
Abstract
Background
The Republic of Cabo Verde (previously known as Cape Verde, but changed to Cabo Verde, per a United Nations directive on October 24, 2013) is an island country that consists of an archipelago of 10 main islands and several smaller islands and islets. Located 570 km off the coast of Western Africa, off Senegal, culturally contiguous with West African sub-Saharan countries, latitude 16 N, the country covers an area of 4,033 km2 and is home to 531,046 inhabitants (estimated as of July 2013). 1 Of the 10 main islands, only 9 are inhabited. The country has a service-oriented economy, with a gross domestic product (GDP), or purchasing power parity, per capita of $4,200 in U.S. dollars (estimated as of 2012). 1
Health indicators are relatively positive in the Republic of Cabo Verde, compared with other countries in sub-Saharan Africa. In 2011, 4.8% of its GDP was spent on health. The infant mortality rate is 23.0 deaths per 1,000 live births, whereas the maternal mortality rate is 48.4 deaths per 100,000 live births. In terms of health resources, the country has 282 physicians, 576 nurses, and 1,081 hospital beds. 2 The distribution of the healthcare force among the nine inhabited islands manifests large differences: the island of São Vicente has the highest ratio per person of both physicians and nurses. In fact, its ratio is 5.6 times higher than on the island of Boa Vista (in relation to physicians) and 2.9 times higher than on the island of Sal (in relation to nurses) (Table 1).
Human Resources in the Republic of Cabo Verde Healthcare Sector
Additionally, the large geographic distances between the nine inhabited islands and the country's lack of specialist physicians make the citizens potentially very vulnerable with regard to needed healthcare services. More complex procedures, such as neurosurgery and cardiac surgery, are done abroad. The Republic of Cabo Verde does not have a medical school, so all of its physicians are graduates of foreign medical schools (in Portugal, Brazil, Russia, China, Cuba, and other countries). These physicians are well educated and trained, and the provision of these specialists combats the problems created by the large geographic distances. Furthermore, the country is prosperous and politically very stable, with a well-funded Ministry of Health (MOH) that provides most healthcare services for its citizens, although some private hospitals and clinics do exist, and the country has relatively good health statistics. Nonetheless, providing medical care to the country's population is challenging.
Situated between Africa and the Americas, the Republic of Cabo Verde starkly illustrates the huge disparities in healthcare and other resources on opposite sides of the Atlantic Ocean. Although the two regions are similar in population, the Americas have 37% of the world's healthcare workforce and spend over 50% of the world's healthcare resources; the corresponding percentages for Africa are 3% and less than 1%. 3
Telemedicine and e-health have been suggested as one solution for closing the health disparity gap between the developed world and the developing world. 4,5 Yet evidence is lacking from current successful programs in the developing world and, in particular, from sub-Saharan Africa. 6
In the mid-1990s, one research group speculated that joint telemedicine networks between European and African countries, featuring remote diagnosis and teleconsultations, could make a real difference in Africa. 7 The later initiatives in the context of the Réseau Afrique Francophone de Télémédecine (RAFT Project) came to a different conclusion: big gaps in resources between European and African countries could limit the importance of the so-called “North-to-South collaboration.” Instead, RAFT Project workers focused on promoting the role of regional networks (i.e., on “South-to-South” initiatives). 8,9 Other published evidence from several RAFT initiatives highlighted the contribution of e-health in distance education 10 and in store-and-forward telemedicine. 11 One difference between Cabo Verde and other countries involved in RAFT is that Cabo Verde funds the continuing medical education (CME) for its doctors, whereas the other countries do not.
