
Abstract
Introduction
Every day, thousands of Brazilians visit beauty salons (BSs), looking for beauty treatments that bring rejuvenation and health. Although there are poor professional regulation and official data on the number of beauty and aesthetics centers in Brazil, there are an estimated 2–3 million Brazilian beauty professionals (BPs). Procedures performed by both health professionals and BPs can involve potentially contaminated biological materials, which cause diseases. BPs perform activities that may generate potential disease transmission risks, due to the possibility of skin injury, unawareness of hygiene rules, and care of instruments.
There are more than 30 different sexually transmissible bacteria, viruses, and parasites that cause, among others, gonorrhea, chlamydial infection, syphilis, trichomoniasis, chancroid, genital herpes, genital warts, and human immunodeficiency virus (HIV) and hepatitis B virus infections. Several of those, in particular, genital warts, hepatitis B and C, and HIV infection, can also be transmitted through blood products and tissue transfer. 1
According to the World Health Organization, a million people are expected to be contaminated every day with sexually transmitted infections (STIs), including HIV infection. In developing countries, STIs and their complications rank among the top five disease categories for which adults seek healthcare. These infections can lead to acute symptoms, chronic infection, and serious delayed consequences, such as infertility, ectopic pregnancy, cervical cancer, and the untimely death of infants and adults. 2
In large countries like Brazil, it is difficult to provide continuing education and ensure properly qualified staff. Even though diagnosis and treatment are medical actions, anyone can be trained to suspect early signs and symptoms of STIs, including BPs. Our research group has developed a distance education course on STIs, indoor health in BSs, hand washing, and material sterilization, in order to improve early detection of STIs and to reduce disease transmission risk.
Materials and Methods
The present course with interactive tele-education tools was managed by the Discipline of Telemedicine (DTM) at the Medical School of São Paulo University (FMUSP), Pathology Department, São Paulo, Brazil, and was in accordance with the Cultural and Extension University Commission certification and accreditation requirements. Its technology infrastructure and multimedia development teams were committed to build educational resources through digital means with interactive features, such as educational projects, technological innovation, computer graphics design, and communication design.
The development of teaching materials engaged professors and staff at the FMUSP Hospital. With the help of experts in dermatology, nursing, infectious diseases, gynecology, urology, and telemedicine and with the analysis of governmental health surveillance matters, the method of topic selection involved the identification of hygiene process problems in BSs and the main disease transmission vectors. A spreadsheet for systematization of themes was developed by an expert in telemedicine and used, with the preparation of a matrix of objectives and skills, for planning a course with significant content in professional practice.
The course was accessed through a specific Web site called Interactive Digital Convention Center (

Beauty professionals' tele-education course: cybertutor (interactive learning environment).
The materials used included a digital classroom setting through Adobe® (San Jose, CA) Connect™ software that enabled implementation of Web conferencing at up to 100 different points, two scientific modules (on indoor health, hand washing, and material sterilization, in BSs, and another on STIs/AIDS), 20 materials for further scientific learning, 3 discussion lists (DLs), 4 applied educational videos, 20 audios with educational tips and information on STIs/AIDS myths and realities, 10 virtual human (VH) sequences, four Web debates videos, and one situations simulator (SS).
BPs and beauty students were selected on a first-come, first-served basis and by the remittance of personal documents to a specific DTM-FMUSP e-mail. The monthly 40-h course was free of charge, released on specific sites of São Paulo University and DTM-FMUSP.
Of the 85 participants, 82 were women, and 3 were men; 61% were BPs (52/85), and 39% were other professionals (33/85) (7 physiotherapists, 6 esthetics students, 3 nursing assistants/technicians, and 17 other professions [technology, communication, or freelancers]).
After enrollment, participants received an individual log-in and password to answer a virtual test, called SS, to evaluate the course participants' knowledge with the focus on the questioning and decision-making by BPs on daily practical situations (30 true or false questions). The themes were developed after the exchange of ideas with health and beauty experts together with a telemedicine and tele-education specialist. The same SS test (Fig. 2) was applied after the course.
