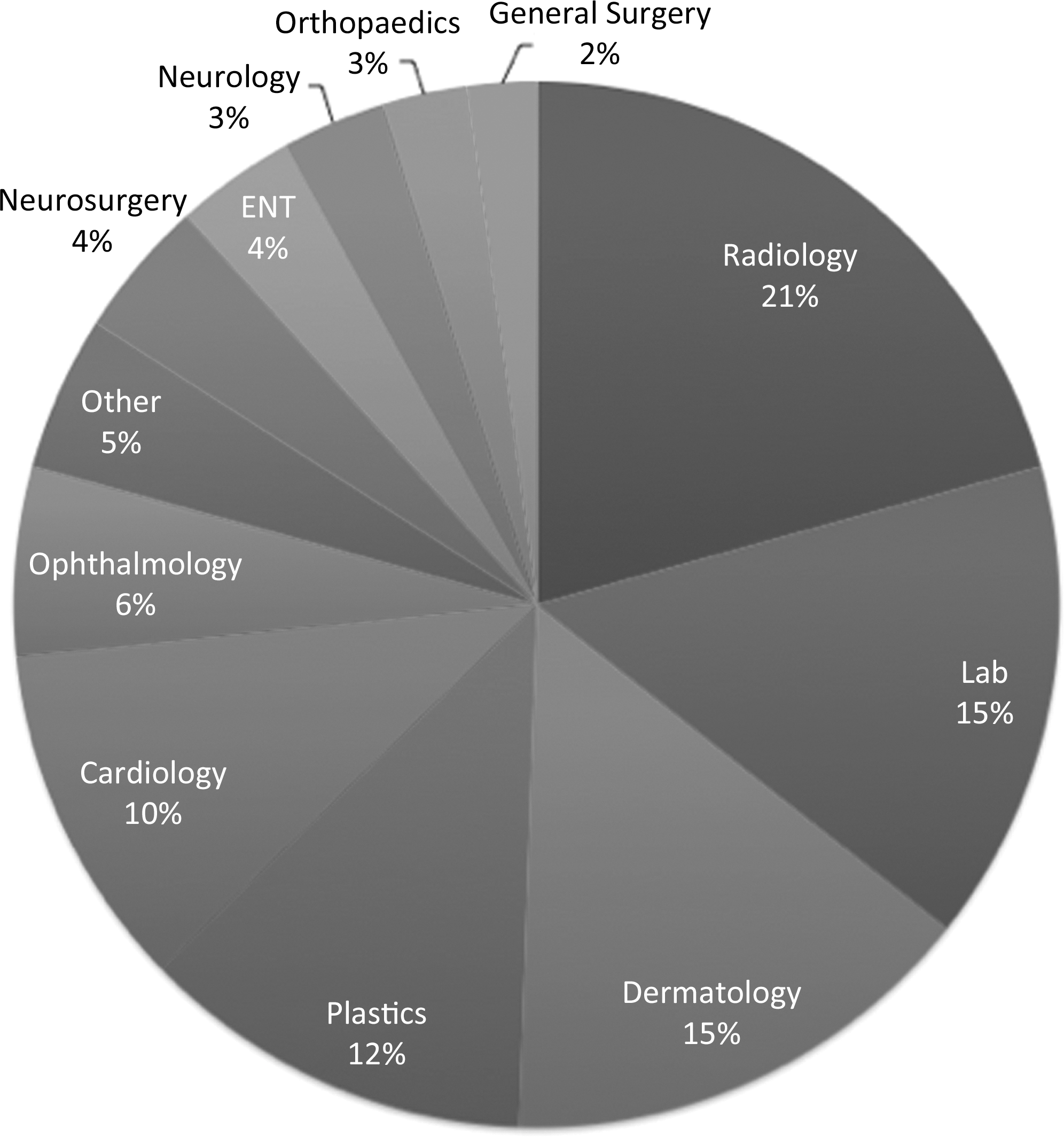
Proportion of publications contributed by different medical specialties.
In our review, we have chosen to discuss articles that focus on providing clinically applicable information.
Imaging in the Laboratory and Basic Sciences
One of the more novel fields of m-health emergence is in its role as a diagnostic instrument in the laboratory. In the context of the detection of an ovarian cancer biomarker, Wang et al. 7 developed a cell phone–based charge-coupled device coupled with an inexpensive microchip to perform enzyme-linked immunosorbent assays, which allowed colorimetric analysis of urine samples. This system had a sensitivity of 89.5% and specificity of 90% to detect the HE4 biomarker. The study demonstrated high reproducibility of measurements in three independent experiments carried out by multiple operators. Although this was a preliminary study, it showed the potential for mobile devices to overcome the need for conventional bulky, expensive spectrophotometers that are currently used.
