
Abstract
Introduction
Obtaining sufficient physical activity (PA) (i.e., 150 min of moderate-intensity activity per week) decreases the risk of developing heart disease, hypertension, type 2 diabetes, and certain types of cancer. 1,2 In recent years, the health benefits ascribed to PA have only grown and include benefits such as decreasing the risk for falls, osteoporosis, depression, and cognitive decline. 3,4 However, fewer than 10% of adults meet current PA recommendations, 5 and this percentage is even lower among subsets of the general population. Rural American adults, for example, are less active than urban or suburban adults and twice as likely to report limitations related to activity. 6 –8 Despite being a high-risk population, geographical isolation (e.g., limited transportation to treatment centers) and/or a shortage of healthcare providers in rural regions represent obstacles to disseminating health-based behavior interventions to rural America. 8 –13
One behavioral health intervention that eliminates treatment barriers is Internet-based contingency management (CM). In CM, motivational incentives (e.g., vouchers exchangeable for goods and/or services) are delivered contingent on objective verification of a target behavior. 14,15 For example, Stoops et al. 16 developed an Internet-based CM intervention to promote smoking cessation among rural Kentuckians. Technology-based CM delivery systems have also been shown to decrease alcohol intake, 17 increase diabetics' adherence to glucose monitoring, 18 and increase PA. 19
Although one criticism of Internet-based CM is that rural dwellers may lack Internet access, the reach of Internet-based CM can be expanded via smartphones. Over 92% of individuals worldwide subscribe to mobile phone services, at a growth rate of 24% each year, 20,21 and rural residents are among the demographic groups that have recently experienced a notable uptick in smartphone penetration. 22 Increased access to technology among rural Americans has presumably contributed—at least partly—to the growth of “telehealth” interventions (i.e., interventions that capitalize on electronic information and telecommunications technologies to support long-distance healthcare 8,23 ). Indeed, a rapidly growing body of research supports the feasibility, acceptability, and efficacy of technology-delivered (e.g., computer, mobile phone) health interventions that target rural individuals. 8,23 –28
Although the field of telemedicine and e-health holds substantial promise for reducing health disparities, implementing mobile phone-based health interventions in rural America is still a relatively new research venture, 29,30 and not all interventions have been successful. 28 For example, Heckman and Carlson 28 developed a phone-based intervention to reduce depressive symptoms among rural individuals with human immunodeficiency virus. Results indicated that telephone-delivered, information-support groups increased participants' perceptions of social support and decreased barriers to healthcare and social services, but depressive symptoms did not change. The authors suggested that one reason the intervention did not influence the main outcome variable was that it was not tailored appropriately for a rural population (e.g., group facilitators of the telephone-delivered program were from large, metropolitan areas and may have been unfamiliar with the challenges of living with HIV in rural environments).
One effective approach to developing tailored interventions is via community-based participatory research, in which systematic inquiry, participation, and action are combined to address health problems collaboratively. 31 –35 For example, “Shape up Somerville” used community-based participatory research to improve the weight status of children with an intervention that involved numerous individuals (e.g., children, parents, teachers, school food service providers) and incorporated strategies based on participants' self-reported barriers to obtaining a healthy weight. 36 Ecological interventions tailored to the needs of particular communities (e.g., developing site-specific strategies to increase walking at rural worksites) have also been effective. 37 –40 Thus, the first step in developing efficacious health-based behavior interventions for rural populations appears to be involving them in the planning process, such that the resultant interventions address their unique needs.
The above research suggests that (a) tailored interventions improve the health of rural Americans and (b) smartphones are an emerging tool for delivering these interventions. Thus, the present research is a first step toward developing a smartphone-based CM intervention to increase PA among a rural population. We have previously used Internet-based CM to decrease smoking 41 –43 and to increase walking in sedentary adults. 19 Inspired by recent community-based participatory research research, 34 –36,39,40 we assessed participants' PA behavior, barriers to PA, and opinions about a smartphone-based CM intervention that is currently in the development stage. The intervention, called the “Get Up and Go” program, will include similar features to those presented by Kurti and Dallery 19 such as goals, feedback, and rewards, but unlike in the previous work, we plan to tailor the intervention based on rural participants' unique PA barriers and preferred PAs. In addition to providing a foundation for making early modifications to the intervention, this work also gauges the acceptability of a smartphone-based CM intervention to increase PA among rural residents.