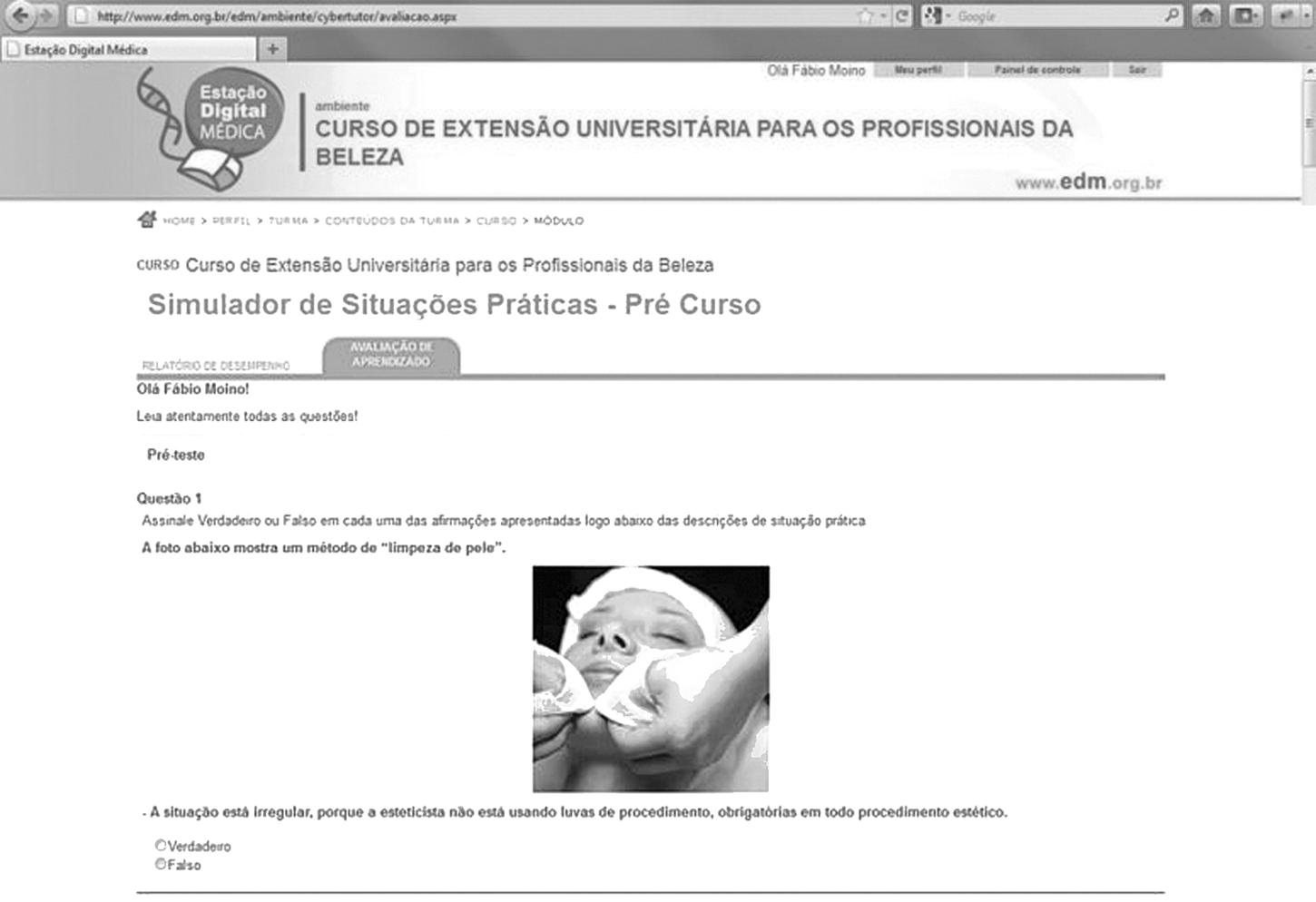
Beauty professionals' tele-education course: situations simulator.