More recently, Mars 11 (who has written extensively about telemedicine and e-health in Africa) concluded that—with the exception of tele-education—there are few sustainable telemedicine services in Africa. In a previous review article, Mars 12 had also concluded that tele-education in Africa appears to be better received and to be more successful than clinical telemedicine. Wootton 13 stressed that the cost-effectiveness of clinical telemedicine for developing countries remains to be determined; moreover, he called for clinical trials to determine the cost-effectiveness of clinical telemedicine, in order to compare it with other interventions whose cost-effectiveness has already been proven. A favorable cost–benefit ratio for telemedicine programs in developing countries, in particular in terms of CME, has been previously demonstrated. 14
The use of telemedicine in Cabo Verde is not new, however. Since 2009, children with cardiac anomalies are examined by a local cardiologist, and the cardiac ultrasound images are sent to cardiac surgeons in Portugal, after which these children are evacuated for definitive surgery. This has proven to be an important improvement in the care of these children, who otherwise would not have been able to get care in Cabo Verde, as they do not have pediatric cardiac surgeons. 15 What is new in telemedicine in Cabo Verde is the establishment of a nationwide integrated telemedicine program.
The primary objective of this study was to present the preliminary results of our efforts in building the Integrated Telemedicine and e-Health Program for Cabo Verde (ITeHP-CV), with an emphasis on initial utilization. The ITeHP-CV is being implemented by the U.S.-based International Virtual e-Hospital Foundation (IVeH), a nongovernmental organization with funding from the Government of Slovenia. 16 Our secondary objective was to demonstrate that the Republic of Cabo Verde seems to be upending the prevailing African telemedicine paradigm with a program that puts more importance on clinical teleconsultations (not just virtual education and electronic knowledge sharing) and that upholds sustainability as a top policy priority.
Materials and Methods
This is a prospective study of data collected while we worked to establish a fully functional, integrated regional telemedicine network and virtual education network in the Republic of Cabo Verde. We used the IVeH strategic approach known as “initiate–build–operate–transfer” (IBOT) 5 over a 26-month period (November 2011–December 2013). The IBOT approach consists of four phases (Fig. 1). The initial phase in the IBOT strategy is structured to provide the nation's leadership with a broader understanding of telemedicine and the necessity of establishing such a program. It starts with an assessment of the utility of instituting a telemedicine program based on the detailed survey whose goal is to understand the needs and the political will of the leadership to establish the program.

The process and time relationship of development of the “initiate–build–operate–transfer” approach. Modified from Latifi. 4
The second phase, or the building phase, is based on the initial technical assessment and on the goals of the project. The four main steps of this phase are as follows: build the network; develop the main physical telemedicine center with the necessary space for an electronic auditorium, training areas, servers, administrative offices, and, ideally, additional resource or educational rooms; establish the electronic medical library; and produce training and educational opportunities so that local personnel can independently run the program and effectively offer clinical and educational services in the future.
The third, or operating phase, is likely the most challenging phase of the IBOT strategy. As part of the capacity-building phase, this part of the process focuses on creating telemedicine experts, ambassadors, and champions.
Finally, the fourth, or transfer phase, ideally, is the final phase of the IBOT strategy and signifies the completion of telemedicine program that is now turned over to the local public institution or the government. The MOH of that country becomes the official “owner” of the telemedicine center and equipment. Institutionalization of telemedicine is vital for sustainability; it must become an integral, long-term part of standard protocols and procedures.
All educational programs were conducted in or translated into the Portuguese language. We describe herein the five main pillars of this process that have been implemented: (1) capacity building; (2) network development and deployment of equipment; (3) implementation of clinical telemedicine; (4) implementation of activities related to CME, delivered from within the country and from abroad; and (5) establishment and use of the electronic virtual library.
Capacity Building
The human resources behind the ITeHP-CV were created through an intensive capacity identification and capacity building process. We organized the first National Intensive Conference on Telemedicine and e-Health in the capital city of Praia, on the island of Santiago, followed by regional replicas in three more regional sites.
In parallel, our project team and our local partners conducted the Telemedicine and e-Health Leadership (TeHL) selection process. We selected one doctor and one nurse from each of the eight referring centers, as well as nine physicians of different specialties from the two consulting hospitals.
