
Abstract
Introduction
The United States continues to rank poorly among industrialized nations in the “triple aim” of healthcare delivery—best quality of care, best access, and affordable costs 1 —while an aging U.S. population and shortages of intensivists, 2 critical care nurses, and clinical pharmacists 3 portend a dire lack between the supply and demand for critical care specialists, all while critical care costs are increasing. 4 Although access to critical care specialists improves patient outcomes, including reducing mortality 5,6 and decreasing costs, 7 fewer than 30% of U.S. hospital intensive care units (ICUs) now provide Leapfrog Group–recommended 24/7 intensivist staffing. 5,6,8,9 Those in rural and underserved areas are at particular risk for inadequate intensivist staffing. 10
Because roughly 85% of U.S. hospitals are community-based, with variable access to specialists, tele-ICU solutions (or “telecritical care” 11 ) are a growing trend. Simply stated, telemedicine is the “use of advanced telecommunications technologies to exchange health information and provide health care services across geographic, time, social, and cultural barriers.” 12 Among tele-ICU solutions, the Centralized Monitoring Model (e.g. Philips-VISICU-eICU™ [Baltimore, MD] 13 ) 14 has been heralded as one such advance, but the Virtual Consultant Model has gained attention as a possible alternative.
In this study, we systematically reviewed all available data associated with use of Centralized Monitoring and Virtual Consultant tele-ICU Models to evaluate impacts on clinical outcomes, financial sustainability, and ICU staff workflow and acceptance.
Materials and Methods
Technology
Nomenclature of tele-ICU systems is described elsewhere, 15 and we focus here on the most commonly used real-time (i.e., data transmitted “live” or within minutes) platforms.
The Centralized Monitoring (or “active” 16 ) Model involves real-time collection and delivery of primary continuous (24/7) clinical data streams, including vital signs, electronic medical record access, and markers of guideline compliance, 11,14,17 often through a secure T1 link that connects remote “spoke” site(s) to a “hub” monitoring facility, where a team of nurses, administrative assistants, and intensivists handles the information. Interaction with on-site providers (and direct patient examination and communication) is determined by the remote team based on clinical needs assessments. Although not mandatory, a fixed, centralized, and closed-communications platform in tele-ICU care is often used (Fig. 1a), of which there are several commercial vendors, including Philips-VISICU-eICU, 13 Cerner, 18 and iMDSoft. 19 Individual health systems have created similar centralized “hub-and-spoke” monitoring and in-house technological systems as home-grown solutions, such as iCare of Banner Health 20 or the Veterans Health Administration hospital network.

The Virtual Consultant (or “low-intensity passive” 16 ) Model, in contrast, utilizes technology to provide periodic, real-time interaction with staff and patients at a remote site without continuous data feeds that are processed by an off-site multidisciplinary team. Instead, a remote provider independently attends the patient and/or staff through a telepresence modality (e.g., a robot, pole- or cart-based videoconferencing hardware, or tablet with two-way video and audio connection) to provide clinical evaluation and treatment in the manner of an in-person consultant. As clinical information and contact are periodic rather than continuous, a portable, decentralized, and open-communications architecture platform (Fig. 1b) is most often used, of which several vendors offer portable robot units, 21 –23 cart-based units, 24 –26 and hand-held devices, including tablets like the Apple iPad®, 27 Samsung Galaxy Tab®, 28 Google Nexus, 29 and Asus Transformer Pad. 30
Search Strategy
We used the PRISMA Statement 31 to perform this systematic review (a comprehensive review of the literature using a priori appraisal criteria). 32 A medical reference librarian (L.M.) used guidelines on effective database searching 33 to search MEDLINE (via PubMed), Scopus, Web of Science, and the Cumulative Index to Nursing and Allied Health (CINAHL) using combinations of key words and, where appropriate, controlled vocabulary terms. We sought to identify all clinical studies addressing tele-ICU systems with the following key words: “tele-ICU,” “telemedicine ICU,” “remote presence ICU,” “teleconsultation ICU,” “telehealth ICU,” “electronic ICU,” “eICU,” “telematics ICU,” “remote monitoring ICU,” “remote consultation ICU,” “centralized monitoring ICU,” and “telecritical care,” with searches later supplemented with “and ICU.” We combined MeSH terms (“teleconsultation,” “telemedicine,” “telecritical care”) and CINAHL subject headings using Boolean operators. We included articles in all languages and synonyms for each concept and applied truncation where applicable (full-text of all search strategies available upon request). Additional studies were included after review of bibliographies of key articles.
