
Abstract
Introduction
Survival following the surgical management of cyanotic congenial heart disease in neonates has improved dramatically over the past 30 years, 1,2 including the survival of infants with hypoplastic left heart syndrome (HLHS). 3 Prior to the surgical innovation of the modified Norwood procedure, now called stage 1 palliation (S1P), mortality for HLHS was greater than 90% in the first month of life, whereas current initial survival following hospital discharge has reached 90% in some centers. 1,4 –6 Despite this drastic improvement in treatment, infants with only a single ventricle (SV) who require initial palliative surgical procedures continue to have a high rate of sudden death following hospital discharge that varies between institutions and can be as high as 20%. 7 –11
The current clinical consensus is that these SV infants are at particularly high risk for sudden and unexpected clinical deterioration owing to their dependence on very small, surgically implanted conduits or stented blood vessels to distribute blood flow from an SV chamber between the lungs and the rest of the body. Blood flow distribution in SV physiology is very sensitive to changes in cardiac function and rhythm, intravascular volume (hydration), and vascular resistance (blood pressure). 12 Unfortunately, signs and symptoms prior to clinical deterioration in these palliated SV patients are often subtle or absent. Following the initial description that frequent postdischarge telephone surveillance 13 resulted in reduced rates of postdischarge deaths in palliated SV patients, many congenital heart surgical programs began to implement similar approaches. 14 These strategies depend on parents or care providers to document daily records of infant weights and noninvasive oxygen saturation by pulse oximetry, respond to intermittent telephone contact between clinical staff and parents, and participate in more frequent follow-up outpatient evaluations. This home monitoring approach has been shown to reduce the number of outpatient visits, improve survival, and shorten the time between S1P and stage 2 palliation (S2P). 10,13 Because of this success, routine postdischarge SV home surveillance is incorporated into the National Pediatric Cardiology Quality Improvement Collaborative, which is evaluating and optimizing the variation in outpatient care for infants following discharge after S1P. However, there can be considerable variation in the frequency of communication among outpatient cardiologists, primary care physicians, and care providers, nutrition route at discharge, and home surveillance strategies. 15
The rapid expansion of electronic home telemonitoring solutions has shown very favorable outcomes in reducing unexpected clinical events in adult patients with chronic medical conditions. 16 –19 However, there has been limited published experience with telemonitoring in pediatric patients. 20 –22 An initial experience using a home telemedicine system for pediatric SV patients had positive results on interstage weight gain but not on interstage mortality. 23 This pediatric cardiology pilot project included monthly outpatient SV patient visits, a 24/7 telephone call network, and a telemonitoring system that transmitted peripheral oxygen saturation and heart rate to a centralized Web site. Additional data, including weight, caloric intake, and data from a 5-point questionnaire, were manually recorded and transmitted by parents. The system included automatic clinician alarm triggers as well as triggers related to missing data. 23
We launched a pilot home telemedicine project in order to determine the feasibility of implementing a daily pediatric home telemonitoring solution for infants following palliation for SV heart disease with the goal of reducing interstage unanticipated adverse events: primarily unscheduled emergency room visits, hospitalizations, and death. The system was designed to provide daily transmission of subjects' peripheral oxygen saturation and weight along with the parental response to 10 clinically relevant questions with data collection and review via a customized WebPortal. Our initial experience provides insights into the complexities and challenges of this approach.
Subjects and Methods
Enrollment and Disenrollment
Subject enrollment began following University of Louisville and Norton Healthcare Office of Research Administration Institutional Review Board protocol approval. Selection criteria for historical controls (HC) inclusion were the presence of cyanotic congenital heart disease (CHD) with SV physiology and palliative surgical management with either a modified Blalock–Taussig (BT) shunt or a hybrid interventional catheter+surgical procedure. These patients were considered to have “shunt-dependent” SV physiology. Additional selection criteria for subjects enrolled in the telemedicine trial (enrolled subjects [ES]) included care provider availability for daily telemedicine data transmissions and English language skills. Disenrollment criteria for ES included failure to transmit data for >7 days (not based on equipment malfunction) or unanticipated death. Following the initiation of the project, the first 2 ES were enrolled approximately 1 month following S1P as outpatients. All subsequent ES were enrolled during their initial inpatient hospitalization. Prior to closing the study, we enrolled and trained with mobile telemedicine equipment 9 of a goal of 16 subjects. We collected clinical data related to cardiac diagnosis and both medical and surgical management for 9 HC and all ES. We closed the study to additional subject enrollment after enrolling 9 ES because of sudden deaths in 2 of 9 enrolled ES (22%) versus 1 of 9 HC (11%).
