
Abstract
Introduction
Projected physician shortages continue to add pressure on efforts to improve the quality, access, and costs of healthcare that comprise the “triple aim” of current U.S. healthcare improvement efforts. 1 An aging U.S. population has amplified concerns about projected shortages of medical staff dedicated to intensive care, including physician specialists, nurses, and clinical pharmacists. 2,3 Despite studies that demonstrate improved clinical outcomes 4,5 and costs 6 with direct involvement of critical care specialists, most hospitals do not employ recommended staffing models, 4,5,7,8 particularly in rural areas. 9
In order to address the need for intensive care specialist support, attention has turned to tele-intensive care unit (tele-ICU) (“telecritical care”) solutions that utilize telemedicine technology. Telemedicine involves the use of telecommunication technologies and enhanced data management systems to provide health information exchange across “geographic, time, social, and cultural barriers.” 10 Existing platforms of tele-ICU involve the Centralized Monitoring Model (e.g., Philips [Baltimore, MD] VISICU-eICU™ 11 ) 12 and the more recently seen Virtual Consultant Model. In this narrative review, we perform a qualitative side-by-side comparison of the two tele-ICU models evaluating technology, usage, and impact on clinical outcomes, financial considerations, and hospital workflow and satisfaction.
Definitions
Tele-ICU systems use fixed or portable hardware and equipment, centralized or decentralized staffing strategies, and open and closed communications architecture schema (Fig. 1). 13 Fixed tele-ICU systems use permanently attached, hard-wired, immobile hardware to transmit data between remote and originating sites, whereas portable or mobile systems allow varying degrees of independent movement of hardware devices involved in data transfer. Degrees of independence are differentiated as “autonomous” (completely independent and self-directed movement), “semiautonomous” (movement through remote manipulation [e.g., via joystick]), or “dependent” (movement via “surrogate hands” [i.e., a physical person moving the device]). Portable robot units (e.g., Vgo Communications, 14 Suitable Technologies, 15 InTouchHealth 16 ) use autonomous and/or semiautonomous movement. On the other hand, stand-alone mobile units that are attached to a cart or pole on wheels (e.g., Cisco, 17 Polycom, 18 Lifesize 19 ) require pushing and positioning the unit to the bedside by on-site personnel. Centralized and decentralized structures refer to the presence (centralized) or absence (decentralized) of a “hub” monitoring