
Abstract
Introduction
“Telemedicine” is the exchange of medical information and direct patient clinical services among distant sites through electronic communication. 1 There is abundant literature on the use of telemedicine for specialist consultation, direct patient evaluation, remote patient monitoring, and the dissemination of knowledge through Web sites. Data are growing about the application of telemedicine as a mentoring tool, or “telementoring.”
Telementoring provides guidance from a distance using virtual classrooms and virtual operating rooms. It has been used most commonly in surgical training, allowing surgeons at a remote site to offer intraoperative guidance through telecommunication networks. 2 Telementoring can also transform the learning environment through the use of “telepresence.” Telepresence uses a robotic audiovisual platform that can maneuver around the environment, creating a sense of “being present” at a remote site. 3 For example, patient clinical evaluations can be conducted from a remote site using robotic telepresence (RTP). At our senior author's institution, RTP is used as supervisory method for neurologic consultations conducted in the Emergency Department, as is further described below.
Teleneurology is an evolving branch of telemedicine. To date, teleneurology encompasses teleconsultation, teleconferencing, and tele-education. 4,5 Experience is limited about the specific role of teleneurology in trainee mentorship.
Since 2009, we have explored the use of teleneurology in RTP in graduate medical education. At our senior author's institution, RTP with the RP-7 Robot (InTouch Technologies, Inc., Santa Barbara, CA) audiovisual platform is used by faculty to supervise resident physicians during neurologic consultations conducted in the Emergency Department, particularly during neurologic emergencies (e.g., acute stroke evaluation) (Fig. 1). Essentially, RTP allows faculty at a remote site to manipulate around the examination room and directly interact with the patient and family in real time (Fig. 2). The average duration of a supervisory session is 40–60 min. The first half of the session focuses on bedside history acquisition, patient examination, and counseling of patients and their families. The second half focuses on private discussions between the faculty and trainee, including feedback and mentorship, neurological education, and debriefing of the telepresence experience.

Robotic telepresence used in faculty supervision of resident physicians during evaluation of a patient with acute stroke.

A faculty member at a remote site controls the robot, allowing for manipulation around the examination room and direct interaction with the patient and family in real time.
Before 2009, the gold standard at our senior author's institution was direct in-person staffing during the day for all cases and direct in-person staffing at night for all complex cases and neurologic emergencies. Staffing over the telephone was reserved for simple cases at night, followed by direct in-person supervision the next morning. Since the introduction of RTP at our institution in 2009, use of RTP as a supervisory tool has not been mandatory. Factors in favor of selecting RTP over direct in-person or telephone supervisory methods include night hours and weekends, junior-level trainees, simple cases, and faculty experience using telemedicine technology. Overall, the neurology faculty at our institution consider RTP an acceptable supervisory method for nighttime consultations and have largely, but not entirely, replaced direct in-person and telephone supervisory methods of these cases.
In the present study, we proposed that RTP can have a valuable role in graduate medical education through allowing for direct faculty supervision of trainees. Specifically, we compared three trainee supervision modalities during neurologic emergencies: telephone only, videoconferencing with RTP through the RP-7 Robot audiovisual platform, and the gold standard of direct, in-person supervision. We aimed to understand the advantages of each modality and to highlight the potential for implementing RTP as a valuable adjunctive tool for supervision and mentorship of trainees in neurology practice.
Materials and Methods
Thirty-six resident physician and fellow trainees and 10 faculty members were invited to be part of the present study, representing all physicians who had either conducted or staffed neurologic consultations in the Emergency Department at Mayo Clinic Hospital in Phoenix, AZ, from July 2009 through November 2011. Trainees consisted of neurology residents and fellows, as well as internal medicine residents rotating through the neurology services. In February 2012, an e-mail invitation was sent to trainees, asking for their study participation. Respondents were directed to a Web-based survey available through the
Responding participants answered 10 questions using a 5-point Likert scale or ranking. A separate trainee survey (Fig. 3) and a separate faculty survey (Fig. 4) were used to obtain data on respondents' experience with faculty–trainee interaction quality and clinical supervision. Specifically, the surveys gauged trainee and faculty satisfaction in regard to their ability to review and reacquire patient data, refine a trainee's impression, influence patient care, provide patient counseling, facilitate trainee autonomy, ensure adequate staff support, create efficient interactions, and facilitate learning opportunities. Each question assessed these factors across the three communication modalities under study, allowing for direct comparison among modalities. Survey results were analyzed with descriptive statistical measures. The Mayo Clinic Institutional Review Board gave exemption status to the study.