At the beginning of the course, two face-to-face meetings happened at the DTM-FMUSP Technology Center in São Paulo City and in Curitiba City, the capital of Paraná State, at a preset day and time, in order to promote the group identification and to explain the goals and course dynamics progress, as well as to enable the participants to have their first exposure to the interactive material. The course sequence was carried out through the educational platform.
For the learning dynamics organization, the self-planning of tele-education included as activities both Web synchronous meetings (four 1-h weekly chats and four 2-h weekly Web conferences) and asynchronous resources (reading materials, DLs, SS, educational videos, and three-dimensional VH video animation on STIs and hand washing).
In relation to online activities, there were chats and Web conferences. The former, with a wide range of specialists, clarified practical questions and doubts from BPs, which covered four main themes: STIs/AIDS, indoor health in BSs, hand washing and material sterilization. The latter, supervised by the course coordinator and professors, had the participation of São Paulo hospitals (Hospital das Clínicas, FMUSP; Santa Casa de Misericórdia; and Emilio Ribas Institute of Infectious Diseases) and BPs from different parts of Brazil (Fig. 3).

Beauty professionals' tele-education course: Web conference.
Students who could not attend the face-to-face meetings and Web conferences had to attend the same recorded class available on ILE, as well as had access to the materials at all times directly on the specific Web site. After watching the videos, the students answered a multiple-choice questionnaire about the key words broadcast on the screen. Through the ILE, it was possible to verify who could or not access the available videos.
With regard to offline activities, supplementary literature was suggested to students for further scientific learning. DLs were designed to be accessed periodically. Audio-videos with educational tips and information on STIs myths and realities were recorded and available on the Web site. The VH (Fig. 4) is an educational learning object that uses three-dimensional computer graphics. Ten 2–3-min videos were produced to teach BPs to wash their hands properly and for the representation of main aspects of AIDS, syphilis, gonorrhea, genital herpes, and genital warts in men and women, in order to emphasize the early signs and symptoms of STIs.

