
Abstract
Introduction
The Australian Government spent $766 million for a new personally controlled electronic health record (PCEHR) system in 2012. 1,2 The PCEHR system was designed to improve accessibility to health services and patient information by creating a series of secure systems that consolidated information from multiple sources into a single record. Consumers could register for a personal record beginning July 1, 2012 on an “opt-in” basis. 1,2
There are theoretical benefits to a PCEHR. Some overseas reviews have suggested such systems achieve increased adherence to guideline-based care, enhanced surveillance and monitoring, and fewer medication errors. 3 –5 The main domain of benefit is reported to be in the primary healthcare sector, with the key outcome being decreased utilization of care. 5
However, other studies concluded there is little evidence that PCEHR systems improve patient outcomes and even less evidence that they improve efficiency of patient care. 4,6 In the United Kingdom a review of the implementation of a nationwide e-health record in secondary care reported that the implementation process proved “time consuming and challenging, with as yet limited discernible benefits for clinicians and no clear advantages for patients.” 3 The United States has fared little better. In 2009, the U.S. Congress passed the Health Information Technology for Economic and Clinical Health (HITECH) Act, allocating $30 billion in financial incentives to physicians and hospitals that adopted electronic health records. 4 Published results were disappointing. 7,8
Given studies where benefits have been identified relate predominantly to primary care and preventative health, one potential role for a PCEHR would be antenatal care. The Australian Government set a target that within a decade, a majority of Australian obstetric patients would use a PCEHR.
No data have surveyed the attitudes of Australian obstetric patients about their views on the PCEHR system compared with hospital-held paper-based records and/or patient-held paper-based record systems.
The aim of the present study was to survey consecutive antenatal patients to determine their preferred medical record system and if there were perceived benefits or concerns in relation to the PCEHR compared with existing hospital-held or patient-held paper-based record systems.
Materials and Methods
Institutional ethics committee approval was obtained. However, following formal consideration the project was deemed to be an audit and was approved by the committee as such.
Consecutive patients attending antenatal clinics at a large north metropolitan hospital in Western Australia were provided with information sheets that outlined the three types of medical records under consideration. These were: a. PCEHRs b. Hospital-held paper-based records (hospital-held) c. Patient-held paper-based records (patient-held)
The hospital-held system was in operation at the hospital at the time of survey, although patients also carried an abbreviated patient-held record.
Patients were provided with written information about each of the three systems before completing the survey. Information on the PCEHR came from Government Web sites to ensure accuracy. A media campaign on the launch of the PCEHR, funded by the Government to coincide with the launch of the PCEHR system, was underway during the survey period. To further familiarize patients, extracts from Web sites explaining the new system were available at the clinic where the survey occurred.
Patients completed the survey with a researcher (S.L.) or independently while waiting for their antenatal appointment. After patients completed the survey, forms were collected by reception staff. Data were entered onto a dataset and analyzed using Minitab® 16 software (2010; University of Melbourne).
To determine survey size, it was calculated that 50% of patients with a hospital-held record would express a concern for the variables under evaluation. A 15% difference in level of concern with either PCEHRs or patient-held records compared with the hospital held record system was considered significant. Assuming 80% power and significance set at 0.05, a sample of 364 patients was required. This sample was exceeded during the first survey period.
Quantitative data were presented as number and percentage for discreet variables and as mean and standard deviation for continuous variables that had a normal distribution and as median and interquartile range when the distribution was nonparametric. Chi-squared tests were undertaken to compare discreet data. A p value of 0.05 was considered significant. Qualitative comments were analyzed thematically in accordance with established methodology. 9
Results
In the 5-week survey period, 528 patients were booked to attend the clinical service. In total, 474 patients completed surveys. This represented a response rate of 89.8%.
Table 1 summarizes the demographic characteristics of the cohort. The mean age of the cohort was 29 years, and the median parity was 1, indicating that half the cohort already had one child and were pregnant again with their second child. Half the women were born in Australia, and nearly half had completed post-secondary education.
Demographics of the Study Cohort
Data are mean (standard deviation) values, number (%), or median (interquartile range) as indicated.
On a Likert scale of 0=not comfortable at all to 10=very comfortable and use for many daily tasks.
The cohort had access to and familiarity with computers and the Internet. Overall, 90.5% had a computer at home, and 87.1% reported their computer was connected to the Internet. When asked to describe their personal proficiency with computers, the respondents rated themselves highly (median score of 9 out of 10 on a Likert scale where 0 was not familiar and 10 was very familiar). Respondents identified that they were able to undertake multiple tasks using computers and accessed the Internet on a daily basis.