facility, often comprising a multidisciplinary team that handles information and delivers ultimate management plans to the “spoke” hospital(s) and/or ICU(s). Communications architecture is “open” if Internet connectivity provides multiple simultaneous peer-to-peer interactions without restriction, “closed” if single and dedicated point-to-point communications are provided (often used in centralized systems between “hub” facility and “spoke” hospital), or “hybrid” if it uses elements of both. 20
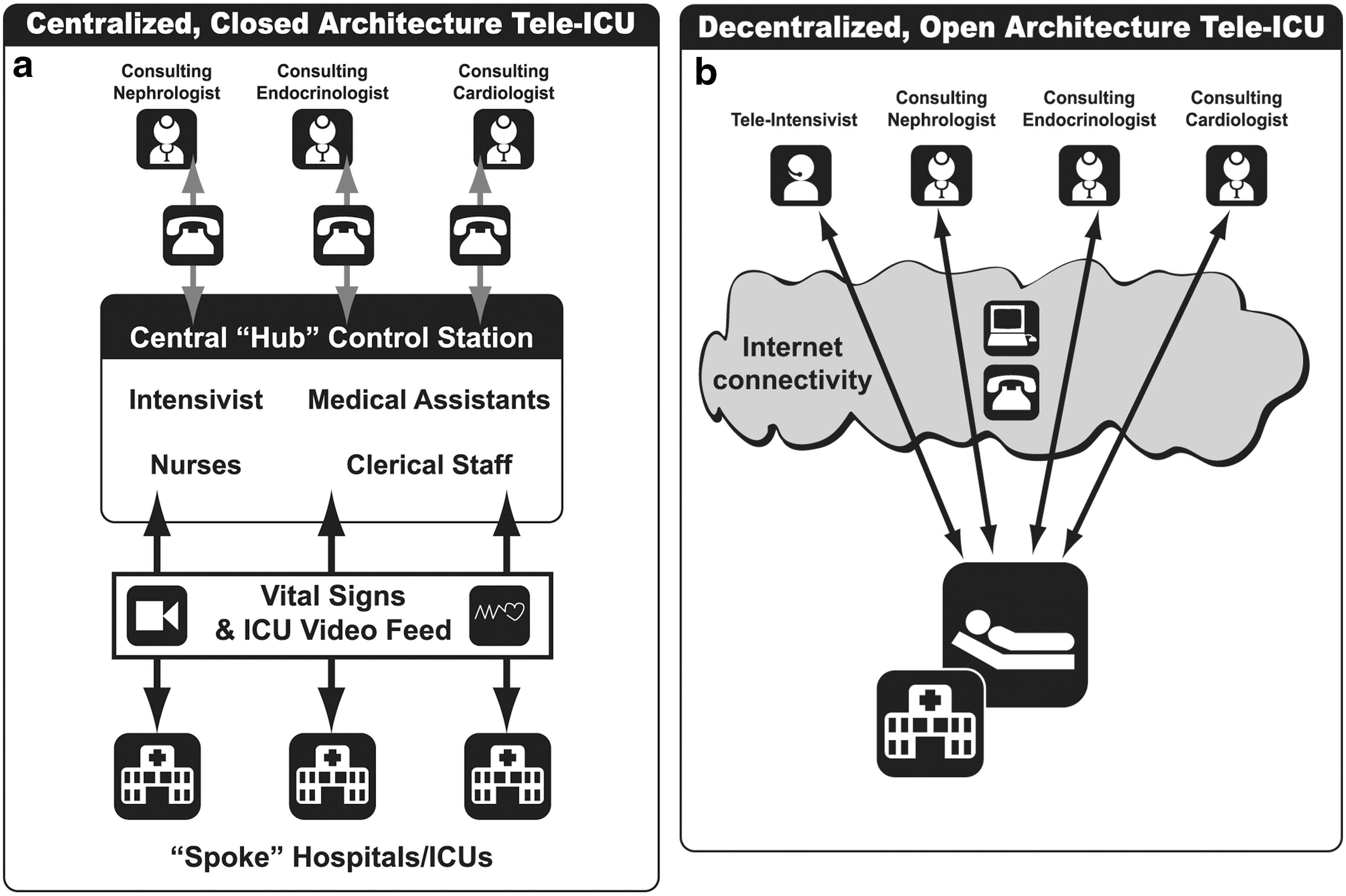
Tele-intensive care unit (ICU) structure.
Technology
The Centralized Monitoring Model (Fig. 1a) is most often a fixed, centralized, and closed-communications platform in tele-ICU care that collects and delivers primarily continuous (24/7) clinical data streams including vital signs and electronic medical record-based information as well as clinical information systems (CISs) that provide indicators and alerts for guideline compliance. 12,20,21 These components are variably implemented according to hospital needs, cost, information technology interoperability, and other concerns. 21 A dedicated T1 connection links the remote “spoke” site(s) to the “hub” monitoring facility where a team composed of nurses, administrative assistants, and intensivists handles the information. Although not universal or mandatory, a powerful feature is a CIS that is partially or fully integrated into the platform that the remote ICU team can utilize for (1) surveillance of physiologic perturbations (e.g., blood pressure changes), including trend analysis, (2) vigilance regarding deviation from clinical practice standards (e.g., protocol adherence) based on diagnosis, acuity, and treatment plan analysis, and (3) primary data collection for case mix analysis, risk-adjusted severity assessments (e.g., APACHE or SAPS scores) for proper patient triage, and outcomes analyses. Integrated CIS software allows for fully automated data input, without which manual input is required. Although interoperability concerns may limit complete CIS integration (and hence full functionality), complete absence of CIS components in centralized monitoring systems is uncommon. Interaction with on-site providers is at the discretion of the remote team, depending on assessed clinical need for on-site intervention.
Although there are several commercial vendors of centralized monitoring systems, incluing Philips VISICU-eICU, 11 Cerner, 22 and iMDSoft, 23 individual health systems (such as iCare of Banner Health 24 or the Veterans Health Administration hospital network) have created similar centralized “hub-and-spoke” monitoring platforms internally.