Study Design and Data Flow
Our study design and telemedicine data flow are outlined in Figure 1. We abstracted de-identified data from the clinical record for all HC and ES. Telemedicine-transmitted data were de-identified, stored in the WebPortal, and analyzed by the research team.

Pediatric cardiac telemedicine project design and data/communication flow. Clinical data abstracted from enrolled subject records were de-identified and analyzed by the research team. Telemedicine data were de-identified, stored in the WebPortal, and analyzed by the research team. Direct communication between the enrolled subjects and clinical cardiovascular (CV) specialists was maintained throughout the study.
Telemedicine Equipment, Data Transmission, and Data Analysis
The telemedicine equipment and customized software for the study were purchased via a research contract between the University of Louisville Research Foundation and Intramed, Inc. (Copenhagen, Denmark) (
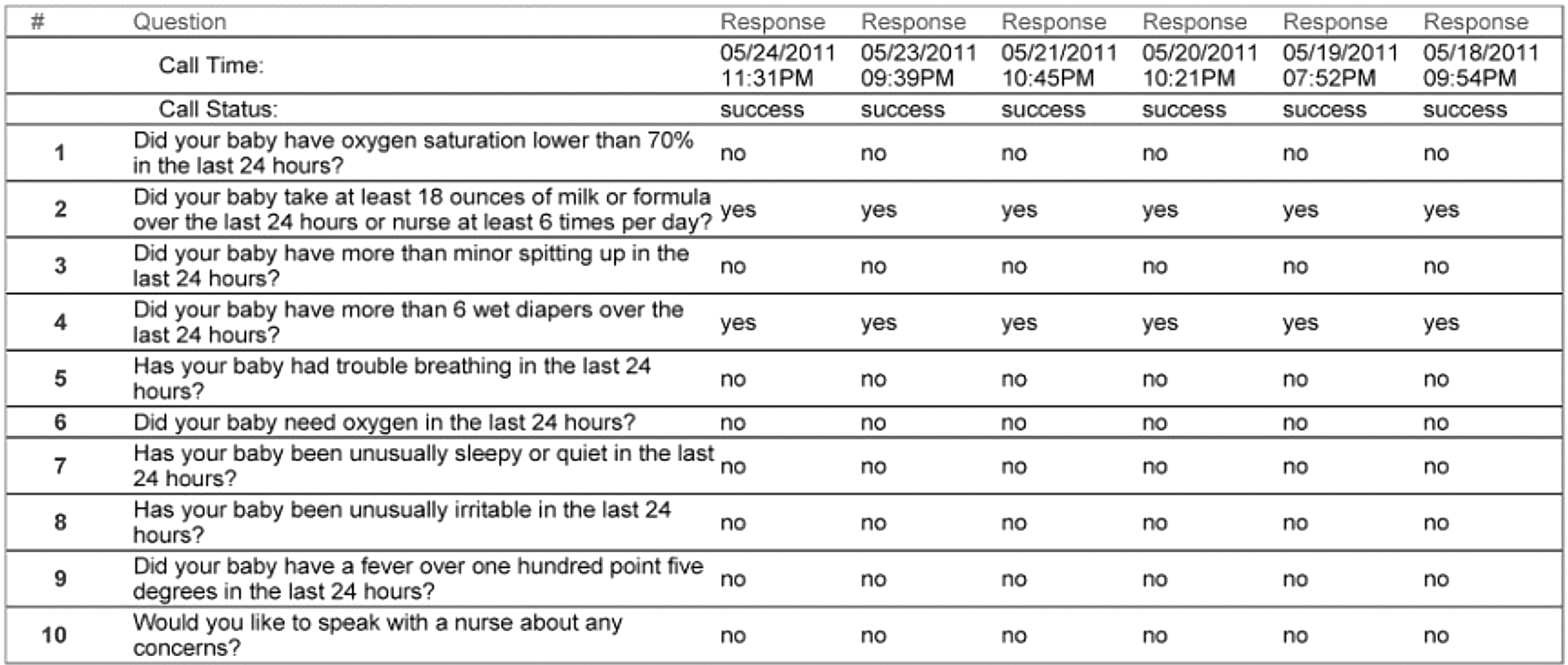
Representative parental data transmission-activated interactive voice response questionnaire with 7 days of responses. Note that all responses were yes/no rather than numerical or free text.