Figure 1 summarizes the first preferences of respondents for a medical record system. Nearly half the cohort preferred a hospital-held paper-based system. PCEHRs were preferred by a third of the cohort, and the remainder preferred a patient-held paper-based system. Overall, the options of hospital-held and patient-held systems were twice as popular as the PCEHR. There were no significant differences in preference by respondent age, computer access, Internet availability, and personal familiarity with computers (all p>0.05).
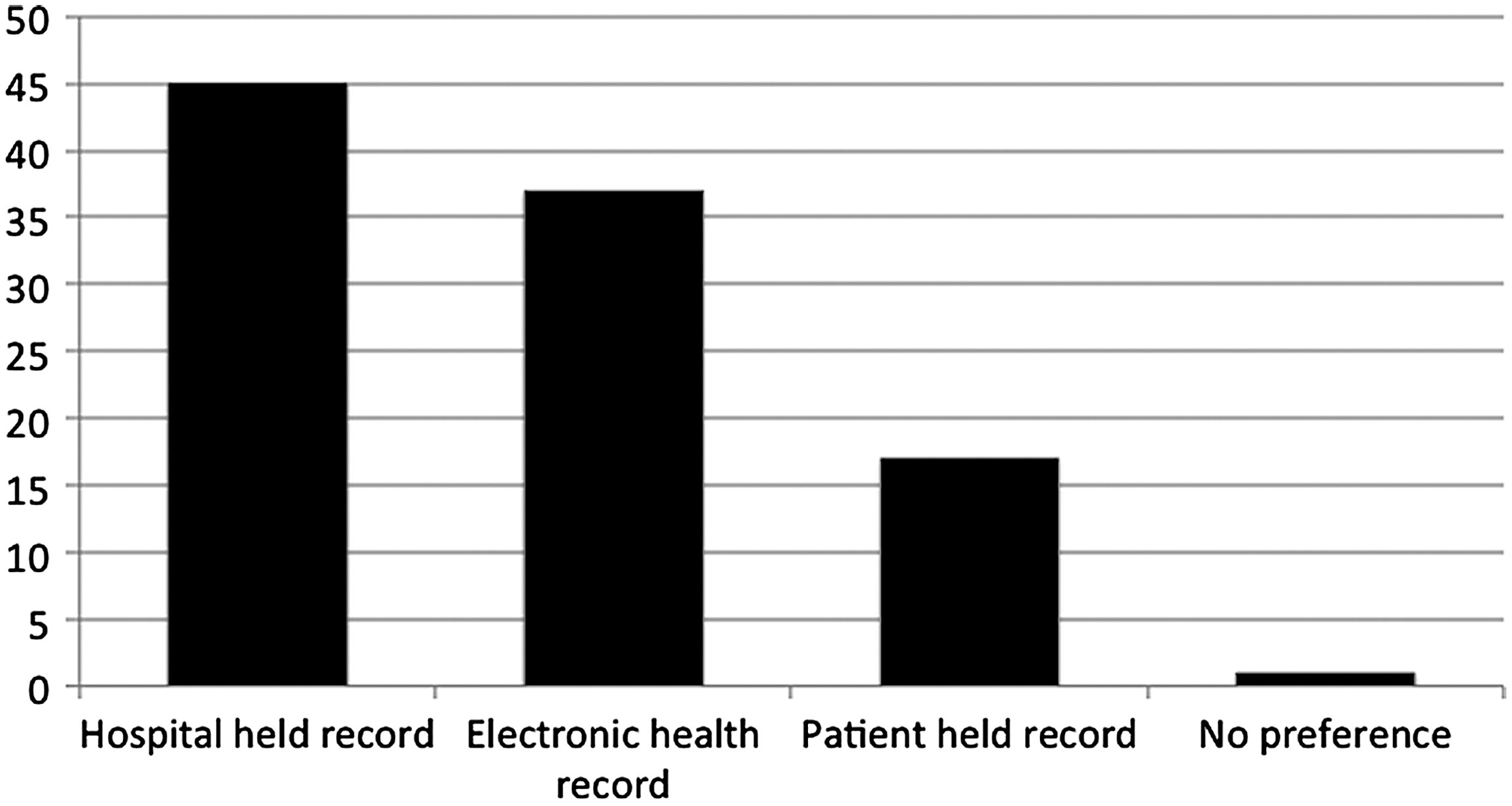
Patient preferences for medical record system. Choices were hospital-held paper-based record, personally controlled electronic health record, patient-held paper-based record, or no preference stated.