The Virtual Consultant Model, on the other hand, is most often a portable, decentralized, and open-communications architecture platform, in which a remote provider attends the patient through a telepresence modality (e.g., a robot, pole- or cart-based videoconferencing hardware, or tablet with two-way video and audio connection). The remote provider takes advantage of the technology to intermittently interact with staff and patients (and their families) to provide clinical evaluation and treatment in the manner an in-person consultant but without access to continuous data streams or integrated CISs that are characteristic of most centralized monitoring systems. There are several vendors of portable robot units, 14 –16 cart-based units, 17 –19 and hand-held devices, including tablets like the Apple iPad®, 25 Samsung Galaxy Tab®, 26 Google Nexus, 27 and Asus Transformer Pad. 28 Some vendors (e.g., Vidyo 29 ) offer primarily software allowing hosting of secure multiuser telepresence sessions with legacy equipment. Unlike centralized monitoring systems, which often wield extensively integrated data streams and CISs, virtual consultant systems do not incorporate CISs per se and provide a more “fly on the wall” bedside experience for the remote provider in which patient-centered data such as case mix and risk-adjusted severity scores must be accessed separately (e.g., remote access portals to electronic medical records, imaging software, CIS, etc.). To date, virtual consultant technology is primarily focused on recreating the experience of being at the patient's bedside for a provider who is in a physically remote location.
The technical specifications of the audio and video feed are similar regardless of the tele-ICU platform. Common to most is two-way digital video and audio with standard (640×480 pixels) or high-definition (1280×720 or 1920×1080 pixels) resolution transmitted between the remote provider and patient using CODEC (“COder-DECoder”) data-compression software (the version most currently used is H.264/MPEG-4), which allows video images to be compressed, sent over the Internet at speeds of at least several megabytes per second, and then decompressed at the monitoring facility. 30 Work is underway to evaluate uncompressed video (e.g., DV transport system, iHDTV, UltraGrid, and HD CXP), which provides higher image quality. Connectivity on both provider and patient ends needs to support such data transfer speeds, which is more of a concern in the case of virtual consultant systems, which commonly use wireless (WiFi and/or 4G) technology. Device mobility complicates maintenance of signal strength, unlike the dedicated T1 connection common to centralized monitoring systems. Like other means of remote patient data access, both virtual consultant and centralized monitoring systems must ensure security in the form of suitable access ports in the hospital firewall and password access for encrypted network entry and maintain compliance with the Health Insurance Portability and Accountability Act and other privacy measures.
Patient Examination
Both Centralized Monitoring and Virtual Consultant Models provide a medium by which remote providers can examine patients. The primary elements of the physical examination—inspection, auscultation, palpation, and percussion—are addressed in order.
Inspection
This is provided by high-definition video and zoom (often 10–12x equivalent), which are similar in both the Centralized Monitoring and Virtual Consultant Models. Such magnification allows visualization to the detail of a pupillary reflex. Screens are either static 11 or offer dual planar (vertical and horizontal) swiveling. 16 –19 Easier mobility and free-standing device screens provide easier independent positioning and better anthropomorphic “presence,” further enhanced by a screen showing the provider's face moving in real time (as opposed to screens fixed to walls). The advantages of higher-resolution sound and video provided with systems with secure, fixed connections are weighed against the benefits of portability because signal strength and consistency of Internet/wireless connectivity continue to be a challenge for portable systems.
Auscultation
In both tele-ICU models, stethoscope quality is currently fair to poor. 31 An internal device transmits sound captured from a stethoscope connected electronically to the unit, conveying audio information in real time to the remote provider, but buffer times (often 1.5–2.0 s) are variable as they depend on connectivity and hardware specifications. One vendor 32 offers a stand-alone stethoscope (the Littmann TeleSteth®) with real-time auscultation ability via Bluetooth® 2.0 (Bluetooth SIG, Kirkland, WA) and Internet-based software transmission at Food and Drug Administration–approved decibel quality, which can be used regardless of tele-ICU platform.
Palpation/percussion
In both the Centralized Monitoring and Virtual Consultant Models, the availability of direct tactile information is currently completely dependent on the on-site “surrogate hands,” 20 usually provided by a bedside nurse. The remote provider must coach the nurse to position, palpate, and/or percuss the organ in question. Because patience, operator skill, and education are required, this is often the most time-consuming part of the examination.