Provider Training and Contact Instructions
At the time of subject enrollment we provided training on the use of the telemedicine equipment and the questionnaires. We used a dedicated clinical research assistant to monitor project data and be available to answer parent questions during routine office hours (8 a.m. until 5 p.m., Monday through Friday). Subject parents were instructed to contact our research office for questions related to the telemedicine project equipment and activities and to contact their child's primary care physician or cardiovascular specialist for all clinical questions, including the management of urgent or emergency clinical issues.
Clinical Data Analysis
We collected clinical data on HC and ES relevant to their basic demographics, clinical diagnosis, procedures, and clinical course (Table 1). Variables of interest that could potentially impact clinical outcomes included maternal age, gestational age, birth weight, weight and age at the time of S1P, length of hospitalization at the time of S1P, and age and weight at the time of S2P. We analyzed the success of the outpatient telephone surveillance program based on completed calls, scheduled and unscheduled office visits, emergency department (ED) visits, hospitalizations, procedures, and adverse events, including death, for HC and ES groups. For the ES group we also determined the success rates for transmitting daily ES weights, oxygen saturations, and questionnaire responses. We generated a clinical course template, including a timeline (Fig. 3), with relevant events for each subject. We then analyzed the times between hospital discharge and office visits for HC and ES.
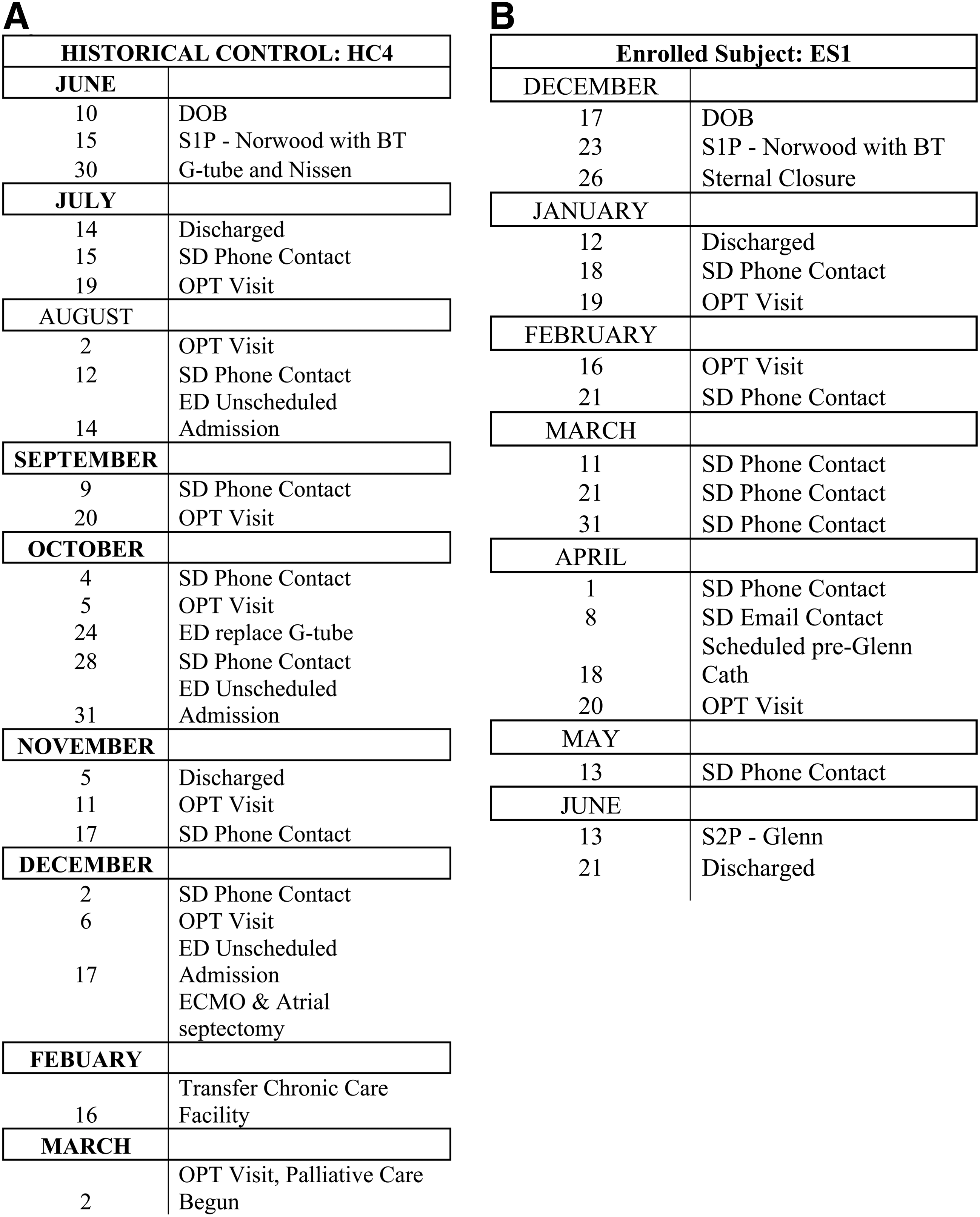
Representative clinical timelines for data collected from a representative
Anatomic Clinical and Procedural Data Collected for Historical Controls and Enrolled Subjects