Beauty professionals' tele-education course: virtual human.
An overall participation of more than 85% in course activities (chats, Web conferences, reading materials, DLs, audio-videos, the three-dimensional VH video animation, SS, and course quality evaluation) and a 70% approval grade in the SS postcourse test were expected. By achieving this result, the students were approved and awarded a certificate. For course evaluation, we used a questionnaire provided by the Cultural and Extension University Commission (available at
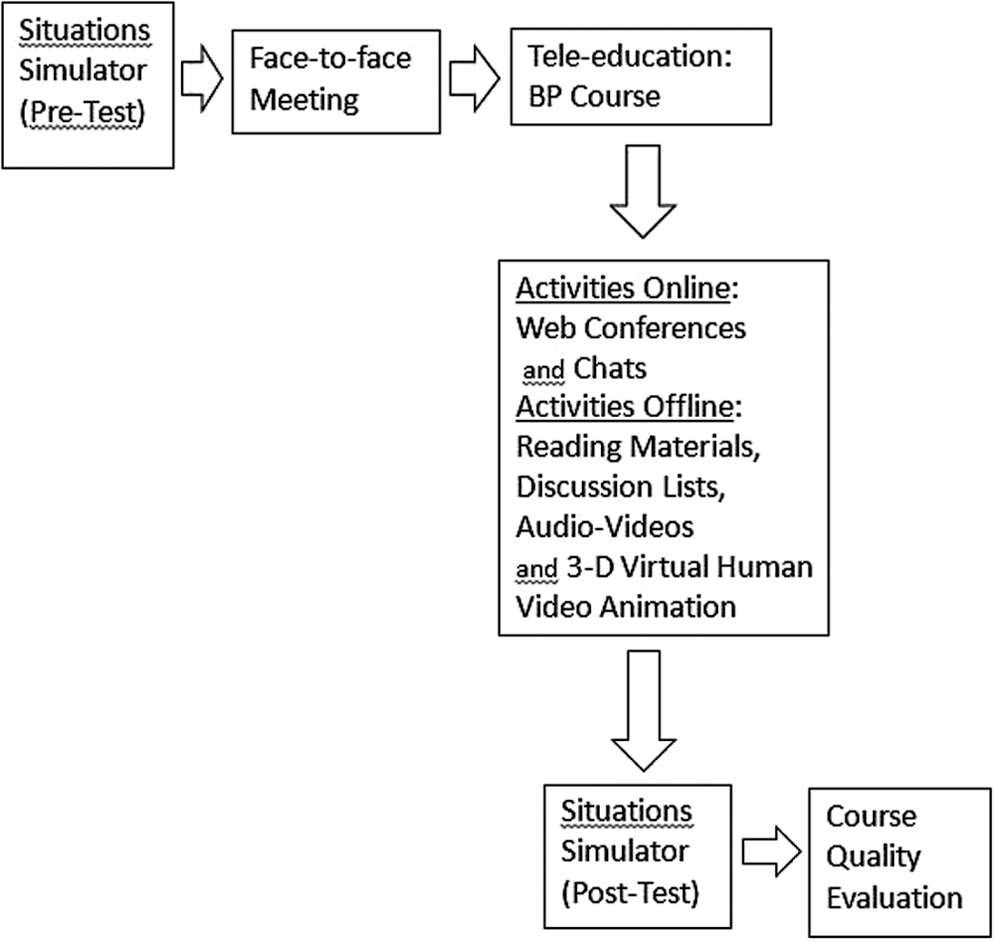
Beauty professionals' (BPs') tele-education course: course outline. 3-D, three dimensional.
Statistical Package for the Social Sciences (SPSS) software (version 17.0 for Windows; SPSS, Inc., Chicago, IL) was used for data analysis.
Results
The present study enabled the development of digital educational material to facilitate BPs' accessibility to excellent scientific contents produced at the university, as well as the creation of an ILE.
Forty-six percent (39/85) of the students had completed high school, 30% (26/85) had graduated from college, 3% (2/85) had finished elementary school, and 21% (18/85) were still attending college.
Regarding Internet use, 78% (66/85) used broadband Internet, 2% (2/85) used dial-up service, 5% (4/85) used mobile Internet, 8% (7/85) accessed the Internet outside the home (cyber cafes and workplaces), and 7% (6/85) did not respond. Regarding Internet access, 66% (56/85) accessed daily, 23% (20/85) weekly, and 4% (3/85) three times a month, and 7% (6/85) did not respond. Sixteen percent (14/85) had done a distance-learning course before.
At the course's end, 72% (61/85) participants were approved (met the requirements). On the other hand, 28% (24/85) of the students did not participate effectively in the course (minimum criterion of 85% activity participation) and/or did not reach the minimum grade of 70% in the SS postcourse test and thus failed: 9 students reported schedule problems in participating, 2 had technical problems on the computer/Internet, 1 had personal technical difficulties, and 12 did not answer.
The approved students showed a significant statistical difference (p=0.022) between SS pre- and post-tests, as analyzed by t test (Kolmogorov–Smirnov). 3
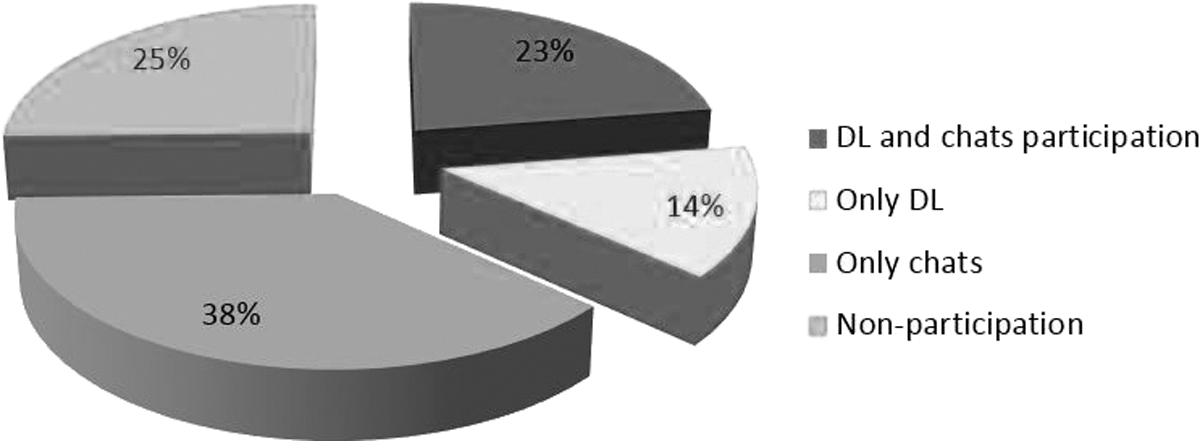
Figures 6 and 7 show the approved students' participation in the activities proposed.