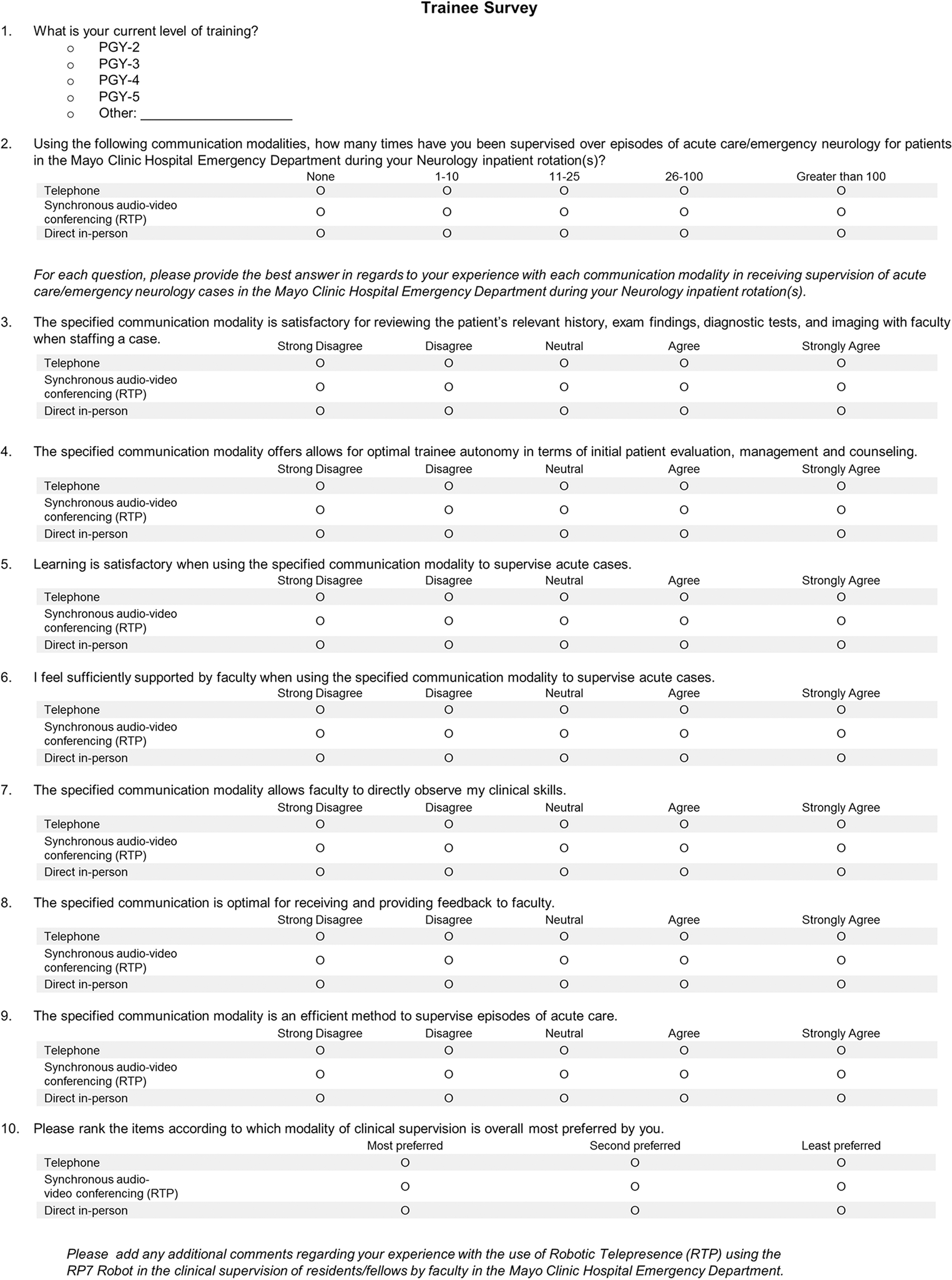
Survey of resident physician trainees on their experience with the three supervisory methods relevant to clinical supervision and faculty–trainee interaction. PGY, postgraduate year; RTP, robotic telepresence.