The participants were divided into two teams and invited to a 1-week international TeHL development conference in Albania and Kosova. During that conference, five clinical telemedicine projects were elaborated on, in the areas of teledermatology, telecardiology, teletrauma, teleradiology, and telegynecology. The TeHL teams have continued for the Republic of Cabo Verde, with ad hoc training and coaching events conducted either in place or through distance education. During installation of the equipment on each site, the local teams were also instructed in the maintenance and troubleshooting of equipment.
In addition to the selection of the TeHL teams, the MOH of Cabo Verde (MOH-CV) established a temporary structure, named the Telemedicine Steering Committee, to advise on and guide telemedicine activities.
Network Development and Deployment of Equipment
We selected equipment based on the identified priorities and available budgets. The telemedicine carts (GlobalMed, Phoenix, AZ) and videoconferencing equipment (Polycom, San Jose, CA) were deployed in two phases: 98 physicians and nurses attended the initial intensive technical training seminars in December 2012; an additional 38 physicians and nurses attended training in June 2013.
Implementation of Clinical Telemedicine
The clinical telemedicine activities are made up of clinical protocols, development of protocols, including development of software by IVeH specifically for the project, scheduling, and coordination of clinical activities. A network of telemedicine carts, which combine videoconferencing capability with several integrated peripherals to support the clinical activity of several telemedicine disciplines, enables these activities. Apart from the video camera, the telemedicine carts are equipped with an additional high-definition camera that can be used for teledermatology and teledentistry, an e-stethoscope, an e-electrocardiograph, an abdominal ultrasound probe, and a vital signs monitor (blood pressure, heart rate, body temperature, and oxygen saturation). The local technical experts, physicians, and nurses who attend the biweekly technical checks are fully capable of exploring the capabilities of the carts.
Implementation of Activities Related to CME
The CME component is supported by Polycom-enabled, multipoint control unit technology that enables the simultaneous connection of all 10 telemedicine centers with each other, as well as with interoperable centers abroad, for the purpose of organizing virtual training events. IVeH has promoted the creation of a liaison among the ITeHP-CV, the Kosova Telemedicine Program, and the Integrated Telemedicine and e-Health Program in Albania as three fully interoperable programs in terms of the CME component.
Establishment and Use of The Electronic Virtual Library
The virtual e-library consists of a network of computers and subscription to the World Health Organization database known as Health InterNetwork Access to Research Initiative (HINARI). The HINARI Programme established by World Health Organization, together with major publishers, enables low- and middle-income countries to gain access to one of the world's largest collections of biomedical and health literature. More than 13,000 journals (in 30 different languages), 28,000 books, and 70 other information resources are now available to health institutions to more than 100 countries, areas, and territories.
Results
During our study period (November 2011–December 2013), we conducted a comprehensive technical and medical assessment of the country's needs and then established 10 fully functional telemedicine centers in all nine inhabited islands of the Republic of Cabo Verde. Our project team was made up of recognized international telemedicine experts working in collaboration with our local partners. The results of the five main pillars described in Materials and Methods are detailed below.
Capacity Building
The ITeHP-CV in the nine inhabited islands consists of 10 telemedicine centers: two are consulting hospitals, and eight are referring centers. The two consulting hospitals provide tertiary care to the windward islands (Santo Antao, São Vicente, São Nicolau, Sal, and Boa Vista) and the leeward islands (Brava, Fogo, Santiago, and Maio). Of the eight referring centers, four are located in hospital structures, and four are in primary healthcare settings (Fig. 2).