Low-cost non-proprietary testing for tuberculosis specimens has been developed; however, these still require skilled personnel to observe and grade the microscopic slides. Zimic et al. 8 demonstrated that smartphone cameras were adequate to capture images of microbiology culture plates taken through a standard microscope that were then sent to experienced, trained personnel who were off-site to comment on the image. The authors demonstrated 98.7% (74/75) concordance of readings between the standard light microscope and the mobile phone–transmitted image.
Similarly, Tseng et al. 9 developed a 38-g, compact, holographic microscope adaptor that transformed the conventional cell phone light-emitting diode into a digital microscope. In this case, samples of patients with Giardia lamblia were loaded from the side of the adaptor, and incoherent light-emitting diode light was scattered from each microscopic object to coherently interfere with background light. This created a lens-free hologram of each microscopic object that was reconstructed through digital processing on the phone itself. Although this study was limited by lack of a gold standard control group, it has set the platform for the emergence of fluorescent microscopic and flow cytometric techniques to be performed using mobile phones.
A comparative study by Zhu et al. 10 showed that a compact, light-weight, disposable microfluidic channel positioned above the existing camera of a cell phone was of equal sensitivity to a conventional hematology analyzer in rapidly imaging body fluids for conducting cell counts. The microfluidic device acted as a optofluidic wave guide to guide the excitation of light as it passes through a fluid specimen. The cell phone camera was able to record the fluorescent movies of the specimen as it passed through the external microfluidic channel. This has significant applications in monitoring conditions such as viral loads and CD4+lymphocyte counts in human immunodeficiency virus and in measuring presence of water-borne parasites that affect millions worldwide.
Radiology
Abdominal computerized tomography (CT) is commonly used for the surgical evaluation of patients with suspected appendicitis. Choudhri et al. 11 showed a 98% concordance in diagnosis of acute appendicitis when abdominal CT scans of 25 patients with right-sided abdominal pain were interpreted on a smartphone (iPhone®; Apple, Cupertino, CA) using a DICOM viewer application compared with a conventional computer workstation.
Furthermore, Yaghmai et al. 12 showed that in patients with head trauma transmission of CT images could be rapidly and reliably performed using commercially available software on a personal digital assistant or smartphone. In this particular study the authors demonstrated that the entire process from image capture to review by a specialist took on average 11.5 min, which facilitated rapid referral to trauma radiologists and neurosurgeons. A novel expansion of this technique is the popular use of smartphone video capacity (video multimedia messaging service) to capture and send multiple CT scan slices in an efficient manner. This application is particularly useful when transferring a large volume of images that are all required to form a full clinical judgement, 13 for example, in neurosurgery where a whole series of neuroimaging was sent to off-site consultants after a video was taken from a series of CT slices being shown on a computer monitor. 14 Overall, the current studies are limited by small numbers and lack of a gold standard reference. However, these examples highlight a growing utility of smartphones to display images of sufficient quality for remote diagnosis of clinically significant pathology.
In addition, Huang 15 demonstrated that a smartphone connected to a 10-MHz ultrasonic surface transducer was able to perform spectrographic analysis of Doppler ultrasound. The study demonstrated the potential of using the smartphone as a portable medical ultrasound device. However, given the paucity of comparison with gold standard measurement, this remains an exploratory instrument.
Dermatology and Plastic Surgery
The most prolific usage (by publication volume) of smartphone cameras has been in the field of mobile teledermoscopy. Kroemer et al.,
16
in a well-designed, randomized study of 278 patients, demonstrated high sensitivity and specificity and strong correlation of mobile teledermoscopy compared with conventional clinical examination in the assessment of benign and malignant pigmented and unpigmented skin lesions. Similar studies have consistently demonstrated adequate diagnostic accuracy of clinically significant skin lesions such as skin cancers.
17,18
An important challenge of teledermoscopy studies remains the accuracy of image color sensitivity and saturation. Thus, despite their promising utility, future studies require verification of color sensitivity to reference clinical color photographs, which is complicated by the following technical factors: 1. Imaging sensor—This part of the mobile device allows it to capture the light energy into an electrical signal that can be processed. Color and contrast reproduction of a scene by a smartphone is thus dependant on the image processing algorithms used by the manufacturer. 2. Compression—Most images taken on mobile devices are stored in a compressed format, such as Joint Photographic Experts Group (JPEG). It is important to balance the need for small file sizes (e.g., when working in areas with poor Internet connectivity), compared with file sizes that convey sufficient information for adequate clinical judgment. This trade-off between file size and image quality needs to be assessed for each case-use scenario. 3. Display technology—The latest generation of mobile devices is also often bundled with high-quality displays, which are often higher quality than typical desktop displays. One caveat is the wide variation in display quality and calibrations between devices, and this needs to be accounted for in clinical usage. 4. Extensibility—By using various adapters, smartphones can be used together with existing equipment, although by using adapters, image quality can be affected.