Survey of faculty members on their experience with the three supervisory methods relevant to clinical supervision and faculty–trainee interaction. RTP, robotic telepresence.
Results
Surveys were received from 20 of the resident physician trainees (55.5%) and 8 of the faculty members (80%). Of the trainee responders, 25% were in their second postgraduate year of training; 40%, their third; 10%, their fourth; 15%, their fifth; and 5%, their sixth. Among the responders, 90% had 25 or fewer encounters using RTP versus 60% and 55% using telephone and in-person modalities, respectively.
Of faculty responders, 37.5% had been on the faculty at Mayo Clinic for 5 years or less, 12.5% for 6–10 years, 37.5% for 11–20 years, and 25% for 21 years or greater. In comparison with responses of the resident physician trainees, faculty responses indicated that the disparities between their experience with RTP and their experience with telephone and in-person communication were even greater. Among faculty responders, those with 25 or fewer encounters using the RTP modality totaled 75%, compared with 25% using the telephone modality and 0% using the in-person modality.
More than 85% of faculty and trainees strongly agreed that direct in-person and RTP were satisfactory supervisory methods for reviewing a patient's relevant history, examination findings, diagnostic test results, and neuroimaging data with one another. By comparison, 15% of trainees and 37.5% of faculty believed the telephone method was unsatisfactory for patient data review. For reacquisition of patient data, reflection on and synthesis of patient data, and refinement of a trainee's impression, at least 87.5% of the faculty members strongly agreed that in-person communication was a satisfactory modality, compared with at least 62.5% with RTP. Moreover, 37.5% of faculty reported that the telephone method was unsatisfactory for these purposes. Among faculty responders, 100% agreed that direct in-person and 87.5% agreed that RTP were satisfactory modalities for influencing patient care and providing patient counseling. Yet, 87.5% of the faculty believed that communication over the telephone was unsatisfactory for patient counseling. In the trainees group, 88% agreed that the RTP modality allowed for optimal trainee autonomy in regard to patient evaluation, treatment, and counseling.
Most trainees (88%) reported the RTP modality also provided them with sufficient staff support, was efficient, and facilitated learning opportunities. In regard to direct supervision of clinical skills, 88% of trainees believed that videoconferencing was a satisfactory modality, whereas 85% believed telephone was unsatisfactory. In regard to receiving and providing feedback, 88% of trainees and all faculty members believed that RTP was satisfactory. Overall, 85% of trainees and 85% of faculty most preferred direct in-person supervision, with RTP a close second, and telephone being least favored (Fig. 5). Overall, a “dose effect” was not observed—that is, the results did not vary with RTP experience.