Materials and Methods
Participants
On hundred thirteen participants (30 males, 83 females) were recruited from two sites. Fifty-four participants completed an anonymous, institutional review board–approved survey at a health fair in Levy County, Florida, and 59 participants completed the survey at a Walmart in Starke, FL. Data were collected on two separate days in Fall 2013. To complete a survey, participants had to be at least 18 years of age and had to report living in a rural area. Participants provided their zip codes, and rural residency was verified using Rural-Urban Commuting Area Codes, a new census tract-based classification scheme that combines standard Bureau of Census Urbanized Area and Urban Cluster definitions with work commuting information to determine rural versus urban status (
Participants' Demographic Data
For continuous variables (e.g., age, physical activity [PA] categories), scores represent averages, and the error (in parentheses) is the standard deviation.
MET, metabolic equivalent.
Measures
The instrument administered to participants is available upon request to the authors. The survey consisted of 48 items, took approximately 10–30 min to complete, and was administered in a paper/pencil format. Tables, chairs, and lap desks were available at both recruitment sites. A “station” was set up at both sites (i.e., a table with a sign advertising that rural adults were needed to answer a survey about PA) that was manned by two research assistants.
To assess PA barriers (14 items), we combined questions from the Brief Risk Factor Surveillance System, 44 the National Health Interview Survey, 45 and other surveys developed for rural populations. 46 –48 This approach to instrument development is consistent with previous research. 49 –51 The barriers assessed included personal (e.g., too tired, not enough time, fear of injury), social (e.g., others discourage me), and environmental (e.g., stray animals, no safe place, poor weather) factors. Participants reported whether the circumstance was “not a barrier,” “somewhat of a barrier,” “a moderate barrier,” or “an extreme barrier.” There was also one open-ended question asking participants to describe anything else that prevents them from being active.
To assess participants' opinions about the “Get Up and Go” program (7 items), participants read the following program description: The program would require you to do physical activities with your mobile phone. You could put the phone in a pocket on your clothing or use an elastic belt when you are being physically active. The phone would monitor the length and intensity of your activity. It will also tell you when your goals have been reached. The program offers small amounts of money, a few dollars a day, when you meet your goals. The phone could also be used to tell your select friends or relatives about your progress, and they could send you text messages to encourage you.
Participants then placed an×in one of four boxes indicating whether they viewed intended aspects of the program (e.g., earning money for meeting goals, being active with friends) as “not at all helpful,” “somewhat helpful,” “moderately helpful,” or “very helpful.” Participants were also shown a list of activities (e.g., aerobics, dancing, walking) and instructed to check those that they would like to engage in during the intervention. Finally, one open-ended question invited participants to share other thoughts about how we could help them increase PA.
The third part of the measure contained demographic questions (20 items). Because income does not always provide an accurate index of financial security in this population, alternative items were used to assess socioeconomic status. 52 –56 Specifically, participants choose from four options to describe their financial security (1=I really can't make ends meet, 2=I manage to get by, 3=I have enough to manage plus some extra, and 4=Money is not a problem; I can buy whatever I want). In addition, participants were asked to describe how comfortably they would be able to pay an unexpected $500.00 medical bill (1=Able to pay comfortably, 2=Able to pay, but with difficulty, and 3=Not able to pay the bill). These questions have been used in several studies with rural participants 52 –56 and have been shown to be a valid measure of financial status in several longitudinal studies. 57,58 A continuous financial security scale (range=0–2, with 2 indicating highest financial security) was created by averaging the two items. The brief version of the International Physical Activity Questionnaire (IPAQ) 59 was used to assess PA levels. This 7-item measure asked participants to report the number of days, and the duration each day, that they engaged in moderate activity, vigorous activity, or walking. Although PA could come from varying domains (e.g., occupational activity, yard work, sport), participants were instructed to think only about those activities that were performed for at least 10 min. The last item asked participants to report the number of days (excluding weekends), and duration each day, that they spent sitting.