Beauty professionals' tele-education course: participation in online activities (n=61).
Beauty professionals' tele-education course: participation in offline activities (n=61). DL, discussion list.
Of the 61 approved students, 25% (18/61) did not participate in the DLs or chats. Fifteen justified their nonparticipation as follows: 6 claimed technical difficulties, 4 noted an excess of daily activities, 3 had a scheduling conflict with the chats or no need to give personal comments on the DLs, and 2 reported technical problems on the computer/Internet. The 109 questions posted on the DLs were answered within 48 h.
After the course, all the attendees answered the course quality evaluation questionnaires. One hundred percent (61/61) of the successful students would recommend the course to a fellow professional, and 95% (58/61) would participate again in a similar course. Relating to course applicability to everyday life, 70% (43/61) considered it excellent, and 30% (18/61) labeled it good.
Table 1 shows the course activities evaluation by the approved students. In addition, approved students gave both three positive and three negative aspects arising from BPs' tele-education course participation, the frequencies of which are presented in Table 2.
Beauty Professionals' Tele-education Course: Course Activities and Satisfaction Level by Students
ILE, interactive learning environment.
Beauty Professionals' Tele-education Course: Positive and Negative Aspects
Discussion
In this study, we identified and produced materials with a meaningful amount of knowledge arising from a set of multiprofessional reflections to practical application in a course aimed at BPs. The educational content gathered scientific evidence to support changes in attitudes and routines in order to make improvements and raise BPs' awareness of correct professional practices.
Multiple learning tools such as Web conferences, educational audio-videos, DLs, reading materials, and assessment through the SS, in addition to VH video animation, provided a wide range of collaborative and interactive work.
Currently, there are several technical training courses in the beauty area, but none deal with common themes on health biosecurity, disease transmission risks, and work environment care. One of the major factors responsible for disease transmission even in a hospital is incorrect hand washing and irregular practice. In order to create a meaningful context, the VH video was provided to demonstrate areas with dirt accumulation and explain the reasons for hand washing techniques.
Approximately 2–3 million Brazilian BPs, who have different health knowledge levels and heterogeneous educational backgrounds, perform procedures with often dangerous habits that may cause disease transmission, such as the use of inappropriately sanitized metal instruments for different clients (like nail pliers), lack of hand washing, nonuse of procedure gloves, and the unawareness of health risks associated with their practices. 4
A significant participation of women and professionals from other segments in this course is partly due to the thriving Brazilian beauty market. This last assumption is certified by the Brazilian Association of Toiletries, Perfumes and Cosmetics, which states the beauty industry here has had an average deflated growth of 10% annually over the past 17 years, much stronger than the rest of the economy, and this is explained in part by the increasing participation of Brazilian women in the labor market. 5
BPs often do not have easy access to university education programs because of an incompatible educational level, constant commute difficulty, or schedule conflicts with other personal activities. In our study, most participants (46%) had only completed high school.