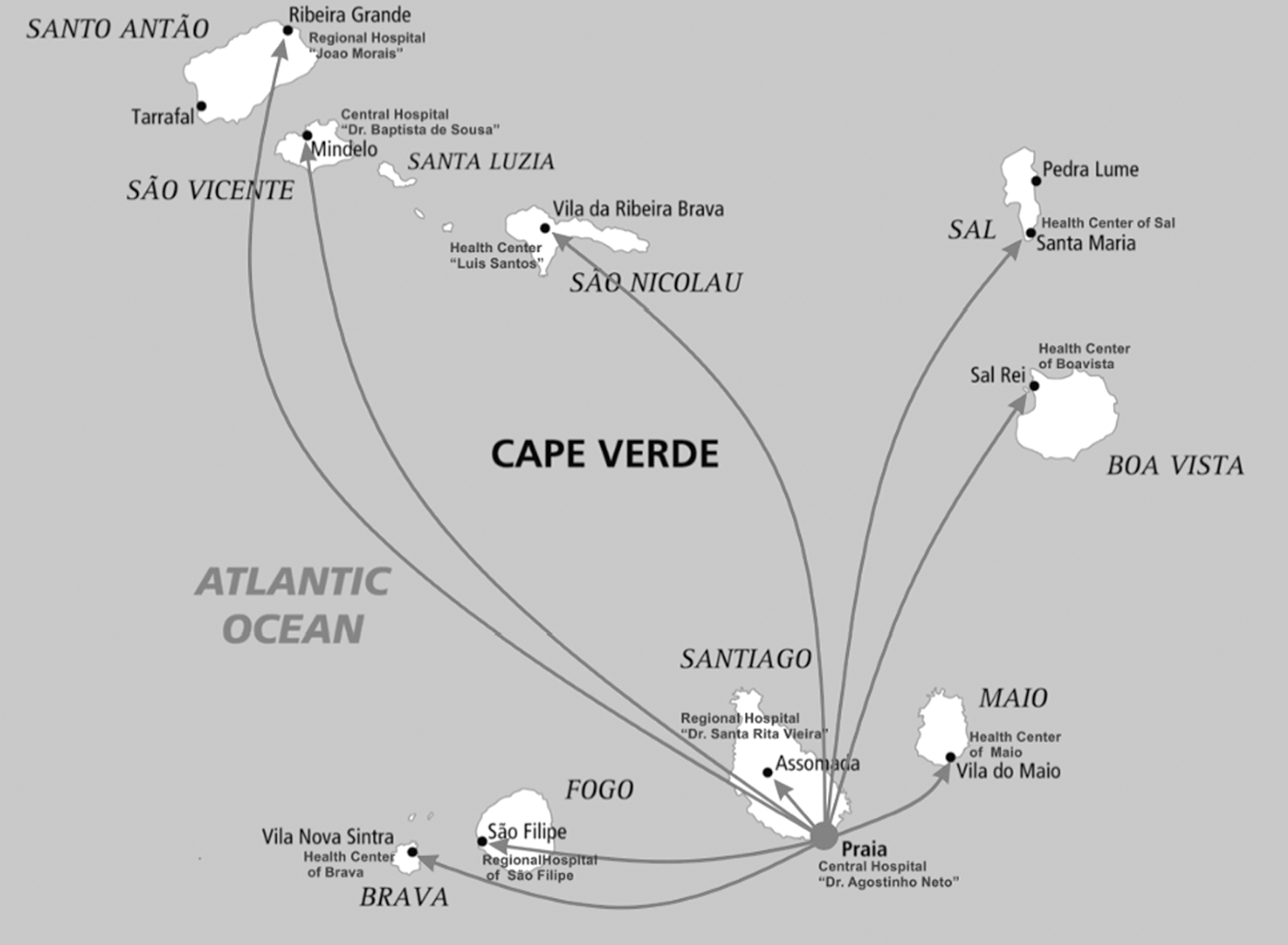
The telemedicine network of Cabo Verde, January 2014.
In total, 368 physicians and nurses (consisting of 42.9% of the country's workforce) attended either the national conference or one of the regional replicas. The conferences dealt mostly with content issues related to telemedicine, e-health theory and practice, and, to a lesser extent, current technology.
Our project team, in collaboration with the TeHL teams, finalized the first draft of our standard operating procedures and administrative forms. The legal package was submitted to the MOH-CV, which is now undergoing the pilot phase's study before an eventual official approval.