Table 2 summarizes the concerns expressed by women in relation to the different types of record system. When asked if record format would cause them to have a concern over their record being lost, respondents were significantly more concerned that patient-held paper-based records would be lost (p<0.0001) and significantly less concerned about PCEHRs being lost compared with hospital held paper-based record systems (p<0.0001). Thematic analysis supported the quantitative findings.
Patients' Concerns About Records
CI, confidence interval; OR, odds ratio; PCEHR, personally controlled electronic health record.
Regarding the patient-held record versus hospital-held record, one respondent said: I've lost the card I was given twice now and given up. I feel safer knowing the hospital has my file.
Regarding the PCEHR versus hospital-held record, another respondent said: I guess if it's on a computer file it can't get lost. My hospital record got lost once. But they did find it eventually.
When asked if record format would cause them to have a concern about poor communication between staff, responding patients had significantly fewer concerns about poor communication with both PCEHR and patient-held paper-based record systems compared with hospital-held paper-based records (p<0.0001). Thematic analysis supported the quantitative findings.
Regarding the patient-held record versus hospital-held record, one respondent wrote: It's good as I showed my card to the midwife and she gave me my injection for the blood ([sic] anti-D). Otherwise I would have had to wait to get everything checked again.
Regarding the PCEHR versus hospital-held record, another respondent said: I think it would help my GP know what the hospital were doing and stop tests being repeated.
However, with respect to concerns over confidentiality and privacy, respondents had significantly fewer concerns in regard to patient-held paper-based systems (p<0.0001) but had significantly more concerns in regard to the PCEHR compared with existing hospital-held paper-based systems (p<0.0001). Thematic analysis supported the quantitative findings.
Regarding the patient-held record versus hospital-held record, one respondent said: If I have it then no one else can see it unless I show it to them.
Regarding the PCEHR versus hospital-held record, another respondent wrote: You hear about people breaking into computers and stealing information. You know, like Wikileaks, only they just want to cause trouble. I'm not sure I want all my medical information out there to be discovered. Who reads it? I also don't want my husband or kids seeing things either and if its [sic] there they might want to see. I'm not convinced it would be safe.
With respect to concerns about a lack of control of their record, respondents expressed significantly fewer concerns in regard to patient-held paper-based records (p<0.0001) but had significantly more concerns in regard to the PCEHR compared with existing hospital-held paper-based record systems (p<0.0001). Thematic analysis supported the quantitative findings.
Regarding the patient-held record versus hospital-held record, one respondent said: I can control who sees it.
Regarding the PCEHR versus hospital-held record, another respondent wrote: They say that only you can see it, but in a few years that will change. All those politicians will want to ransack our records for things and you won't get a say in how they use them. Once somethings [sic] on-line you've lost control.
The two other major themes emerging from qualitative analysis related to the cost of the PCEHR system and a belief that electronic systems were the path of the future. In the latter case there were both positive and negative conclusions drawn by respondents.
Regarding cost, comments included: How much are they spending on all this? I'd prefer to see my money spent building hospitals. The problem with these systems is that as soon as they are built they are useless. Technology has moved on. I looked at this electronic system and thought it was already out of date. It's a waste of money.
Regarding the path of the future, in the positive side, comments included: Everything is on line now. I find a lot of it easier, like banking. Why should medical records be different? By the time my kids are my age paper will old fashioned. In school now they don't use paper. Why should hospitals be different?
Regarding the path of the future, concerns expressed included: Everything will be on line, but I wonder if it helps. We spend more time entering things on computers and lose the chance to speak to people. It's the future but I hate it. I can't see that medicine is better because doctors have my file on a computer. In fact, usually its [sic] worse. Half the information is wrong or out of date.
Discussion
Main Findings
The results of the present survey indicate that a hospital-held paper-based record system remains the most popular option. If the existing systems of hospital- and patient-held paper-based options were combined, they exceeded preferences for a PCEHR by a factor of 2. This is likely to reflect the respondents' familiarity with existing systems, despite being well educated, computer literate, and having good access to the Internet.
It is interesting that age, computer access, Internet availability, and personal familiarity with computers did not impact upon preferences. The age and parity of the sample were similar to those of the wider Australian maternity population. 10
Respondents identified two areas of advantage of PCEHRs compared with hospital-held paper-based records: they identified fewer concerns about record loss and poor staff communication. However, they expressed significantly more concerns about confidentiality and privacy, as well as loss of control, with a PCEHR compared with the existing hospital-held system. It is interesting that the fewest concerns were in regard to the patient-held system, even though they were the least preferred option!
