
Abstract
Introduction
Obesity is problematic in American society and worldwide. In 2011 and 2012, more than two-thirds of adults were reported to be obese or overweight, more than one-third of adults were obese, and about 6.4% were extremely obese. 1 The World Health Organization reported that being overweight or obese is the fifth leading risk factor for global death and leads to at least 2.8 million adult deaths every year. 2,3 Overweight and obese individuals have a higher risk for diseases such as coronary heart disease, stroke, hypertension, type 2 diabetes, and certain types of cancer. 4 Obese individuals may also suffer from psychosocial problems such as depression, anxiety, low self-esteem, low quality of life, social stigmatization, and discrimination. 3,4 In addition, these negative outcomes result in higher healthcare costs. Recent reports estimate that weight-related healthcare costs total almost $147 billion in out-of-pocket, private, and insurance expenses. 4,5 Clearly, obesity is a significant problem in American society, one with adverse physical, social, psychological, and financial consequences.
An important fact is that obesity is largely preventable 2 and remediable. 5 For decades, healthcare providers and researchers have developed and studied the effects of weight-loss interventions (WLIs). They have found that WLIs reduced blood pressure, serum triglycerides, blood glucose, and serum cholesterol levels and increased high-density lipoprotein levels. 3 Indeed, weight loss can make individuals healthier and reduce their risk factors for chronic diseases.
Although overweight and obese individuals do lose weight successfully through these kinds of WLIs, previous studies have reported that participants quickly regain the weight after completing the interventions. 6 A recent report asserted that most participants regained about one-third of the weight lost during the year following the completion of an intervention program and tended to return to their baseline weight within 3–5 years. 7 This confirms that weight-loss maintenance is extremely challenging for participants who lose weight through short-term interventions. Researchers have developed and examined several strategies to maintain weight loss, such as ongoing therapist contact, training in relapse prevention, problem-solving therapy, providing prepackaged foods, and incorporating peer support. 6
Another weight-loss maintenance strategy—technology-based interventions—is one of the newest approaches and has several advantages. First, technology makes the information easier and quicker to access. 8 People can easily access Internet- or mobile phone-based programs to provide reminders to maintain their healthier lifestyles despite their other commitments. Second, technology-based interventions are less expensive than in-person interventions over the long term. Many individuals can access technology-based programs anytime and anywhere. Computers, tablet PCs, smartphones, smart TVs, and wireless Internet access have quickly grown in popularity. Companies are developing new fitness devices to monitor individuals' physical activities. The availability of such technology means there is great potential to augment or improve interventions and to offer participants powerful tools. In addition, technology-based interventions can provide a private, varied, and rapid contact using computers, tablet PCs, or smartphones that can access WLIs through the Internet or downloadable applications. 9 Secure, personalized access can be used to provide enhanced cultural and personal sensitivity. 8 Therefore, particular programs can be personalized for specific users.
A previous meta-analysis revealed significant evidence that the use of Web-based interventions improved behavioral change results and increased exercise time, knowledge of nutritional status, and knowledge of healthcare, among other concerns. 10 Also, several reviews have recently examined the effectiveness of technology-based interventions. 4,11,12 However, there are relatively few weight-loss maintenance interventions (WLMIs), and few studies have discussed technology-based WLMIs.
The purpose of this article is to review the randomized controlled trials of technology-based WLMIs for adults published since 2000. The following research questions were the focus of this review: • Q1: What are the characteristics of the primary studies of technology-based WLMIs? • Q2: What is the quality of study designs of the primary studies? • Q3: Are the technology-based maintenance interventions effective in maintaining weight loss?
Materials and Methods
Article Identification Search Strategy
A systematic literature review of scientific journal articles published since 2000 was conducted using the following five electronic databases: OVID Medline, CINAHL, PsycINFO, Compendex, and PubMed. Key words were selected in accordance with the review purpose to include three main concepts of interest: purpose and length of intervention, outcomes, and technologies used. Therefore, key words were “long term*,” “maintain*,” “sustain*,” “weight loss,” “weight gain,” “body weight change,” “telecommunication,” “telephone,” “cellular phone,” “Internet,” “telemedicine,” “technology,” and “wireless technology.” The search was limited to journal articles published in English since 2000. In addition, a manual citation search was performed of the reference lists of the selected articles.
Selection Criteria
Table 1 shows inclusion and exclusion criteria. The criteria were developed to narrow the results and to focus on the rigorous research studies conducted on technology-based WLMIs. Selection criteria were established according to population, study design, intervention, publication type, and outcome. Only journal articles published after 2000 were included because technology-based interventions are a relatively recent development. Articles were included when they were published in a scientific journal, reported quantitative body weight changes, and conducted a technology-based intervention for maintenance of weight loss that performed random assignment.