The training of Internet-based technological resources in the face-to-face meetings provided digital inclusion, adding value to the curriculum and to BS professionals' everyday life. Only 16% had done a distance-learning course before, but 78% had access to broadband Internet, and 66% accessed it daily. Technological equipment cost has been falling, which allows greater access to computing resources and Internet market availability.
Except for the face-to-face meeting, all other online activities were held mostly through the access to recorded videos available later on ILE. The possibility of customizing and making flexible the study schedule can increase adherence of the BP segment, according to the andragogical model based on self-direction in learning about relevant issues that contribute to solve common everyday problems.
The active participation of most students on DLs with 109 comments showed the important role of this educational tool: of the approved students, only 25% did not participate in either DLs or chats, and the majority reported technical difficulties as the main cause in the access of these ILE tools. It probably occurred because of participants' inexperience in courses supported by technology, or the fact that the use of some tools, such as chat and DLs, had been less intuitive on this educational platform. 6
Analysis of the answered course quality evaluation questionnaire demonstrates good acceptance of this type of intervention, and 100% of participants would recommend the course to other peer professionals. It also shows compatibility between the material offered and the assigned score, which reinforces the strategic planning focused on meaningful information with professional day-to-day applicability. Three tools with high approval rates should be highlighted: Web conferences, VH, and SS.
The Web conferences allowed a real-time interaction between health professionals and BPs to debate questions comfortably, without the difficulty of commuting (also to large urban centers) and the inherent risks such as of burglary.
The creation of VH videos, although costly, allowed important educational tools to transmit a large amount of content briefly, precisely, and in a focused way, supported by scientific relevance. Therefore, a spreadsheet systematizing the content of these learning objects was discussed with a telemedicine expert. 7
The SS creation strengthened the educational models that focused on the questioning and decision-making by BPs, in daily practical situations and not just as a cognitive assessment. The theoretical knowledge acquired over the course did not necessarily make the person understand what happened in practice, but it could support positive behavioral change.
At the course's end, students sent comments on the three main positive and negative course aspects (Table 2). Regarding the positive side, students reported learning, training, awareness, updating, experience, and sense of responsibility to prevent disease transmission in BSs as the most important aspects acquired through the course. Second, comments were made on the course quality itself, with emphasis on the materials (content, focus, and clarity), involved professionals, Web conferences, and SS.
Even with the asynchronous flexibility and the possibility of accessing study materials and videos through ILE at any time, most (26%) pointed to conflicting schedule as the most important negative point for fulfillment of all proposed activities. However, second most frequently, 18% reported no negative points, which shows good course acceptance.
As an increasingly common social habit nowadays, thousands of Brazilians visit BSs every day, and these places have become meeting points with potential spread of disease. BPs have a direct contact with many people, in particular, women, and may, if qualified, learn new habits that reduce disease transmission risk, learn how to suspect signs of potential STIs/AIDS, and know how to guide clients properly.
Although there are several temporary Brazilian programs to promote STIs/AIDS prevention, such as condom distribution in primary health centers, events, and festivities (Carnival), the implementation of a thorough and long-lasting official qualification program for non-health professionals, like BPs, can be a complement to prevention strategies. In our study, 70% considered excellent and 30% good the course applicability to everyday life, and 95% would participate again in a tele-education course like this. 8
Conclusions
This interactive tele-education model for BP training in disease prevention gained acceptance in this professional segment, and the measured learning shows a behavioral change improvement in practical situations.
The creation of an ILE with directed selected themes promotes distance learning focused on management and decision-making in the face of everyday practical situations.
The results demonstrate the feasibility of an interactive, tele-education model using low-cost tools as an educational resource to teach BPs. In the future, this may become a branch of nationwide telehealth action.
Footnotes
Acknowledgments
We would like to thank the course participants for their collective and participative spirit, the course teachers for their support, and all of the team of the Discipline of Telemedicine at São Paulo University's School of Medicine for their help in educational projects, technological innovation, computer graphics design, and communication design. Moreover, the authors are thankful to the reviewers for their significant contributions to this article.
Disclosure Statement
No competing financial interests exist.