Data Analysis
Pearson chi-squared tests of independence were conducted to determine whether PA barriers, helpful aspects of the program, and preferred activities were related to demographic variables (e.g., sex, race, education) and/or PA status (low versus moderate). Low versus moderate activity scores were assigned based on cut points specified in the IPAQ scoring guidelines. 59 Bivariate correlations were conducted to determine whether the above variables differed based on participants' age and financial security. For all analyses, alpha was set at p=0.05.
Data from the IPAQ were summarized in terms of participants' (a) weekly PA across the three categories (i.e., walking and moderate and vigorous activities), (b) total PA (i.e., sum of the three categories), and (c) estimated sedentary time each week. PA was estimated by weighting the reported minutes per week of each category by a metabolic equivalent (MET) energy expenditure estimate (i.e., an estimate of the energy used by the body during the activity). Values for weighted MET-minutes per week were calculated as duration×frequency per week×MET intensity, which were summed across all three categories to produce the estimate of total PA per week. The following MET values were used: walking=3.3 METs, moderate PA=4.0 METs, and vigorous PA=8.0 METs. 59 Finally, participants received a categorical PA score based on the IPAQ guidelines 59 stating that high=total PA MET-min/week ≥3,000, moderate=total PA MET-min/week ≥600, and low=total PA MET-min/week <600.
Results
Participants were (on average) 45.1 years old (standard deviation=17.4) but ranged in age from a minimum of 18 to a maximum of 89. Seventy-six were white, 27 were black, 4 were Native American, 1 was Asian, and the remaining 5 were “other” (e.g., more than one race). Approximately half (46.8%) of participants attained education levels that included, at maximum, graduating high school. The mean financial security score was 1.21, a score that was identical to that obtained by the rural Floridian sample of Riley et al. 55 Thus, despite using a convenience sample, participants were demographically similar to the random sample of rural north Florida residents examined by Logan et al. 54 Forty-two participants received a PA score of low, 54 were moderate, and 17 participants left the IPAQ items blank (anecdotally, many of these participants reported not knowing how much PA they get). Finally, 92 participants owned a phone for personal use, and 56 owned smartphones.
Because preliminary analyses using chi-squared tests of independence (categorical variables) and independent samples t tests (continuous variables) indicated that only age differed across sites [t(108)=4.4, p<0.001 (i.e., participants sampled at the health fair were older [mean= 52.4 years, standard deviation= 16.3 years] than those sampled at the Walmart [mean= 38.8 years, standard deviation= 15.9 years])], the results of statistical analyses that we describe subsequently were conducted with data collapsed across site.
Figure 1 shows the distribution of participant responses for the extent to which various circumstances represent barriers to PA. The extent to which particular items posed barriers differed across race, education, PA status, age, and financial security status. Specifically, participants who identified as white were more likely than those identifying as any other race to indicate being self-conscious [χ2=26.0(15)] and having health problems [χ2=26.1(15)] as barriers, whereas those who self-reported as black were most likely to indicate not having the right clothes [χ2=27.3(15)] as a barrier (p values <0.05). Participants with lower educational attainment more commonly identified being tired [χ2=28.5(18), p= 0.055] and unaware of how much exercise was required for health benefits [χ2=32.3(18), p<0.05] as barriers than participants with higher educational attainment. Low-active participants were more likely than moderate-active participants to identify poor weather (39% versus 18.9%) [χ2=10.9(3), p<0.05] and marginally more likely to identify fear of injury (36.2% versus 18.9%) [χ2=7.5(3), p=0.057], too tired (60.3% versus 48.1%) [χ2=7.1(3), p= 0.068], and health problems (49.2% versus 24.5%) [χ2=7.3(3), p=0.064] as at least somewhat of a barrier.