Outcomes in Centralized Monitoring and Virtual Consultant Tele-ICU Models
Both Centralized Monitoring and Virtual Consultant Models provide tele-intensivist care of remotely located patients, with notable distinctions (Table 1). We performed a qualitative comparison of the data from our systematic review that involved examination of 1,468 publications addressing the use and effectiveness of centralized monitoring and virtual consultant tele-ICU systems. 33 In that study, 46 documents involved clinical outcomes (guideline compliance, 5; mortality and length of stay, 28; feasibility, 13), 9 documents addressed financial sustainability, and 36 addressed ICU staff workflow and acceptance. We proffer these conclusions to institutions looking to incorporate tele-ICU technology that might best suit their particular ICU needs.
Comparison of Tele-intensive Care Unit Platforms
Note that all costs are based on 2013 pricing based on manufacturer's suggested retail price (MSRP), corporate documents, and personal communications with corporate representatives.
Cost does not include depreciation.
Tablet models are MSRP for 32GB flash memory, 802.11 WiFi capable only. RP-Xpress is a tablet-like device for telepresence use only.
All InTouchHealth units require a one-time $5,900 installation charge.
Prices are for standard, fully assembled, and integrated components on a cart on wheels (Codec, high-definition display, 10–12x camera, microphone, system speakers, rechargeable battery, cables) by the vendor listed with calling capability for up to four multipoint users. Touch control panel, WiFi kit, and other options are sold separately at additional cost depending on vendor and contracted partners. Core Codec options exist for individual purchase at lower cost that can be integrated with existing equipment per client needs (additional software may need to be purchased).
Prices quoted include activation of (assembled) device on an existing secure data- or WiFi-enabled network. Prices exclude data service activation and data usage plans offered through commercial providers, as well as set up of virtual private network, wireless network, and secure firewall network (if desired, some vendors [e.g. Cisco, Polycom] offer installation at $20,000–$50,000). Software license fees vary depending on number of total users as well as concurrent usage. Also, initial software fees are often included in service contracts. All InTouchHealth units require a one-time $5,900 wireless connectivity and access point assessment and installation per hospital.
For software and hardware upgrades.
Prices quoted exclude data usage or rental options (InTouchHealth).
Rental prices vary with contractual agreement but are roughly $2,500 per month (InTouchHealth).
Several vendors offer secure servers to allow legacy equipment multipoint control unit bridging and/or hosting of or other telepresence conferencing (e.g., Clearsea™ of Lifesize, VidyoGateway™ of Vidyo).
CIS, clinical information systems; CPT, current procedural terminology; ICU, intensive care unit; IT, information technology.
Clinical Outcomes
One of the main advantages of the Centralized Monitoring Model appears to be the offering of a dedicated, robust, and integrated clinical information ecosystem for ICU patients. Harnessing the power inherent to the combination of 24/7 continuous and automated data streams, electronic medical records (with computerized order entry), data collection and analysis software, and a multidisciplinary clinical team, centralized monitoring tele-ICU systems promise safe and effective ICU care (both actual and preemptive) that seems intuitive. Individual cases can be parsed according to diagnosis, acuity, and treatment algorithm and analyzed for compliance and accuracy. Furthermore, the software can assess risk-adjusted severity to ensure expedient and proper patient triage. Automated alerts for physiologic abnormalities are fielded immediately by nurses. Sepsis, 34 glucose control, 35 and other protocol deviations are corrected within seconds of automated notifications, and concerning data trends can be reviewed at the click of a button and discussed with an ICU specialist immediately. Indeed, staff perceptions of improved patient safety, including error reductions, were seen in a recent systematic review. 33 As a result, new goals of “patient-centered” ICU care can be achieved using data acquired before and during a patient's ICU stay to triage patients appropriately, analyze case mixes, and construct patient-specific coordinated care plans. Parameters include APACHE and/or SAPS severity scores, 36 preceding medical history including response to past interventions, and population-based metrics based on existing comorbidities.
Full functionality of integrated CISs and automated data population is required for full benefits to be realized; partial integration due to interoperability concerns with legacy information technology systems and/or manual data entry requirements substantially limits the clinical potential of centralized monitoring systems. Although hospitals that use centralized monitoring systems are not obligated to use all components of these CISs in the tele-ICU workflow, most attempt to do so, with good reason.