AA, aortic atresia; AS, aortic stenosis; BT, modified Blalock–Taussig; DILV, double-inlet right ventricle; DORV, double-outlet right ventricle; HLHS, hypoplastic left heart syndrome; HRHS, hypoplastic right heart syndrome; IVS, intact ventricular septum; MA, mitral atresia; MS, mitral stenosis; PA, pulmonary atresia; PDA, patent ductus arteriousus; RVOT, right ventricular outflow tract; TA, tricuspid atresia; TGA, transposition of great arteries; VSD, ventricle septal defect
Statistical Analysis
Clinical data were summarized as mean±standard deviation values. Statistical differences between the ES and HC groups were determined for continuous variables using unpaired Student's t test with significance assigned to a p≤0.05 and a fold change of ≥1.5. The small sample sizes limited the power of the statistical analysis.
Results
Patient and S1P Variables
The anatomic diagnosis and initial intervention for each ES and HC are summarized in Table 1. All of the ES and HC had complex cyanotic heart disease requiring at minimum a modified BT shunt for intervention. No patient received a heart transplant as primary treatment. The HC comprised subjects with HLHS (56%), hypoplastic right heart syndrome (22%), and tricuspid atresia (22%). For the ES the anatomic diagnoses included HLHS (78%), double-inlet left ventricle (11%), hypoplastic right heart syndrome (11%), and double-outlet right ventricle (11%). The procedural palliation for the HC group included the Norwood procedure (33%), a hybrid procedure (11%), and varying types of modified BT shunt (55%). The procedural palliation for the ES included the Norwood procedure (67%), a hybrid procedure (22%), and the Damus–Kaye–Stansel procedure (11%). Table 2 summarizes the clinical variables for ES and HC, and Table 3 summarizes the procedural data for ES and HC. There were no significant differences between the gestational age, age at S1P, weight at S1P, or hospital stay following S1P. The mothers of the ES were significantly younger than those of the HC (p=0.02). The youngest maternal age in the ES was 17 years old versus 30 years old for the HC.