Number of participants who endorsed various items as not a barrier, somewhat of a barrier, moderate barrier, or an extreme barrier to increasing physical activity.
Finally, being younger in age was associated with reporting being self-conscious (r=–0.19), childcare responsibilities (r=−0.25), and not enough time (r=−0.27) as greater barriers (p values <0.05). Participants with lower financial security also reported being self-conscious (r=−0.19, p<0.05) as a greater barrier. When given the opportunity to write additional barriers, 27 of 47 responses pertained to low motivation (e.g., not interested, too lazy) and/or injury (e.g., spine injuries, bad knees, hip problem).
Figure 2 shows the distribution of participant responses regarding how helpful different aspects of the intervention would be. With the exception of using the phone to track progress and receive feedback, all other items received a majority of endorsements as very helpful. In particular, participants reported that earning money for meeting goals and being active with friends and/or relatives, or others in the “Get Up and Go” program, would be very helpful. Females were more likely than males to indicate that using the phone to track progress would be at least somewhat helpful (73.2% versus 44.8%) [χ2=8.4(3), p< 0.05]. In addition, an inverse relation was observed between age and the extent to which various aspects were helpful, in that younger participants reported that earning money (r=–0.22), receiving messages from friends (r=−0.20), and being active with friends (r=−0.30) or others (r=−0.20) as helpful (p values <0.05). In response to the open-ended question soliciting other thoughts about the program, participants' suggestions involved capitalizing on other mobile phone-based capabilities (e.g., sending encouragement over social media Web sites, receiving e-mails with recommended workouts), and providing low-intensity and/or walking-based opportunities (e.g., organized walks in the community, “mild” PA requirements).
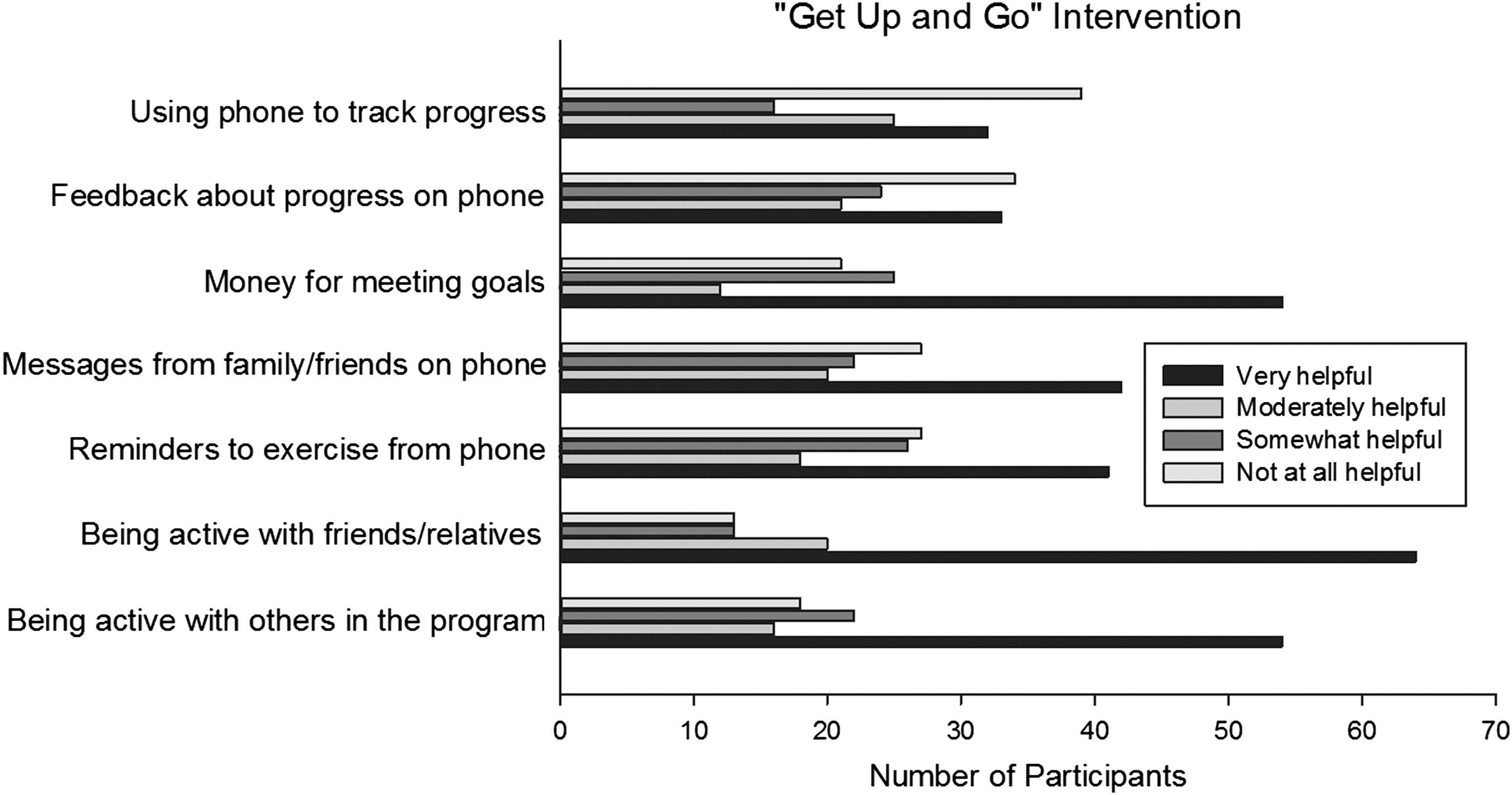