Nevertheless, we found that the effect of centralized monitoring on macroscopic indicators of clinical outcomes of mortality, morbidity, and length of stay is generally favorable but not definitively so. 33 Several early studies 37,38 indicated considerable benefits, although limitations of small sample size, single academic hospital setting, and possible clinician bias questioned the generalizability of results.
More recent studies have shown improved mortality 39 –48,50 and lengths of stay 43,44,47 –49,51 –53 in Centralized Monitoring Models of tele-ICU; however, most are quasi-experimental and single-center investigations, with marked variations in study design. Thus, doubts exist over whether the benefits were due to the actions of the technology itself or to simply better care provided by bedside clinicians. 54 Studies had conflicting results: some showed no change in mortality, 55 –57 even in a variety of hospital settings (teaching, urban, and community), 57 whereas others showed no change 56,58 or even increased length of stay. 55 The meta-analysis of Wilcox et al. 59 showed a mortality improvement with use disparate tele-ICU systems, but the low numbers of studies included in the study unfortunately did not yield sufficient power to perform subgroup analysis to identify a true treatment effect between “active” (centralized monitoring) and “passive” (virtual consultant) usage or a dose–response effect of such technology. We support the conclusion that the Centralized Monitoring Model reveals mixed effects on clinical outcomes, although there may be benefits to its use in specific situations, such as outcomes in a rural health setting, 48 in an academic surgical ICU, 46 or in sicker patients. 60
Advantages have been seen with centralized monitoring use in ICU protocol compliance. 34,35,61 –63 Thus, we see the greatest advantages and possible recommendations for the Centralized Monitoring tele-ICU Model in rural hospitals and/or medical centers aiming to improve protocol adherence or outcomes in specific patient populations where other measures have not been successful, using real-time surveillance of aberrations through extensive, around-the-clock monitoring. Furthermore, those hospital systems with existing or planned use of CIS for disease (e.g., sepsis) and severity classifications (e.g., APACHE) would likely benefit from an integrated centralized monitoring tele-ICU platform that can draw on such data streams for effective ICU patient care and even proper level of care designations that consequently enhance resource utilization efforts. There is much power that is afforded by centralized monitoring systems in the realm of research studies, given larger sample sizes and diverse patient populations that can be managed from a centrally located remote location. 36 This may be of particular interest to hospitals that are part of risk-sharing organizations (e.g., accountable care organizations) or connected to academic centers where researchers can collaborate with clinicians for population-based approaches to healthcare that are rapidly gaining momentum.
In contrast, efficacy studies of the Virtual Consultant Model in improving clinical outcomes are almost completely lacking. As in centralized monitoring systems, adherence to best practices is seen in some virtual consultant systems. 62 –64 Vespa 64 described improved lengths of stay with Virtual Consultant Model interventions in an academic neurointensive care unit. A major disadvantage is the relative difficulty in utilizing the power of CIS in patient evaluation and treatment that most centralized monitoring systems boast. Rather, the Virtual Consultant Model does not incorporate CIS as part of its decentralized platform and requires separate access to CIS if patient-centered information is desired (e.g., case mix, risk-adjusted severity scores). The Virtual Consultant Model primarily provides a stand-alone “fly on the wall”-type experience that recreates the experience of standing at the patient's bedside. However, as integrated data streams are unavailable, the individual remote provider assumes almost all of the risk of overall patient care provision. Knowing what we do about the complexity of ICU care and increasing need for clinical provider and data coordination for best practice-based outcomes and resource utilization, this raises questions as to whether satisfying the immediate need for an ICU specialist ultimately benefits the overall care of the patient from the systems-based point of view. Thus, further study is needed before any efficacy assessments or recommendations can be made.