Since July 1, 2012, the PCEHR system has been an “opt-in” system. This has meant that individuals with confidentiality and privacy or loss of control concerns did not have to register for a PCEHR.
Concerns over privacy and data security would appear to have some foundation. One review highlighted the threat posed by hackers in regard to electronic health record systems; several hospitals have faced payouts as a result of privacy and data security breaches. 11 One U.S. FBI investigation into the hacking of a computer system at a medical facility found that “the system had been hacked into by 11 other groups before the breach under investigation had been identified.” 11
There is evidence from the private healthcare sector in the United States that some consumers with concerns over loss of security and privacy have transitioned their healthcare contracts to companies that do not use electronic health records. 12 Data from New Zealand also reflect concerns over data security. The New Zealand consumer patient survey reported high levels of concern about hackers (79.4%), vendor access (72.7%), and malicious software (68%). 13
Of note is that respondents expressed significant concerns they would lose control of their record under a PCEHR system. This view differs from those of high-profile consumer advocates on government committees who have vocally welcomed the benefits for consumers. The chief executive officer of the Consumer's Health Forum was quoted as stating recently that a PCEHR system would result in a chance for consumers to take greater control of their health. 14 One potential loss of control manifestation may result from data entry errors that may subsequently be transcribed from one provider to the next without the safety check of consumer involvement. Instances of inaccurate data, particular in regard to prescribed drugs, were observed in an evaluation of the English Summary Care Record. 15 Patients were found to have drugs listed that they were not prescribed, and in other cases medications they utilized were omitted from the record. 15
Our results suggest that there remain concerns over privacy and control that will need to be addressed before some members of the public embrace a PCEHR system in antenatal care.
Overall uptake of the Australian PCEHR system has fallen behind target. On May 4, 2013, the National Clinical Lead on the National E-Health Transition Authority advised that 125,000 Australians had registered for a PCEHR since its launch. 2 This was against a background target for the first year of 500,000. Other reports suggest even this figure is optimistic. One media report stated that by March 2013 there were only 73,648 consumer registrations. Furthermore, of those registered, there were only “108 shared health summaries and 51 discharge summaries uploaded into the PCEHR system that consumers could share with their healthcare providers.” 1
Consumer concerns over cost were one of the additional themes to emerge from the qualitative analysis. Economic forecasters predict growth within the information technology field may exceed 15% for the industry as a whole, largely attributable by the healthcare sector. 2
Another layer of complexity results from burgeoning numbers of single-purpose electronic systems that deal with a specific local demand such as patient bookings, discharges, or medication systems. Individual systems may be developed and championed within institutions by clinician-linked developers. Given the myriad of competing programs and demands, budget blowouts and implementation delays can occur. In Australia, the planned opening of a new $2 billion healthcare facility was delayed, predominantly because of information technology complexity. 16 The final theme to emerge was the feeling that the introduction of electronic records was inevitable. It is interesting that comments were equally divided between this being a positive and negative concept.
This study focused on patient attitudes. However, other studies have reported that hospital staff and administration are also barriers to the implementation of electronic health records. Barriers to use and implementation have been documented by nursing and medical staff as well as by administrations fearing cost overruns and failure of systems to integrate. 1,3,6,7
Strengths and Limitations
The study has the strength of including a consecutive patient sample that reflects the wider demographics of the Australian maternity population in terms of age and parity. Patients had the option to complete the survey directly, by writing their answers, or via a research assistant. The survey coincided temporarily with the media promotion of the new PCEHR system, and the subject matter was therefore topical for respondents and helped achieve a high response rate.
The study also has several limitations. First, data are derived from a single institution. The responders had high levels of access to computers and the Internet. However, we did not find differences in attitudes by computer familiarity or access. Second, hospital-held and patient-held systems were in operation at the hospital and may have influenced respondent preferences because of their familiarity.
Interpretation
Given that national uptake of the Australian PCEHR is below target, patient concerns over confidentiality, privacy, and control need to be addressed.
Conclusions
Information technology systems offer potential benefits in healthcare outcomes, but for such systems to be embraced by consumers, the concerns identified in this article need to be addressed.
Footnotes
Acknowledgments
We acknowledge the women who completed surveys.
Disclosure Statement
No competing financial interests exist.
J.A.Q. and R.W.P. designed the study and obtained ethics approvals. S.L. implemented the survey and entered data. J.A.Q. analyzed the study and wrote the draft manuscript. All authors approved the final manuscript.