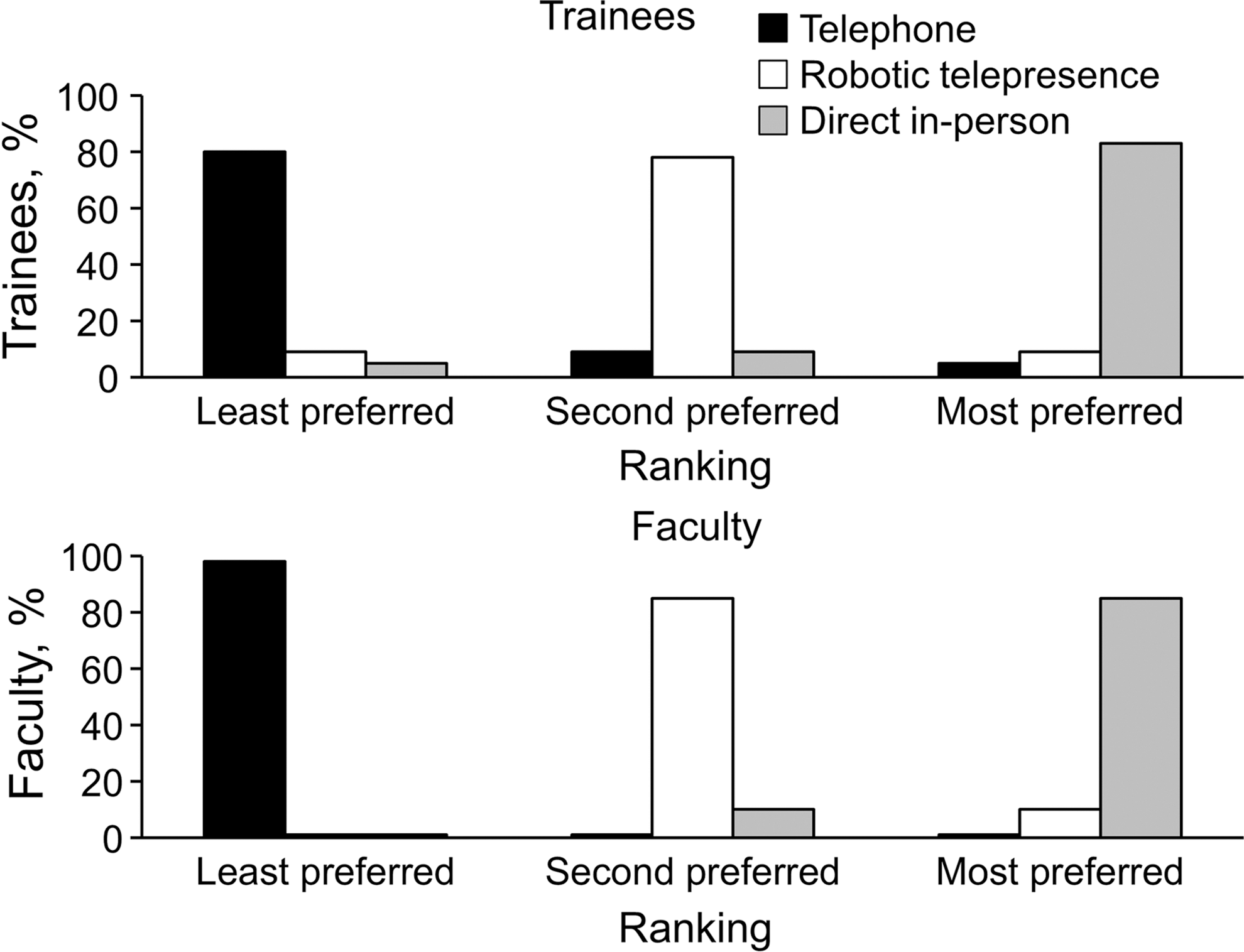
Ranking of the three clinical supervision modalities by resident physician trainees and faculty.
Discussion
Although the observations from the present study are preliminary, they add to the limited literature regarding mentoring, remote supervision, and educational applications of telemedicine in neurology teaching. This study shows that videoconferencing with RTP is perceived as a feasible supervisory tool that enables reliable clinical evaluation, provides case-based learning opportunities, and allows for direct supervision of clinical skills. These factors are fundamental in the medical education of trainees. This study also reports that videoconferencing with RTP is perceived as efficient, allows for real-time feedback, and optimizes the fine balance between trainee autonomy and supervision. Unlike the telephone and direct in-person supervision modalities, videoconferencing with RTP enables faculty to directly observe the trainee–patient interaction, as well as directly influence the episode of care in real time, while still allowing the trainee to remain the commander of the clinical interaction.