Costs and Financial Sustainability
Nine studies 55,56,60,65 –70 addressed cost considerations with the use of both centralized monitoring and virtual consultant types of tele-ICU systems. 33 Study quality varied considerably given inconsistent methods of cost calculations and estimates, although most reported cost savings from reduced patient transfers (up to 58% 70 ), nearing $10,000 saved per patient not transferred, 67,72 and up to $279,000 of increased revenue gained per year. 69 Weaknesses of centralized monitoring systems lie in its high cost to install and maintain. 65,67 Consisting of fixed, comprehensive overlays, the centralized monitoring solution is often permanent, requiring physician and nurse staffing at an additional annual $10,000–$20,000 per ICU bed covered. 67 A recent systematic review of tele-ICU costs 65 examined eight studies at centers using centralized monitoring systems and demonstrated combined cost estimates for implementation and first-year operation of approximately $50,000–$123,000 per ICU bed, depending on depreciation methods used; based on the available data, the authors were unable to calculate cost savings associated with use of centralized monitoring. Hospitals must make ad hoc arrangements for financial reimbursement for centralized monitoring services, as they are not currently supported by third-party payers. 65,67 Indeed, hospitals adopting centralized monitoring systems do not expect to realize cost savings. 67 Considering these findings, it seems most appropriate that hospitals that do not require transparent and immediate financial returns on investment may find centralized monitoring systems a reasonable platform to utilize.
There were no specific studies of costs associated with the Virtual Consultant Model; furthermore, any cost-effectiveness evaluation is premature given minimal data documenting clinical efficacy. Thus, no conclusions or comparisons with the Centralized Monitoring Model can be made in this regard until further studies are done.
Our review of corporate documents and Internet sites suggests that absolute values of initial and maintenance costs of Virtual Consultant Models are low. If hardware is purchased and owned by the institution, prices range from approximately $500 for tablets to $6,000–$20,000 for semiautonomous mobile robot unit 14,15 to approximately $20,000–$65,000 for stand-alone, dependent, cart-based unit with assembled components 17 –19 to $141,000 for a completely autonomous mobile robot unit. 16 Although rental of hardware is not currently available for tablets, it is possible for some mobile units, 16 for around $3,000 per month. Unless hardware is proprietary, 16,17 service contracts for hardware components are through contracted vendor partners, with costs approximately $1,000 per unit per year. Software license costs vary by the number of users but uncommonly exceed $1,000 per user per year when proprietary hardware is used 16 –18 ; session hosting is available at $100 per month per virtual conference room and $50 per month per user. 29 Data packages must be purchased for Internet connectivity services. With one active mobile unit and one backup unit available for every 10–15 ICU beds (the average size of an ICU in the United States), the total cost is less than $70,000 in most cases (excluding maintenance and/or replacement costs). Other speculative advantages to hospitals concerned with returns of investment include the following: possibility of a “trial period,” after which the unit can be removed without major disruption; portability, allowing other specialty services (e.g., pharmacy) to utilize the mobile unit during “downtime,” thereby enhancing overall utilization; and billing reimbursement, because growing numbers of U.S. states allow Current Procedural Terminology (CPT) 73 reimbursement of remotely provided clinical services, under 99253–99255 or 99221–99223 for initial consultative evaluations and 99231–99233 for subsequent care codes, with the –GT telemedicine modifier.
For these reasons, we suggest that the Virtual Consultant Model may be attractive to rural or other hospitals concerned with absolute costs, lower patient volumes, relatively infrequent need for specialist access, and a need for short-term cost recovery through billing reimbursement. Hospitals in which enterprise information technology solutions or an extensive CIS are not possible may see benefit from the Virtual Consultant Model. Furthermore, putative return on investment assessments can occur relatively quickly given easy implementation and removal.
Staff Workflow and Acceptance
Our review 33 revealed 36 studies 52,67,74 –107 addressing tele-ICU impact on workload and staff acceptance. Although overall nursing and staff satisfaction 52,76,81,88,93,95,96,99,100,102 –104,106,107 and perceived teamwork, quality of care, and patient safety 67,75 –77,79,80,82,87,88,90,91,93,98 –100,104,106 were subjectively enhanced by use of centralized monitoring or virtual consultant tele-ICU technology, we could not find any study that showed corroboration with objective findings.