Variables of Interest Selected Based on Potential to Impact Clinical Outcomes for Historical Controls and Enrolled Subjects
p<0.05.
SD, standard deviation.
Procedural Data and Significant Clinical Events for Historical Controls and Enrolled Subjects
ECMO, extracorporeal membrane oxygenation; ED, emergency department; G-tube, gastrostomy tube; SD, standard deviation.
Interstage Outpatient Course and Morbidity/Mortality
The postdischarge course of both ES and HC revealed substantial variation in the schedules for outpatient follow-up for infants after S1P discharge as displayed in the outpatient follow-up graphs (Fig. 4). Clinical parameters, including postoperative extracorporeal membrane oxygenation, days to sternal closure following S1P, the need for gastrostomy tube feedings, and unscheduled outpatient or ED visits, showed no statistical difference between the ES and HC groups. Although there were more total unscheduled ED visits for the HC (n=11) versus ES (n=9), there was no significant difference in the number of unscheduled, non–feeding tube-related ED visits. There was also no significant difference in the number of hospital admissions from the ED between the ES (n=9) and HC (n=11). The age and weight at S2P for the two groups were similar. Interstage death (ISD) occurred in 1 of 9 HC (11%) and 2 of 9 ES (22%). Sudden death occurred in 1 ES without symptoms or change in saturation (reported) within 2 h before clinical collapse. ISD also occurred in 1 ES following disenrollment due to study noncompliance.

Representative examples of the variability in days between scheduled outpatient office visits for
Telemedicine Monitoring Technical Issues and Success Rates
There were several basic technical issues identified during the study. First, many of the ES were noted to have inconsistent pulse oximetry readings between the original pulse oximetry sensor compared with oximetry data generated by the hospital-prescribed Masimo oximeter. We located a flexible digital sensor similar to the design used with the Masimo oximeter for the final ES that resulted in comparable oxygen saturation recordings. ES parents all commented on their frustration using the original oximeter sensor on the post-study questionnaire. Unfortunately, the study oximeters were digitally coupled to the telemedicine hub, preventing the use of transmitted digital data from the Masimo oximeters. It is important to note that all clinical decisions were based on Masimo-derived oximetry data. There were no issues with the operation or transmission of digital scale data. However, there were technical issues related to the quality of landline signals in some rural locations, and therefore all subsequent ES utilized telemedicine hubs with cell phone modems.
The days from discharge to enrollment took on average 18 days. The average amount of time after discharge for a subject to transmit data was 3 days, with the main reason for delays being technical limitations due to equipment or parental noncompliance (Table 4). On days when data transmission failure occurred, all three data components (weight, saturation, IVR) were usually absent (57%). Less frequent was the isolated lack of oxygen saturation data (14%) (Table 5). When the research team noted a lack of data transmission, the parents of ES were contacted via e-mail and/or cell phone to identify and resolve any technical issues. However, it was difficult to determine if lack of data transmission occurred because of study noncompliance or to technical issues. One ES required replacement of a cell phone modem. Reasons for data transmission noncompliance revealed by the exit survey included that an ES parent was out of town, there was a scheduling conflict, or that the parent simply forgot (Table 5).
Analysis of Enrollment and Transmission Successes and Failures
Three subjects had significant lags in transmission. All inpatient days were excluded from total enrolled days and transmission percentage calculations. Complete transmission required transmission of weight, oximetry, and interactive voice response data.
Disenrolled because of parental noncompliance.
Death.
Technical issues with equipment.
ES, enrolled subjects.
Analysis of Partial or No Data Transmission by Parents of Enrolled Subjects
Data were taken from exit survey written data.
IVR, interactive voice response.
Post-Monitoring Survey
Exit survey information was returned by four of five parents of enrolled subjects and is highlighted in Table 6. Five of nine parents of ES completed exit surveys. Based on the survey, parents felt that their training session prior to discharge helped them feel confident to use the home telemedicine equipment. The equipment appeared easy to use, and the IVR and digital scale received average satisfaction scores of 4.25 and 4.75 out of 5, respectively, for ease of use. As we expected, the pulse oximeter had the lowest score for ease of use (e.g., 3 out of 5). The parents of the final ES, who used the new oxygen sensor, gave the pulse oximeter a 5 out of 5 and stated that all of the equipment was easy to use. The system was reported to take an average of 8 min/day for the family to use, and parents generally agreed that the daily monitoring gave them peace of mind. The amount that the parents would be willing to pay each month to use comparable telemedicine equipment in the future ranged from $0 to more than $100 per month.