Search Criteria
Articles that targeted specific illnesses were excluded, except for those that focused on cardiovascular disease risk factors, such as hypertension, diabetes, and dyslipidemia. Because many studies' long-term goals were to prevent cardiovascular diseases or other chronic diseases, cardiovascular disease prevention studies were also considered relevant to the present review. Eating disorder groups and post–gastric bypass surgery groups were excluded because the specific nature of their disease or surgery serves as a guide to different intervention strategies. Secondary analysis studies, such as cost-effective analyses and review articles, were excluded. Those articles that reported only WLI and did not report WLMI were also excluded (see Appendix 1).
Data Synthesis
To examine the characteristics of primary studies, data were extracted from the original studies. The study quality was measured according to the nine methodological characteristics tool developed by Norman et al. 8 (see Appendix 2). Originally, Norman et al. 8 established the study quality coding criteria to rate methodological characteristics for e-health interventions. In this article, the study quality coding criteria were adapted for this review to assess the quality of the studies identified. The score given to each study was calculated as a percentage of the maximum score. In addition, each study was categorized by the level of effectiveness of the technology-based WLMI to facilitate the maintenance of weight loss. Meta-analysis was not conducted because of the heterogeneity of the studies and the lack of data.
Results
Study Selection
Eight original studies were identified. Figure 1 shows the flow diagram of study selection that was used for identifying the studies. The 166 records were identified through the electronic search databases OVID Medline, CINAHL, PsycINFO, Compendex, and PubMed. An additional eight records were identified through a manual search of article reference citations. After duplicates were removed, 82 studies remained. Then, 41 articles were excluded after articles were screened by title and abstract. Twenty articles that did not meet the inclusion criteria were excluded, and 21 WLI studies using technology were identified. 7,9,13 –31
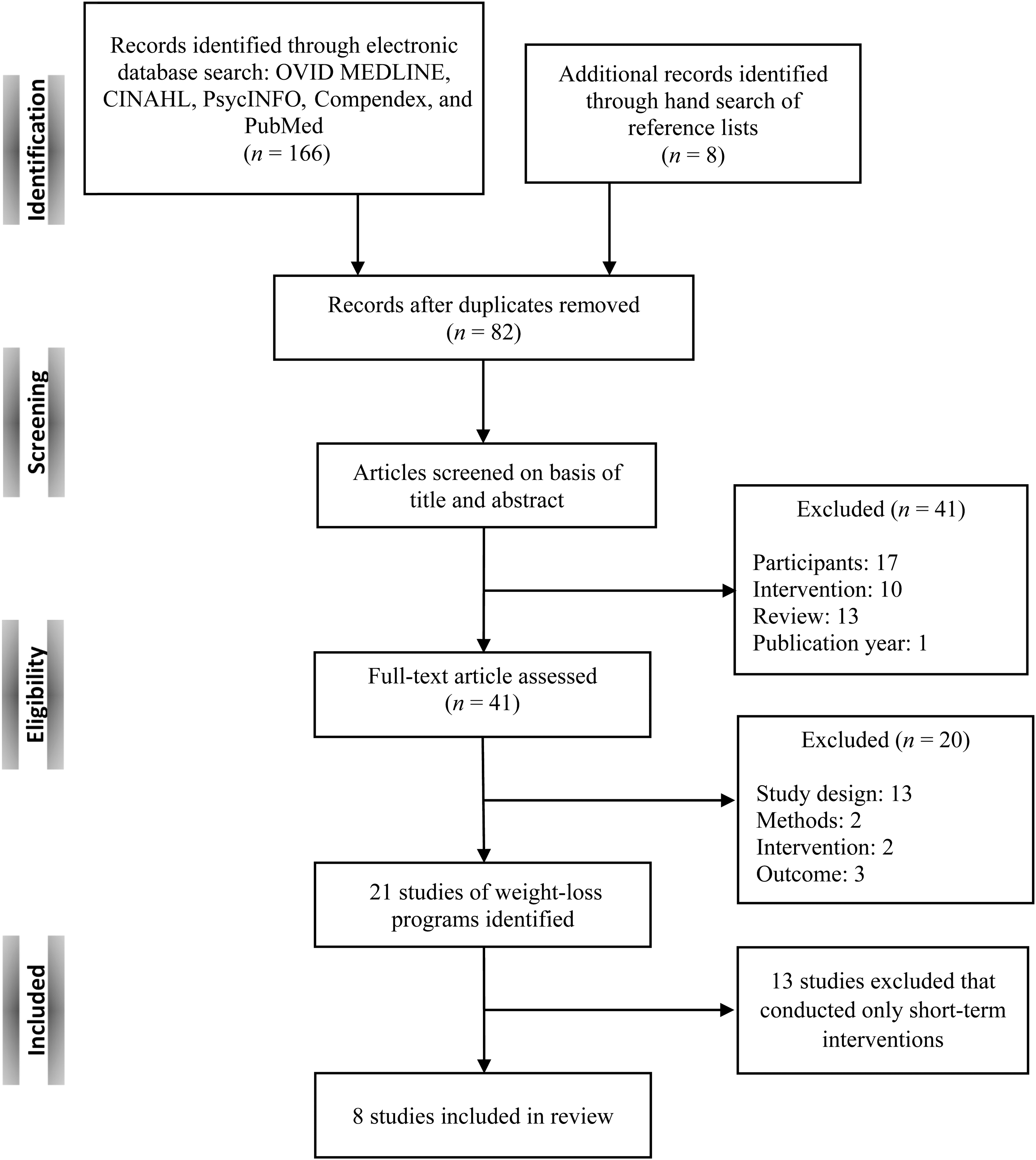
Flow diagram of study selection.