The most important legal document that was signed during our study period was the Order of the Minister of Health making teleconsultations mandatory before any medical evacuation, with only one exception: when the referring physician or team of physicians deems the life of the patient to be in imminent danger, based on their clinical judgment.
In addition, our project team collaborated with members of the five clinical telemedicine projects to develop technical and clinical protocols for those specialties. The draft protocol for image acquisition in teledermatology was the first to be completed, with several other drafts now in the pipeline.
Network Development and Deployment of Equipment
Starting in May 2013, biweekly technical checks and refresher training seminars have been conducted remotely. IVeH technical personnel from Prishtina, Kosova, and Tirana, Albania, conduct the training and checks, in collaboration with ITeHP-CV personnel in Praia. At least one technical expert and one doctor or nurse from each of the 10 telemedicine centers attends the biweekly technical checks and the refresher training seminars.
Implementation of Clinical Telemedicine
The clinical component of the ITeHP-CV started on May 15, 2013. From that date until December 15, 2013 (i.e., our initial 7-month reporting period), in total, 63 teleconsultations were conducted in nine medical specialties (Fig. 3 and Table 2). Teledermatology, telecardiology, and teletrauma represent the most consistently accessed specialties, offering teleconsultations almost every month of the reporting period.

Increasing number of teleconsultations during the first 7 months of the Republic of Cabo Verde telemedicine program.
Number of Teleconsultations by Specialty
Teleconsultations took place in real time for 84.1% of the cases and in store-and-forward mode for 15.9%; all of the store-and-forward teleconsultations were for teledermatology cases. The two dermatologists and the trauma surgeon performed the highest number of teleconsultations (57.3% of the total) during our initial 7-month reporting period. This reflects the need for these services and the preparation of local champions among physicians. Two of the local telemedicine centers referred 84.2% of the cases (one of those referred over 54.0% of the cases). The general practitioner with the highest number of requested teleconsultations referred 18 cases (28.6% of the total). This is a reflection of staffing or lack of specialties in some centers, such as Sal Regional Hospital.
In all, 15 physicians referred cases during our initial 7-month reporting period. Of those teleconsultations, 76.2% were by the team of doctors who were trained in Albania and Kosova. This element explains the need for physician training and fostering local champions, and one cannot expect that merely installing telemedicine equipment will foster the use and adoption by physicians. The most important trend during our initial 7-month reporting period was the increasing number of teleconsultations: in the first 2 weeks alone of December 2013, a record 22 cases (34.9% of the total) were accepted for teleconsultations.
Implementation of Activities Related to CME
The educational component of the ITeHP-CV started on April 5, 2013; the first lecture celebrated World Health Day 2013 (April 7th of each year). Since then, 18 CME sessions have been organized (an average of 2.25 sessions per month): 14 sessions were delivered by lecturers inside the country, compared with 4 by lecturers from abroad. The number of telemedicine centers in the Republic of Cabo Verde that connected to the sessions varied from two to nine; the highest attendance was reached for the last event of December 17, 2013, when the draft teledermatology protocol was discussed.
Establishment and Use of The Electronic Virtual Library
The two consulting hospitals were the first to complete the subscription process for HINARI (access is provided for free to the Republic of Cabo Verde). Use of the virtual library has not been as great as we had anticipated, possibly because of the fact that there is no medical school in Cabo Verde. We are currently in the process of revising our strategy for library usage implementation in order to encourage the assimilation of this valuable resource.
Discussion
The telemedicine program in the Republic of Cabo Verde (ITeHP-CV), which is being implemented by the IVeH, has been successfully launched. The IVeH, whose hallmark is the IBOT strategic approach, has been instrumental in rebuilding public healthcare systems in developing countries such as Kosova and Albania. 15 –17 The balance of responsibilities between the IVeH and the Republic of Cabo Verde in implementing this program has been notable. The Cabo Verde government is committed to e-government, and telemedicine is a logical extension to the overall strategy and the network that has been created. Furthermore, the collaboration among the Cabo Verde government, the donor, and the implementing agency is superb, with clear terms of references for each of the players. The Republic of Cabo Verde provided facilities, committed personnel, provided integration into overall MOH services, and provided a mandate for telemedicine transfer. The MOH needed telemedicine to reduce transfer costs between the islands and abroad. The IVeH, on the other hand was funded and committed to provide the strategy, policies and procedures, equipment, and training, plus clinical and technical support. Previous studies have demonstrated that telemedicine saves money. 14,15
The two previous national telemedicine programs for Kosova and Albania took much longer to complete (5 and 3 years, respectively), with a much later introduction of clinical activities. In contrast, the initial implementation of ITeHP-CV has gone much more quickly (7 months) and smoothly.