Number of participants who endorsed various aspects of the “Get Up and Go” intervention as not helpful at all, somewhat helpful, moderately helpful, or very helpful.
Walking was the only activity that a majority (87%) of participants reported wanting to engage in during the intervention. The second most popular items were biking (48.7%) and swimming (48.7%). On average, 64.9% of participants responded “no” with respect to whether they would like engaging in all other activities listed. However, females were more likely than males to identify dancing (46.3% versus 23.3%) [χ2=4.8(1)] and aerobics (28.0% versus 10%) [χ2=4.0(1)] as desirable activities (p values <0.05), whereas males were more likely to identify running (46.7% versus 17.1%) [χ2=4.0(1)] and basketball (50% versus 7.3%) [χ2=12.1(1)] (p values <0.01). In addition, moderate-active participants were more likely than low-active participants to report biking (58.3% versus 39.7%) [χ2=4.3(1)], basketball (22.2% versus 6.9%) [χ2=5.4(1)], and soccer (25% versus 5.2%) [χ2=5.9(1)] as desirable (p values <0.05).
Discussion
The present research evaluated PA behavior, barriers to activity, and opinions about a smartphone-based PA intervention among rural Floridians. Although barriers differed across several variables (e.g., age, PA status), participants identified most aspects of the intervention as helpful irrespective of these variables. Participants' favorable response to the program description supports the acceptability of smartphone-based PA interventions in rural communities.
Participants' positive response to the program description is consistent with previous research indicating that adults prefer home-based activity programs rather than instructor-led programs in gyms. 60,61 Furthermore, participants' preference for walking is consistent with research identifying walking as the preferred activity among sedentary individuals taking up PA, 62 as well as research indicating rural residents' positive attitude toward increasing PA via walking trails. 63,64 Our results also expand previous research by demonstrating rural residents' interest in a walking intervention delivered via smartphone.