Analysis of Exit Survey Data Compiled from the Parents of 4 Enrolled Subjects
On a scale of 1=strongly disagree, 2=disagree, 3=agree, and 4=strongly agree.
ES, enrolled subject; IVR, interactive voice response.
Discussion
The primary goal of our study was to evaluate the feasibility of establishing a telemedicine approach to increase the frequency and the accuracy of collecting potentially clinically relevant data in infants with CHD after they have undergone initial surgical palliation. These infants are at high risk for clinical deterioration and/or death while awaiting subsequent palliative surgery. Although the problem was initially logistically challenging, we were able to generate a customized telemedicine solution that included the transmission of subject weight, oxygen saturation, and IVR-documented clinical parameters that resulted in both increased frequency and content of transmitted data versus traditional methods that depend upon clinical follow-up telephone calls.
As would be expected of ES from both urban and rural settings, we noted variable access to adequate quality landlines or cell phones for data transmission. One candidate subject could not be enrolled because of the lack of dependable cell or landline phone access, and the study was not designed to provide cell phone service to ES.
We identified an initial technical problem with the accuracy of recording pulse oximetry data using the supplied oxygen sensor. The problem was solved before the enrollment of ES number 9. The delay in identifying an oxygen sensor to replace the original equipment and to integrate it into the system was primarily a function of the limited number of vendors with sensors developed and validated for infants. Fortunately, all ES were also prescribed a Masimo oximeter, and data from that oximeter were used for clinical management. For subsequent studies our preference would be to couple the Masimo oximeter for data collection and transmission in place of the initial study oximeter.
Analysis of the clinical timelines of the HC and ES in our study revealed extremely variable outpatient courses with respect to scheduled follow-up visits and unscheduled office, ED, and hospital admissions. The variability was due in large part to the medical complexity of the CHD as well as to noncardiac issues for each subject.
A previous study published by Cross et al. 23 in 2012 reported that use of a telehealth system for home monitoring of SV-pathology infants is feasible and may provide improvements in nutritional status at S2P. Our study attempted to gain further insight into the challenges post-S1P discharge by also including automated pulse oximetry data transfer as well as weight scales that did not require manual input from care providers. In addition, our daily 10-point questionnaire was automatically triggered following the transmission of weight and oximetry data and utilized a voice script to prompt simple manual responses.
Although our study failed to achieve the primary end point of reducing ISD and unscheduled events, there were several important observations gained from the daily monitoring of ES. In contrast to the study by Cross et al., 23 their primary end point of weight at S2P was not significantly different between HC and ES in our study. However, it is worth noting that the two youngest and lowest weight infants at S2P in the ES underwent earlier palliation as a result of their participation in our project.
ES6 was disenrolled from the study because of the mother's inability to comply with study guidelines and failure to respond to the research team after multiple attempts to make contact. At disenrollment the extent of parental noncompliance with the study resulted in a decision by the clinical team to proceed with earlier S2P in this high-risk infant. S2P for ES6 occurred without complication. Similar noncompliance was noted in the parents of ES8. However, shortly after disenrollment and prior to S2P, this infant suffered ISD. Telemedicine-transmitted data for ES9 showed low oxygen saturations and suggested brief episodes of tachycardia that resulted triggered two unscheduled ED visits. Therefore, ES9 was also scheduled for an earlier S2P than was initially planned, which was successful.
The observed noncompliance with this telemedicine project provides some insights into the limits of care providers to manage the medical complexity of these high-risk infants. These results suggest that daily telemedicine monitoring can expose at-risk social situations in addition to the primary goal of identifying altered clinical status.