As already pointed out, Mars 12 and numerous other authors, reporting from different initiatives in the context of the RAFT Project, found that many telemedicine projects in sub-Saharan Africa benefited more from tele-education than from clinical telemedicine. Similarly, Meso et al. 18 and Weinberg et al. 19 found that, in Africa, distance education was the potential telemedicine success story, rather than other forms of e-health. However, the reverse was true during the first 7 months of our Republic of Cabo Verde experience: tele-education trailed clinical telemedicine consultations, in both the number of events and the frequency.
We have identified several driving forces responsible for this unprecedented emphasis on clinical telemedicine over tele-education, including our advance identification of national clinical priorities, careful preparation of clinical programs in collaboration with the TeHL teams, and continuous support and technical training. Likewise, Bediang et al. 20 cited good organization, careful training, and continuous support as key factors for the success and sustainability of efforts in the field of e-health in African countries. These factors are important in non-African countries as well. Specifically in Australia, Moffatt and Eley 21 reported the same factors as important prerequisites for implementing successful telemedicine programs, elaborating on challenges related to funding, physicians' time and skills, infrastructure, and equipment. Zanni 22 stressed that successful telemedicine programs depend on first identifying, and then fulfilling, a clinical need, which is exactly how our clinical telemedicine program started in the Republic of Cabo Verde.
Our finding that real-time delivery has, so far, been the preference in the Republic of Cabo Verde is contrary to the bulk of reports from the African continent. Meso et al. 18 reported that teleradiology in store-and-forward mode was a potentially successful clinical telemedicine approach for sub-Saharan Africa. Weinberg et al. 19 implemented the regional “African Teledermatology Project,” which used store-and-forward telemedicine to treat 345 patients from 13 African countries over a 2-year period. Brauchli et al. 23 described a store-and-forward Internet-based telemedicine platform (iPath) used in more than 1,800 teleconsultations in a teledermatology project in South Africa and in a telepathology project in the Solomon Islands. Puustjärvi and Puustjärvi 24 proposed cloud-based solutions as a means to mitigate developing countries' deficient Internet capabilities and lack of sophisticated peripheral support.
The two barriers cited by Puustjärvi and Puustjärvi 24 —deficient Internet capabilities and lack of sophisticated peripheral support—are exactly what we overcame in the Republic of Cabo Verde. The Internet provider there, the Núcleo Operacional para o Sociedade de Informação, managed to establish adequate Internet connectivity with each of the telemedicine sites through the combined use of optic fiber, dedicated lines, and microwave transmission. The heterogeneous network that resulted is still a far cry from the homogeneous virtual private network that IVeH has recommended as the connectivity modality of choice; however, this network is currently working well. In December 2013, for example, for a training session that grouped nine telemedicine sites, the video and audio multipoint communication was optimal. No interruptions or problems occurred during the training.
In addition to good Internet capabilities in the Republic of Cabo Verde, the ongoing peripheral support encompasses a multitude of needed telemedicine instruments: not only “classical” ones such as an e-stethoscope, vital signs monitor, and dermatology camera, but also the e-electrocardiograph and ultrasound probes. Such tools are essential for diagnosis and case management, enabling an integrated approach to patient care that includes long-term follow-up if needed. And, continuous support has been, and still is, provided: not only from trained and experienced technical experts from Albania and Kosova, but also from the presence of a professionally growing network of technical specialists at the telemedicine sites.