We performed all searches on August 19, 2013 and included any data in the form of published studies, conference abstracts, written commentaries, and/or communications describing use of remote technology in clinical intensive care. To minimize risk of bias, two independent reviewers (V.R.R. and L.H.) reviewed abstracts and titles of all articles using inclusion criteria determined prior to screening; a third reviewer (N.K.) resolved disagreements (Fig. 2).
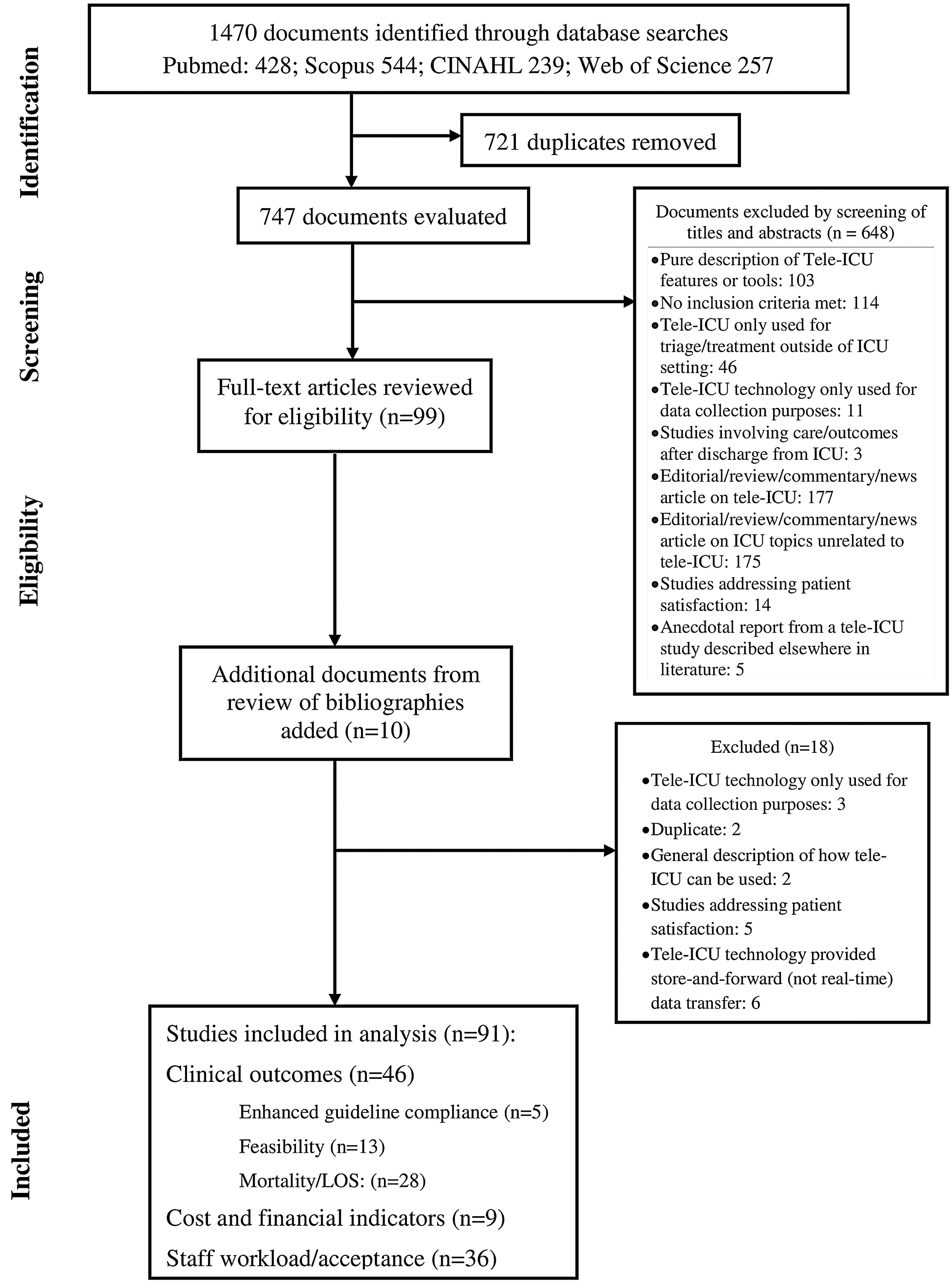
Literature search and selection. ICU, intensive care unit; LOS, length of stay.