Technical Limitations
Our study faced a variety of technical limitations during the course of implementing and operation. The use of an external vendor (and subcontractor) to provide telemedicine software and hardware had both advantages and disadvantages. Following substantial delays related to contract and invoice resolution, we had additional delays related to the timely resolution of both software and hardware issues. Although there was no resulting compromise of the clinical status of ES by any technical issues, there were gaps in data collection that likely could have been avoided with another vendor.
The major hardware challenge related to the reliability of the vendor-provided reusable pulse oximeter sensor compared with the commercial Masimo sensor. The inaccuracy of the original sensor made it impossible to utilize in the data analysis. In changing the pulse oximeter sensor for the final ES to one similar to the disposable Masimo sensor used in the hospital, this issue was resolved, giving accurate data transmission for the final ES. Furthermore, it was clear on the exit surveys that parents who were given the original sensor found this piece of the equipment difficult to use, which prompted replacement with a more effective sensor. Future hub configurations could incorporate the digital output from the Masimo system, avoiding the need for an independent oximeter.
Independent of the vendor and oximeter issues was the issue of variable access to reliable data transmission. Although landline transmission resulted in more consistent data transmission from rural areas, not all subjects had a landline phone available. This made it necessary to utilize cell phone technology, which was not always reliable. Although the equipment for our study consistently worked in the university hospital setting during training, this did not always translate to successful monitoring in the ES home environments. This was a particular problem with ES7, who experienced rapid clinical decline on Day 16 that resulted in ISD. Because of the inability to transmit data for unclear technical reasons, no daily recordings were available prior to the infant's sudden clinical deterioration. Cross et al. 23 utilized a weekly home technical support option, but our study did not have home technical support and depended on remote technical support from the research team and/or AMC Health, which introduced substantial time lags into the resolution of some technical issues. Implementing home technical support would likely have more rapidly resolved data transmission failures in the ES home environment and should be integrated in future telemedicine programs.
Clinical Challenges
Our study did not result in a reduced number of ISD or unscheduled hospital visits in ES versus HC. This is likely due in large part to the medical complexity of this high-risk population, which was compounded by social factors impacting a parent's ability to comply with the study protocol. Paradoxically, the parents of several potential subjects declined participation because of what they perceived to be additional complexity to the postdischarge care plans. Thus, we were only able to enroll 9 subjects for our study over a total project time of 36 months. The inability to meet the primary outcome in an interim analysis led to the decision to terminate the program prior to reaching our enrollment goal of 16 ES. Although we were able to identify 1 ES with reduced saturation and possible arrhythmia resulting in early S2P and one noncompliant parent leading to early S2P, it was not clear that home telemedicine was more effective than an aggressive traditional home telephone surveillance. The current multicenter National Pediatric Cardiology Quality Improvement Collaborative, which is evaluating and optimizing the variation in outpatient care for infants following discharge after S1P, is likely to generate standardized surveillance guidelines and may incorporate home telemedicine monitoring for future infants following S1P.
Looking Forward
We anticipate continued evolution in the available software and hardware that can support home telemonitoring for pediatric patients with complex and high-risk chronic diseases. Our study uncovered the potential impact this technology can have on families with high-risk health problems as well as the substantial challenges encountered in launching a new telemedicine project. It is apparent from the exit surveys that the availability of home monitoring technology gave peace of mind to families and that it did require a significant amount of time for daily use. This increased patient confidence may reduce parental stress and aid parents in their ability to care for their high-risk infant.
Overall, our study provided further insights into the feasibility and potential for telemedicine monitoring in a high-risk infant CHD population. Despite the logistical challenges, great potential remains for innovative home telemedicine systems that improve the connectivity between high-risk patients and their healthcare providers.
Footnotes
Acknowledgments
This work was financially supported by a translational research pilot grant from the Office of the Vice President for Research and Innovation, University of Louisville (to B.B.K.), and the Kosair Charities Pediatric Heart Research Endowment (to B.B.K.). We also acknowledge the assistance of the following cardiovascular clinicians in clinical data collection: Renae Akins, Deborah Campbell, Tracy Dilling, and Terri Massey.
Disclosure Statement
No competing financial interests exist.