Last, but not least, we are confident that we have laid the groundwork for program sustainability—which remains a huge problem with telemedicine in Africa and elsewhere (even in developed countries). To help ensure the sustainability of ITeHP-CV, we introduced several measures (Table 3), incorporating various recommendations from the literature. Bediang et al. 20 listed several factors as key to sustainability of telemedicine and e-health efforts in Africa, of which the most important are lack of ownership by African stakeholders, lack of interoperability, as many of the projects are deployed by multiple organization, and, finally, lack of basic infrastructure and training support. None of these factors applies to Cabo Verde. For this reason we have previously cited the IBOT strategy, which ensures interoperability and creation of the infrastructure and completes a real ownership by local government and human capacity. 5 Shiferaw and Zolfo 25 in Ethiopia identified e-government readiness, enabling policies, and the capacity-building process as crucial components, noting that they consider telemedicine as being in a premature phase of development in Ethiopia and other sub-Saharan countries. Ajuwon and Rhine 26 highlighted the underutilization of e-resources in Africa and stressed the need for information communication technology training. With regard to the University of Arizona's telemedicine program in Panama, Vega et al. 27 identified the use of the country's assets as a critical factor to ensure sustainability.
Measures We Introduced in the Republic of Cabo Verde Telemedicine Program to Help Ensure Sustainability
ITeHP-CV, Integrated Telemedicine and e-Health Program for Cabo Verde.
Overall, although there are several initiatives of telemedicine in Africa, 28 –30 there is a need for establishment of new strategies in Africa in order ensure that telemedicine achieves its full potential. The Cabo Verde example may serve to change the paradigm from “project oriented and experimental” to sustainable programs owned and operated by local governments. There are several well-described strategies for how to achieve these results. 4,5,14,31
Several issues need to be elaborated in order for the sustainability of this program to be ensured. First, although the plans and the commitment of the government of Cabo Verde are that upon completion of the current project and funding from the Slovenian government to take over completely, this remains to be seen; however, currently the government of Cabo Verde bears the cost of connectivity, an impressive cable network in all islands that is run by the Núcleo Operacional para o Sociedade de Informação. This most likely will ensure connectivity for the future if the government continues support to the telemedicine program, as it does currently. Furthermore, the majority of local personnel involved in each hospital are supported by the MOH, and telemedicine activities are part of their daily clinical or technical routine. We are in the process of getting funding for another 2 years of support of the program, and this may prove sufficient to ensure proper transfer of the program to the MOH.
Second, currently, the majority of teleconsultations are done through live interactions and from a limited number of clinicians. Will this change in the future, and will the balance of store-and-forward versus live consultations change? This is difficult to predict. Our subjective impression is that it will, but this, too, remains to be seen.
Third, the use of the electronic library has not been optimal in this phase. Perhaps the lack of dedicated personnel to assist clinicians or because there is no medical school in Cabo Verde may explain this phenomenon. We plan to send a portion of the units of the electronic library to the nursing school, and this, hopefully, will increase the utility of this great source of knowledge.
The main strength of our study was our use of the scientific IBOT strategic approach, which has been described in numerous peer-reviewed articles as well as books on telemedicine and e-health. 5 Most important is that the IBOT approach has been used in one of the best examples of a sustainable, integrated telemedicine and e-health program, that of Kosova. There are several limitations to our study as well. These are the initial results of a nationwide implementation of a program. Despite the good start, the long-term results are not yet known.
Conclusions
The Republic of Cabo Verde telemedicine program has been successfully launched, and the initial results are encouraging. The signs clearly suggest that the ITeHP-CV will be a success story both in the short term and for the foreseeable future. However, long-term follow-up is required, and the sustainability of the program needs to be ensured.
Footnotes
Acknowledgments
This project was funded by the Ministry of Foreign Affairs of Republic of Slovenia, through the International Trust Fund, Ljubljana, Slovenia.
Disclosure Statement
No competing financial interests exist.