Inclusion criteria were use of telemedicine in the ICU for critical care patients only and the presence of at least one of the following as a primary outcome of the study: (1) financial sustainability (e.g. costs, revenue, cost-effectiveness, billing), (2) clinical outcomes (e.g., mortality, morbidity, clinical practice guideline compliance), or (3) ICU workflow and acceptance (e.g. satisfaction).
Studies were excluded if they were (1) duplicate, (2) pure description of tele-ICU features or tools, (3) device manufacturer materials, (4) treatment or triage via tele-ICU prior to or after ICU admission, or (5) critical care intervention via tele-ICU received in a setting outside the ICU (e.g., long-term acute care hospitals, emergency departments) or if (6) tele-ICU was purely used for data collection purposes, (7) studied outcomes were unrelated to the ICU stay itself (i.e., for previously critical patients), or (8) the study was anecdotal or a case report from a larger tele-ICU study described elsewhere in the literature.
Included studies were analyzed for the primary and secondary outcomes and strength of the evidence, based on type of study. 34
Results
In total, 1,468 documents (1,400 in English, 68 in non-English languages) were reviewed. Of these, 1,371 were excluded: duplicates, 723; pure description of tele-ICU features and/or tools, 103; no inclusion criteria met, 114; tele-ICU used only for triage or for treatment outside of ICU course, 46; tele-ICU used only for data collection purposes, 14; studies involving care outcomes after discharge from ICU, 3; editorial, review, commentary, or news article-related (177) or unrelated (175) to tele-ICU systems; studies addressing patient satisfaction, 19; anecdotal report from a different tele-ICU study described elsewhere in the literature, 5; tele-ICU usage characteristic description only, 2; general descriptions of how tele-ICU can be used, 2; and tele-ICU technology provided store-and-forward (i.e., not real-time) data transfer, 6. After exclusion, the remaining 91 documents (Tables 1 –5) were categorized as follows: clinical outcomes (46 documents: 28 studies [60.8%] addressed length of stay [LOS] and/or mortality outcomes; 13 studies [28.2%] were feasibility studies; and 5 studies [10.8%] discussed enhanced compliance with existing practice standards), financial sustainability (9 documents), and ICU workflow and staff acceptance (36 documents).
Characteristics of Studies Addressing Financial Sustainability of Tele-intensive Care Unit Systems
Provided for quasi-experimental studies only by guidelines of Harris et al. 34
Technology categories are as follows: centralized monitoring, virtual consultant, and mixed. Centralized monitoring and virtual consultant use definitions defined in the Technology section of this article using full, real-time data review and intervention; mixed refers to a combination of both the Centralized Monitoring and Virtual Consultant Models.
eICU, electronic intensive care unit; ICU, intensive care unit; NICU, neonatal intensive care unit; PICU, pediatric intensive care unit; VHA, Veterans Health Administration.
Characteristics of Studies Addressing Compliance with Clinical Practice Guidelines of Tele-intensive Care Unit Systems
Provided for quasi-experimental studies only by guidelines of Harris et al. 34
Technology categories are as follows: centralized monitoring, virtual consultant, and mixed. Centralized monitoring and virtual consultant use definitions defined in the Technology section of this article using full, real-time data review and intervention; Mixed refers to a combination of both Centralized Monitoring and Virtual Consultant Models.
DVT, deep vein thrombosis; HOB, head of bed; ICU, intensive care unit; PUD, peptic ulcer disease.
Characteristics of Studies Addressing Intensive Care Unit (ICU) Clinical Outcomes (Mortality, Morbidity, Length of Stay) of Tele-ICU Systems
Provided for quasi-experimental studies only by guidelines of Harris et al. 34
Technology categories are as follows: centralized monitoring, virtual consultant, and mixed. Centralized monitoring and virtual consultant use definitions defined in the Technology section of this article using full, real-time data review and intervention; mixed refers to a combination of both Centralized Monitoring and Virtual Consultant Models.
eICU, electronic intensive care unit; LBW, low birth weight; LOS, length of stay; NICU, neonatal intensive care unit; RPT, remote presence technology; SICU, surgical intensive care unit.