Although our study demonstrated that direct in-person faculty supervision of trainees' management in neurologic emergencies was preferred over videoconferencing with RTP, this type of supervision is not always practical. For example, in neurologic emergencies, faculty who take home-call responsibilities may not be able to be directly present at the bedside for the initial neurologic evaluation in a timely manner. Videoconferencing with RTP has the potential to improve the efficiency and timeliness of patient care.
As healthcare enters an era of limited duty hours, staffing shortages, and increasing use of midlevel providers, RTP has tremendous potential to meet the increasing training and staffing demands. With changes in healthcare and funding of graduate medical education, innovative solutions such as videconferencing with RTP have great potential interest and impact. Furthermore, the telephone method is still widely used across the nation as a supervisory method in the staffing of cases. This survey highlights that videoconferencing with RTP is preferred over the telephone method as an adjunctive supervision tool.
Can videoconferencing with RTP be substituted by a more economical option, such as a fixed-camera video teleconferencing modality similar to those on smartphones? Previous studies have noted that a mentor's ability to effectively move around the environment provides both the patient and the trainee with a feeling of the mentor's true presence. 6
Additional Telementoring Applications
Patterson and Gormley 7 demonstrated that implementing telemedicine through a real-time video link is an effective way to teach groups of medical students about patient consultation and neurologic diagnosis. Similarly, even before trainees are required to actively engage in patient care, videoconferencing with RTP can be used as a tool to prepare them for neurologic emergencies. For example, junior resident physician trainees can sit behind the camera and observe neurologic emergencies before intervening. In addition, RTP can be used in simulation scenarios with standardized patients, allowing for real-time feedback. Furthermore, telepresence sessions can be electronically archived into a library for review in an educational setting. RTP also allows for multipresence telementoring, such that multidisciplinary teams can be present virtually at the patient's bedside. With telemedicine being the wave of the future, Yudkowsky et al. 8 have highlighted that physician trainees must learn to communicate effectively over remote video links in order to function successfully in a telehealth environment. RTP can be used to prepare trainees for such teleconsultation. Finally, telementoring applications can address several core competencies, including patient care, communication, professionalism, and systems-based practice.
Strengths and Limitations
Strengths of the present study include its anonymous format and semiquantitative form of responses. Furthermore, this study assessed multiple factors in clinical supervision that are valued by both faculty members and physician trainees.
Several study limitations were identified. Our survey was conducted retrospectively, and the survey instrument has not been validated. The study design tests perceptions and was subject to both recall bias and responder bias. The present survey was a subjective measure of various factors across all three communication modalities. Research that is more quantitative in objectively measuring the direct effect of videoconferencing with RTP on trainee–faculty mentorship interactions is a potential future area of study. The study also had a small sample size. Furthermore, there was a low response rate among the trainees, raising a potential bias in the residents who responded to the survey. At the time the survey was conducted, most of our respondents (both faculty and trainees) had minimal experience using videoconferencing with RTP as a supervisory tool in neurologic emergencies. Future studies with a larger number of experienced participants will provide stronger evidence to assess the magnitude of the impact of videoconferencing with RTP. Finally, the present study was conducted at a single institution, and more research may be needed before results can be generalized to other centers.
Conclusions
Learning is maximal when self-directed, interactive, and practical. 9 Videoconferencing with RTP, when used for clinical training purposes, highlights these same qualities. Telemedicine technology used in the supervision and mentorship of resident physician trainees has the potential to transform graduate medical education, shifting the focus from the traditional teacher and classroom to an engaging learner-centered environment.
Footnotes
Disclosure Statement
N.M.K. reports no competing financial interests exist. B.M.D. previously served as a consultant for Genentech, Inc., as a member of an advisory group for CellTrust Corp., and as a consultant for REACH Health, Inc.
N.M.K. is responsible for study concept or design, drafting/revising the manuscript, acquisition of data, and analysis or interpretation of data. B.M.D. is responsible for study concept or design, drafting/revising the manuscript, acquisition of data, analysis or interpretation of data, and study supervision.