Beyond diagnostic ability, teledermatology has evolved as an important avenue for patient follow-up in the setting of chronic skin diseases. Berndt et al. 19 reviewed a system of teledermoscopy composed of two main components: (1) dermoscopy performed using an app on a mobile phone that enabled the skin image and patient data to be transferred to a clinician and (2) an online portal for the care providers to interact with the patients themselves. The randomized study showed a feasible and safe system of teledermoscopy that could be performed for the management of chronic skin conditions such as eczema, psoriasis, and monitoring of postoperative wounds. Similarly, Pirris et al. 20 demonstrated that the status of surgical wounds in a cohort of neurosurgical patients could be reliably monitored remotely through patients sending photographs taken using cell phones to the treating medical team. Particularly for people residing in remote areas, this platform of teledermatology offers an important clinical adjunct without the inconvenience of travel and costs.
Growing numbers of observational studies have shown that m-health in plastic surgery has improved management of wound care, assessment of burns, and real-time monitoring of free-flap grafts. Hsieh et al. 21 showed that images of a broad range of hand and limb injuries presenting to a trauma hospital captured on a mobile phone were of sufficient quality to facilitate teleconsultation with the consultant surgeon in order to establish initial surgical management plans. It is noteworthy that the management decision was modified in 15% of cases when the patient was reviewed by the surgeon. Further studies are required to establish whether these cases where the management decision was modified compared with a standard voice-only telephone consultation.
Studies have demonstrated the utility of m-health imaging in time-critical plastic surgical cases such as postoperative monitoring of free flap grafts. Hwang et al. 22 demonstrated that monitoring and rapid notification of free flaps using a smartphone camera and communicating the images with clinical history using a messenger app increased the threatened flap salvage rate from 50% to 100%. This was partly facilitated by shortening the interval to the operating theater for patients requiring surgical re-exploration of potentially compromised grafts. Studies have shown that this concept of “real-time” monitoring of free flaps using smartphone photography and transferring images over a wireless network not only achieves comparable diagnostic accuracy to having a specialist on-site, but improves patient care by shortening the response time if wound threatening changes develop. 23
The sustainability of m-health imaging in dermatology and plastics is also dependent on the ease of use of the techniques described. In most cases, studies have shown that with minimal additional training, nonspecialist medical workers (doctors in training, nurses, and allied health workers) can be trained to perform simple tasks of image capture. Florczak et al. 24 showed that nurses were able to satisfactorily monitor pressure wounds, recognize changes in wound status, and determine the risk of severe skin damage in elderly residents of a nursing home using a smartphone camera. Similarly, in the setting of teledermoscopy, Chung et al. 25 showed that the technique could be easily taught to nonspecialists such as medical students and nurses and yet reproduce gradable images. However, there is a paucity of evidence comparing the diagnostic accuracy of trained professionals against specialists.
Although growing numbers of automated applications claim to accurately interpret images to categorize as benign or malignant, 26,27 Wolf et al. 28 highlighted in a study of 60 melanomas and 128 controls (pigmented, non-malignant lesions) comparing four popular apps that large variability existed in the diagnostic accuracy; three of the four smartphone apps failed to identify 30% of true melanomas. In this context, current evidence suggests that the most appropriate use of m-health in dermatology is for image capture rather than automated diagnosis.
Ophthalmology
Globally, refractive error remains the leading cause of all vision impairment. To address this, a novel adaptor to a conventional smartphone was developed. The pilot study by Bastawrous et al. 29 demonstrated in a nonrandomized control group study the ability for refraction to be assessed using a pinhole adaptor to an iPhone. The authors showed there was no statistically significant difference in the Near Eye Tool for Refractive Assessment adaptor compared with standard subjective assessment of a patient's refraction (spherical equivalence). Additionally, the low cost of these adaptors (estimated market price of U.S. $30) demonstrated the potential for such innovations to be cost-effective, particularly in low-resource settings where optometrists or trained refractionists are not readily available.
Commercially available slit-lamp adaptors have been demonstrated to be able to capture adequate quality imaging of the anterior chamber of the eye. 30 Lord et al. 3 have previously described retinal imaging using an iPhone and indirect lens. However, the sensitivity and specificity for imaging posterior segment (retina and optic nerve) disease using this technique are yet to be validated.