Characteristics of Studies Addressing Feasibility of Tele-intensive Care Unit Systems
Provided for quasi-experimental studies only by guidelines of Harris et al. 34
Technology categories are as follows: centralized monitoring, virtual consultant, and mixed. Centralized monitoring and virtual consultant use definitions defined in the Technology section of this article using full, real-time data review and intervention; Mixed refers to a combination of both Centralized Monitoring and Virtual Consultant Models.
ICU, intensive care unit; ISDN, Integrated Services Digital Network; NICU, neonatal intensive care unit.
Characteristics of Studies Addressing Staff Perception, Satisfaction, and Workload of Tele-intensive Care Unit Systems
Provided for quasi-experimental studies only by guidelines of Harris et al. 34
Technology categories are as follows: centralized monitoring, virtual consultant, and mixed. Centralized monitoring and virtual consultant use definitions defined in the Technology section of this article using full, real-time data review and intervention; mixed refers to a combination of both Centralized Monitoring and Virtual Consultant Models.
eICU, electronic intensive care unit; ICU, intensive care unit; IT, information technology.
In studies addressing LOS and/or mortality outcomes, 18 (64%) involved centralized monitoring systems, 35 –52 8 (29%) used virtual consultant systems, 53 –60 and 2 (7%) used elements of both. 16,62 Of the centralized monitoring system studies, 15 used a pre–post design, 35 –40,42 –47,49 –51 one used posttest-only design, 52 one was a prospective clinical practice study, 41 and one was a triple-cohort time-series study, 48 whereas in the Virtual Consultant Model, two were pre–post prospective studies, 55,57 one used a control group without a pretest, 56 two used pre–post design, 58,60 and one was a systematic review (although only one study met inclusion criteria). 59 The two studies that involved both Centralized Monitoring and Virtual Consultant Models were systematic reviews. 16,62 In the Centralized Monitoring Model, 11 studies showed reduced mortality, 35,36,38,41,42,44,45,48 –50,52 whereas 4 studies showed no change in mortality. 37,43,46,47 Hospital and/or ICU LOS was reduced in eight studies, 39 –41,44,49 –52 unchanged in three studies, 43,46,47 and increased in one study. 37 Mean sample size of the centralized monitoring studies was 4,891 patients in an average of 6.8 ICUs. In the Virtual Consultant Model, mortality was reduced in two studies, 53,55 and hospital and/or ICU LOS was reduced in five studies. 54,56 –58,60 Mean sample size in the virtual consultant studies was 372 patients in an average of 1.3 ICU.
Regarding staff acceptance and workflow, there were 21 studies that used Centralized Monitoring Models, 47,63 –82 13 studies using Virtual Consultant Models, 56,83 –93,95 and 2 that used both. 62,94 The Centralized Monitoring Model showed 3 studies with pre–post studies, 47,63,66 whereas the 17 others were posttest studies. 64,65,67 –77,79 –82 In the Virtual Consultant Model, eight were posttest-only studies, 83,84,86,89,90,92,93,95 one was an embedded case study, 85 two were pre–post studies, 87,94 one was a cohort study, 88 and one used a control group with no pretest design. 56 Studies using both tele-ICU models included a pre–post controlled survey 94 and a systematic review. 62
Findings in the Centralized Monitoring Model generally fell into three categories: perceived tele-ICU impact on patient safety, communication between providers, and staff workflow. Many studies indicated increased perceptions of improved patient safety, 47,64 –67,69 with one study 69 mentioning likely error prevention. Perceived usefulness was a determinant in its use. 73 Communication-related concerns were mentioned frequently, with centralized monitoring cited to both enhance and detract from such interactions. Many raised the importance of pre-implementation teamwork between on-site and remote providers. 69,71 –76,79 –81 Effects on nursing workflow was mixed, as some perceived it to have been enhanced by improved teamwork, 66 nighttime support, 80 or other types of nursing practice, 64 whereas others felt it was hampered by interruptions, poor communication, or inaccurate information. 71,75,76,82 Information technology interoperability was cited as a problem in a few studies. 65,68 Virtual Consultant Model studies commented mostly on general satisfaction of the providers in tele-ICU use 88 –92,95 with perceived reductions in interhospital transfers 84,87 or reduced anxiety in critical care contexts. 84,85 Only one study commented on improved multidisciplinary system improvement. 93
Financial sustainability of tele-ICU systems was evaluated for centralized monitoring systems in six studies, 37,38,43,96 –98 whereas three studies 60,88a,99 looked at Virtual Consultant Models. In centralized monitoring systems, cost-effectiveness was unclear, 96 although enhanced documentation had putative benefits. 97 Virtual consultant cost-effectiveness was not examined.