Regarding the Centralized Monitoring Model, conclusions are generally favorable, although there are several caveats to note. Like other enterprise solutions (e.g., Epic 108 and Toyota Production System 109 ), the centralized monitoring platform requires extensive and multidisciplinary strategies before, during, and after initial implementation to ensure optimal adoption and efficacy. 7,84,86 Young et al. 107 found positive staff acceptance of disparate tele-ICU systems but were hampered by methodologic shortcomings based on the quality and heterogeneity of the data that precluded a meta-analysis, similar to our study. Reduced interoperability of the Centralized Monitoring Model with hospital legacy systems impacts functionality, as benefits are realized only when the full platform is applied. 67 The presence of supportive and experienced on-site staff 82 –84 and a collegial relationship with remote providers 79,89,91 are essential to local staff enthusiasm to use the centralized monitoring system. The relatively impersonal (centralized monitoring coverage panels tend to be extensive), reactive, and imperfect 67,85 nature of centralized monitoring interventions has led to friction and skepticism toward recommendations 67,78,110,111 because the physicians are often unknown to local staff, and interactions are frequently faceless. 89 Althugh some on-site staff champion the “oversight, redundancy, and feedback” 67 that centralized monitoring offers, others dislike the anonymous “Big Brother” aspect 67,78,107 and have perceptions of increased workload, 78,84 “overreaction” to minor physiologic perturbation, 67 and “alert fatigue.” 112 Concerns about disruptions of workflow have been raised in recent years. 81,85,86
As a result, up to 66% of primary care physicians have limited centralized monitoring involvement in ICU in some studies, 56,57 raising questions about the role of centralized monitoring technology in actual outcome improvements. 54 We suggest that larger academic centers accustomed to enterprise solution planning and implementation with experienced staff may find centralized monitoring systems more effective, whereas community hospitals, where personal relationships are particularly important, may not.
Regarding the Virtual Consultant Model, data are again too sparse to make any definitive conclusions. Some studies showed improved provider perception of care 100 and reduced staff burnout. 113 We speculate that this may be due to anthropomorphic features of the telepresence unit itself, the ability to examine a patient directly and ad hoc, and easy integration, given minimal interference with hospital legacy systems with possible bridging of connections between different legacy systems and products. 18,29 Further study is greatly needed.
Limitations
There are several limitations to our review. First, the relative lack of data in the Virtual Consultant Model considerably affected our ability to make proper comparisons with the Centralized Monitoring Model. 33 Wilcox et al. 59 experienced similar difficulties in their systematic review and meta-analysis of tele-ICU outcomes when attempting subgroup analysis of tele-ICU model platforms. Furthermore, we did not include studies of centralized monitoring systems in which continuous data streams and at least partial integration of automated CISs were not used, given that their incorporation is the most common practice. Future studies should focus on identifying the incremental advantage of each of these data components towards the overall effectiveness of the centralized monitoring system. Second, the wide variation in the objectives and study design of the reviewed studies, many of which were quasi-experimental or observational, did not allow for objective analysis such as a meta-analysis. Third, experimental studies themselves were of varying quality, rigor, and methodology lending to difficulties in analysis, as was experienced by Young et al. 107
Future Directions and Conclusions
Although the gold standard is still a direct, in-person presence between physician and patient, tele-ICU solutions continue to fill an evolving void. Many areas of investigation still need to be addressed. 114 Regarding workflow considerations, how many patients can be seen by a particular virtual consultant tele-intensivist? Is a nighttime tele-intensivist sufficient in the presence of a low-intensity, daytime, in-person staffing model? 115 Regarding training challenges, how will the use of tele-ICU affect medical education and training needs and skills in general? What specific training is needed for tele-intensivists? Regarding technology requirements, will the optimal interface among provider, patient, and staff be mobile unit-based, tablet-based, or other? To what extent does autonomous portability matter to provider, patients, and staff? How important is CIS integration to either platform in achieving full benefits?
These and other areas need to be addressed by the critical care research community. Investigations of clinical efficacy of both tele-ICU models, particularly the Virtual Consultant Model, are still needed before cost-effectiveness can even be considered. We urge that ongoing and future investigators of tele-ICU systems, particularly the Virtual Consultant Model, focus on executing randomized controlled trials with sufficient methodologic quality and rigor to provide substantive conclusions and comparisons between and within groups. Such data will prove invaluable in making judicious decisions regarding tele-ICU systems to provide further advances towards “safe, effective, patient-centered, timely, efficient, and equitable” 116 healthcare.
Footnotes
Disclosure Statement
No competing financial interests exist. V.R.R. composed the manuscript text. N.K. oversaw all aspects of the study, served as an arbitrator, and contributed to writing the manuscript.