Participants' self-reported barriers to PA are also consistent with those reported in previous research. 63 –65 In a systematic review of literature examining barriers and facilitators of PA among rural adults, Frost et al. 64 reported that, across studies, adults were more likely to obtain sufficient activity given pleasant esthetics, access to walking trails and parks, low crime, and walkable destinations. Our results also expand this work by demonstrating that barriers differ based on demographic variables and PA status. PA status also differentiated participants in terms of preferred activities (i.e., more active participants preferred activities other than walking alone). Thus, efforts to develop tailored PA interventions for rural communities should incorporate features that appeal to specific subsets of this target group.
Because the “Get Up and Go” program is in the development phase, participants' opinions are useful for designing the program for a rural population. For example, based on participants' strong interest in walking and positive views about earning money for meeting goals, the resultant intervention may provide financial incentives for meeting step goals. 19 In addition, because many participants were interested in being active with friends and/or others, the “Get Up and Go” program may incorporate a social component (e.g., organizing participants into teams with shared PA goals 66 ). Although 81.4% of participants owned a mobile phone, only 56% owned smartphones. These data suggest that either (a) the “Get Up and Go” intervention may be limited to rural dwellers with smartphones or (b) the cost of providing participants with smartphones must be built into the budget to fund the intervention. That being said, increasing numbers of rural dwellers can be expected to own smartphones in the near future. 22,67 From May 2011 to February 2012, the number of rural households owning smartphones increased 13%, 68 and this rate is expected to increase as phones and data plans become increasingly inexpensive. The growing ubiquity of smartphones may contribute to the sustainability of smartphone-based health interventions and minimize their cost.
In addition to guiding our own future research, results of the study have implications for other researchers as well. For example, having suggested the feasibility and acceptability of a smartphone-based PA intervention among rural individuals, the present study may justify future researchers' proposals to treat this population using smartphone-delivered health interventions. Additionally, researchers targeting participants of a similar demographic in PA interventions may use the present results to inform the development of their interventions (e.g., including group-based components). Finally, results of this study suggest some considerations that should be made with respect to developing PA interventions for rural residents, like taking preparatory measures to minimize circumstances that may pose barriers to intervention efficacy.
Study Limitations
Although promising, results of this study must be interpreted in light of several limitations. First, participants' self-reported PA may not index their actual activity levels, as people sometimes overestimate PA. 68 Objective measurement of PA may have categorized a larger portion of participants as low-active, therein providing a more convincing demonstration of the need for a PA intervention among this population. A second limitation—and a potential contributor to participants' positive response to the program description—is that participants completed questionnaires with the experimenters present; thus demand characteristics may have been present.
A third limitation is that a majority of survey respondents were female; thus results of the study may not generalize to rural Floridian males. In addition, respondents were not asked about their use and/or proficiency with current health management (e.g., PA) applications, or their general information technology literacy and/or experience. Asking these questions may have revealed differences in participants' conceptualization of the proposed intervention as a function of these variables. Ideally, we would have collected these informative data in the context of focus groups as opposed to surveys. However, given constraints on funding and time to devote to recruitment, focus groups were deemed infeasible.
Conclusions
In addition to providing a snapshot of PA behaviors and barriers, this work represents the first demonstration of the acceptability of a smartphone-based CM intervention to increase PA among rural residents. Based on research supporting the importance of tailoring interventions to the targeted population, 24,28,34,35 this work is a critical first step toward developing an innovative, efficacious smartphone-based intervention to increase PA among rural individuals. Given the demonstrated need for effective health-based interventions in rural communities, the “Get Up and Go” program, as well as other smartphone-based interventions, stands poised to substantially improve the health of this high-risk and historically underserved population.
Footnotes
Acknowledgments
We would like to acknowledge Lesleigh Craddock, Jessica Riedel, and Jessica Cowan for their help with data collection and data entry. We would also like to acknowledge Tanvi Pendharkar and Lesleigh Craddock for their help converting a previous version of this manuscript into AMA style. All of these students are current research assistants of Allison Kurti at the University of Florida.
Disclosure Statement
No competing financial interests exist.