Feasibility studies evaluated centralized monitoring systems in only one study (8%), which addressed the addition of telepharmacist involvement in daily sedative interruption protocols, 100 whereas 12 (92%) primarily posttest-only observational studies 84,86,88,101 –109 evaluated virtual consultant systems that focused on demonstrating general proof-of-concept benefits when tele-ICU technology was used as a surrogate for on-site microsurgery, 102 cardiology, 105 ophthalmology, 107 burn medicine, 108 and neonatal and pediatric intensive care 88,104,109 specialists.
Studies evaluating use of centralized monitoring tele-ICU in achieving clinical practice guidelines included two for centralized monitoring systems 110,111 and three for virtual consultant systems. 112 –114 Study design was either posttest-only 110,111,113 or pre–post 112,114 observations. Centralized monitoring studies described specific improvements in either blood glucose levels 110 or increased mean levels in sepsis bundle compliance, 111 whereas virtual consultant studies described improvements in adherence to ventilator-associated and venous thromboembolism prophylactic measures. 113,114
Discussion
In our systematic review of tele-ICU systems, we found a higher quantity and quality of studies addressing efficacy of the Centralized Monitoring and Virtual Consultant Models in terms of clinical outcomes, staff acceptance and workflow, and financial sustainability indicators. Studies of the Centralized Monitoring Model were almost twice as frequent as those addressing the Virtual Consultant Model. In particular, we found that investigations involving the Centralized Monitoring Model involved a more than 13-fold higher sample size of patients (and located in a larger number of ICUs) compared with studies with the Virtual Consultant Model, thereby boasting a statistical advantage when considering minimization of risk of bias.
Our findings are due to several reasons. First, hospitals that use the Centralized Monitoring Model often integrate powerful clinical information systems as part of their enterprise platform, thereby allowing for easier and effective data collection and analysis. In contrast, Virtual Consultant Models are often stand-alone platforms requiring manual input of data into existing hospital information technology systems. Second, the use of electronic medical record systems and clinical information systems has been part of a growing wave of efforts to improve the value of inpatient and outpatient healthcare through “meaningful use” of technology. As governmental pressure has mounted toward universal adoption of such systems by 2014, enthusiasm has blossomed in turn for centralized monitoring tele-ICU and other systems that can further utilize such datastreams and leverage them toward additional health care gains. Third, Virtual Consultant Models studied to date have included peer-to-peer-based interactions that are not easy scaled; as a result, most studies included only one ICU where patients were evaluated. In contrast, the remote multidisciplinary team essential to the centralized monitoring system infrastructure allows for easy expansion and enhanced economies of scale, as one control center “hub” often addresses the needs of multiple ICUs in multiple locations. 17 This expedites the enrollment of more patients in different locales and allows for use of statistical methods that can generate sufficient power for hypothesis testing. Fourth, wireless and other technology allowing adequate data transfer speeds for mobile telepresence (upon which the Virtual Consultant Model often rests) have been relatively recent and somewhat unreliable, whereas dedicated T1 connections upon which Centralized Monitoring Models depend have been robust for decades.
For all these reasons, study of centralized monitoring systems has been easier and appears more conceptually in line with ongoing and future efforts to find healthcare solutions through the analysis of “big data” (i.e., large and complex datasets that require novel data processing techniques) that is now gaining momentum.
Study designs that were utilized by researchers of tele-ICU systems were quite homogeneous between the two models: except for one study that was a quantitative randomized study, 54 all studies that met our inclusion criteria used a quasi-experimental study design using primarily a pre–post, cohort, or retrospective observational study design. We hope that future studies will use more prospective and randomized controlled trial designs to strengthen the conclusions made.
Qualitatively, our study findings are largely consistent with those of previous systematic reviews and meta-analyses, 16,62,96 which have been dominated by centralized monitoring systems. We too found that concerns about increased costs exist in the midst of increasingly promising trends for ICU mortality improvements. 45,49 We also found that staff satisfaction with centralized monitoring systems is generally favorable. However, in distinction to the findings of Young et al., 62 more recent studies have emphasized the disruptive nature of centralized monitoring tele-ICUs if organizational factors, perceived need, and proper channels of communication between remote and on-site providers are not optimized and continually configured. 63,71,76 Although a direct comparison is difficult given the small number of studies that met inclusion criteria and the variability of study design, our review revealed that both the Centralized Monitoring and Virtual Consultant Models demonstrate clear and similar benefits in clinical practice adherence efforts. This may become more significant as future studies are planned and executed.