Lamirel et al. 1 demonstrated that retinal images taken using a non-mydriatic camera in an emergency department setting were able to be transferred and graded by an off-site ophthalmologist with high accuracy on an iPhone display to identify emergent retinal and optic disc pathology. Similarly, Kumar et al. 31 showed that retinal images of patients at minimum with moderate severity of diabetic retinopathy when read by a specialist on a smartphone achieved high concordance with images read on a standard office computer workstation. However, the study was limited by the small number of images with early, more subtle pathology being included for comparison.
The Expanding Role of M-Health Imaging in Other Medical Specialties
Bolkhovsky et al. 32 demonstrated the video recordings of fingertip pulsation using a smartphone camera could be used to monitor heart rate variability using principles similar to those of conventional photoplethysmography. Specifically, the photoplethysmography signal components around 0.1 Hz corresponded to the sympathetic component of the heart rate. 33,34 Tahat 35 extended this concept to demonstrate that mobile phones could receive electrocardiogram data from skin leads and record and transmit the information dynamically via multimedia messaging service to clinicians. The clinical implication of this would be of particular benefit for remote monitoring of people with cardiac arrhythmias and those with angina or coronary atherosclerotic disease who would benefit from ambulatory monitoring of their pulse rhythm and rate without wearing cumbersome equipment as occurs at present.
In neurosurgery, freehand placement of ventricular catheters into the brain has varying accuracy. As most patients will have had magnetic resonance imaging or CT of their brain, Thomale et al. 36 showed that entering basic dimensions using a smartphone-based algorithm assisted the surgeon in precise entry into the ventricles based on the individual's specific anatomy. A prospective randomized study is planned to compare the clinical utility of this technique to current clinical practices. Similarly, in the context of approach to the patient with significant laryngeal edema requiring advanced airway management, smartphone recording of videolaryngoscopy was demonstrated as a useful adjunct to plan conventional intubation methods. 37 The portability of smartphone cameras has also been shown to be of advantage in the management of dental emergencies. In a comparison among a special-purpose oral camera, a digital SLR camera, and a smartphone camera to capture images of the oral cavity, the smartphone camera provided the most convenient method while preserving quality necessary for initial diagnosis even at high compression ratios. 38
Potential cost savings in using smartphones for medical imaging were reported by Sohn et al., 39 who demonstrated that the resolution of images obtained from gastroscopy onto a smartphone (iPhone) were considered of comparable resolution to that of a traditional high-definition camera to make a clinical judgment; yet, the smartphone was reported to be 3,000 times cheaper than the high-definition camera. Other examples are provided whereby ambulatory monitoring of patients for the risk of common postoperative complications such as bruising, blood-stained bandaging, allergic reaction, bandage being too tight, and gait disturbances can all be monitored by the patient transmitting images taken on a smartphone from home. 40 –42
Ethicolegal Issues
Given that m-health imaging has only become popularized in the recent few years, it is not surprising that a 2012 review did not identify any clear guidelines specifically addressing imaging on smartphones.
43
Some important principles that clinicians need to take into consideration include consent,
44
privacy,
45
and secure storage
46
as summarized in the following: 1. Consent—Informed consent needs to be obtained, giving permission both to take the image and to transfer it to a third party, if that is its intended use. Ideally this should be documented in the patient's medical notes. 2. Privacy—Where possible, it is advisable to avoid identifiable patient features. 3. Secure storage—It is essential that mobile devices are secured with at least a PIN code to prevent access by unauthorized personnel, and where possible encryption of the device is recommended.
Discussion
A growing body of literature has demonstrated a spectrum of purposes where m-health has been applied across a myriad of medical subspecialties, particularly in the context of medical imaging. 47 Although m-health technologies have raised much interest in the medical community, that scientific rigor and sound principles of evidence-based medicine must also apply to m-health.
Recent meta-analyses of m-health have shown that there are currently few studies based on high methodological quality. In our review also, we found most studies to be exploratory in nature and attempt to prove a concept rather than validate these devices. 48,49 Limitations included the lack of objective clinical outcomes and the heterogeneity between reported outcomes amongst studies with similar interventions. Additionally, it was noted that the majority of studies were conducted in high-income countries. This limited the extent to which the results can be contextualized to low-resource settings, where m-health is positioned to make the biggest impact. Furthermore, there are few regulations or policies in place to ensure adequate quality in the delivery of medical imaging through m-health.
Despite this, medical imaging using m-health technology has shown several excellent examples by which it can facilitate healthcare. The existing concerns regarding limited high-quality research in m-health should guide the planning of studies that address methodological deficiencies in previous studies. This will ultimately enable medical imaging through m-health technology to be accepted as an important adjunct to the delivery of healthcare globally.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.