Despite the existing lack of studies addressing Virtual Consultant Models, it is important to note that attention and research studies are quickly growing. We found that the majority (92%) of feasibility studies to date addressed the Virtual Consultant Model, 50% of which took place in the 3 years immediately prior to our review. Alongside with the breadth of medical specialties studying its use in these articles (from neonatal to adult medical and surgical specialties), this recent increase is noteworthy. In the near future, we expect and hope that the quality and quantity of studies evaluating Virtual Consultant Models will begin to match those of Centralized Monitoring Models to allow for a more equitable comparison of features, outcomes, and costs (for a current overview, see Table 6).
Comparison of Tele-intensive Care Unit Platforms
Note that all costs are based on 2013 pricing based on manufacturer's suggested retail price (MSRP), corporate documents, and personal communications with corporate representatives.
Cost does not include depreciation.
Tablet models are MSRP for 32GB flash memory, 802.11 WiFi capable only. RP-Xpress is a tablet-like device for telepresence use only.
All InTouchHealth units require a one-time $5,900 installation charge.
Prices are for standard, fully assembled, and integrated components on a cart on wheels (Codec, high-definition display, 10–12×camera, microphone, system speakers, rechargeable battery, cables) by the vendor listed with capability for up to four multipoint users' calling. Touch control panel, WiFi kit, and other options are sold separately at additional cost depending on vendor and contracted partners. Core Codec options exist for individual purchase at lower cost that can be integrated with existing equipment per client needs (additional software may need to be purchased).
Prices quoted include activation of (assembled) device on an existing secure data- or WiFi-enabled network. Prices exclude data service activation and data usage plans offered through commercial providers, as well as set up of Virtual Private Network, wireless network, and secure firewall network (if desired, some vendors [e.g., Cisco, Polycom] offer installation at $20,000–$50,000). Software license fees vary depending on number of total users as well as concurrent usage. Also, initial software fees are often included in service contracts. All InTouchHealth units require a one-time $5,900 wireless connectivity and access point assessment and installation per hospital.
For software and hardware upgrades.
Prices quoted exclude data usage or rental options (InTouchHealth).
Rental prices vary with contractual agreement but are roughly $2,500 per month (InTouchHealth).
Several vendors offer secure servers to allow legacy equipment multipoint control unit bridging and/or hosting of or other telepresence conferencing (e.g., Clearsea™ of Lifesize, VidyoGateway™ of Vidyo).
CIS, clinical information systems; CPT, current procedural terminology; ICU, intensive care unit; IT, information technology.
There are several limitations to our study. The relative dearth of data for the Virtual Consultant Model in comparison to that of the Centralized Monitoring Model coupled with the wide range of study objectives and design did not allow a meta-analysis and made cross-comparisons difficult. Thus, conclusions are discussed qualitatively and are based on study-specific findings. The wide variation of the types of ICU in which tele-ICU was implemented may have influenced how the tele-ICU model was used. For example, the Virtual Consultant Model may have been more accepted in relatively smaller specialty (e.g., neurologic) ICUs where intermittent evaluations were more appropriate than in busier, larger ICUs (e.g., mixed medical/surgical), where a larger multidisciplinary team intrinsic to Centralized Monitoring Models might be more apt. Apart from one study, 65 studies looking at hospital administration or patient and family satisfaction were not included. This would be important to include, given that administrators are closely involved with the choice and implementation of tele-ICU models. In an age where patient satisfaction scores are gaining in importance, patient and family satisfaction scores may vary between these two models whose benefits may not always be obvious.
Conclusions
In our systematic review, we found that studies to date that have investigated the effects of the Centralized Monitoring Model of tele-ICU care were more frequent and of higher sample size than those studying the Virtual Consultant Model. Future studies of the Virtual Consultant Model should incorporate enhanced study design, statistical methods, and outcomes studied in order to provide better comparisons with centralized monitoring systems.
Footnotes
Disclosure Statement
No competing financial interests exist. V.R.R. composed the manuscript text. L.M. performed search strategies and obtained articles for review. L.H. and V.R. performed data analysis. N.K. oversaw all aspects of the study, served as an arbitrator, and contributed to writing the manuscript.