Many technology-based WLIs have been conducted over the last decade using the telephone, 13 –16 the Internet, 7,9,14,17 –21 remote support, 22 computer, 23 e-mail, 24 Web sites, 13,25 –27 mobile phones, 28 text messaging, 29 a tailored expert system, 30 or interactive technology. 31 This article focused on technology-based WLMIs. This focus led to 13 studies being excluded because they examined only WLIs (during primary program implementation), not maintenance interventions. Appendix 1 provides a summary of the 13 studies and the reasons they were excluded. Finally, eight studies were identified that used randomized controlled trials and conducted technology-based WLMIs; these were subjected to description and evaluation. As an exception, the study of Wing et al. 7 added value because it focused on the maintenance intervention for participants who lost weight over long periods.
Characteristics of Included Studies
All eight studies conducted two-arm 9,17 or three-arm 7,15,19,20,21,31 randomized controlled trials. Table 2 shows the summary of these eight primary studies according to population, intervention, comparison, outcomes, setting, and publication year (time). The most recent study was published in 2012. 17 In each of these studies, more women were recruited than men. The majority of the studies' participants were in their forties 9,17,19,20,21 and fifties. 7,15,31 The participants were either overweight or obese (mean body mass index range, 27.5–37.1 kg/m2). Their health characteristics were diverse. Participants were generally healthy adults (employed), 17 perimenopausal women, 9 obese women in rural areas, 15 women with hypertension, dyslipidemia, or both, 31 or healthy, overweight, and obese adults. 19 –21
Summary of Characteristics of the Primary Studies
Data for age and body mass index (BMI) are mean (standard deviation) values.
Total number in study (at randomization).
Recalculated from the original data.
p<0.05, for differences between groups.
Not reported by groups.
BP, blood pressure; CG, control group; CI, caloric intake; DI, dietary intake; EEE, exercise energy expenditure; EG, experimental group; EI, energy intake; FL, fasting lipids; FSG, fasting serum glucose; NB, nutrition behavior; PA, physical activity; RCT, randomized controlled trial; WC, waist circumference; WLI, weight-loss intervention; WLMI, weight-loss maintenance intervention.
The studies focused on the changes in the participants' weight, body mass index (BMI), blood chemistry, cardiovascular disease risk factors, physical activity, and dietary intake. Additionally, one study measured the participants' self-reported overall health as “excellent, very good, good, fair, or poor.” 17 Another study analyzed the Spearman correlation coefficients of the Internet log entries with changes in weight, exercise energy expenditures, and energy intake during the maintenance period. 9 Several investigators analyzed the adherence 15,19 –21 to and cost-effectiveness 15 of weight-loss programs. The studies included maintenance interventions immediately following the same short-term interventions and randomization. The WLIs were 10 weeks–6 months long, and the WLMIs were 22 weeks–30 months long. Svetkey et al. 31 performed the longest intervention, which lasted 30 months.
Table 3 summarizes the primary studies' measurements and results. In terms of retention rates, the rates for Experimental Group 1 (technology-based WLMIs) were lower than those of the control group or Experimental Group 2 or 3 (non–technology-based WLMIs). During the WLI period, participants lost significant amounts of weight (−2.7 to −9.4 kg) except in the study of Wing et al. 7 Among the studies reviewed, the participants in the study of Perri et al. 15 lost the largest proportion of body weight. However, all participants regained the weight during the maintenance period (0.4–5.5 kg) except those in the study of Harvey-Berino et al. The longer WLMI studies tended to report more weight regain. 31
Summary of Measurements and Results
Data are numbers for the recruitment, enrollment, allocation, and completion stages (by groups), respectively. The percentage of retention rate is calculated from the original participant numbers.
Weight is given as mean or mean (standard deviation) value.
Recalculated from the original data.
p<0.05, e p<0.001, for differences between groups.
Not reported by groups.
BMI, body mass index; CG, control group; EEE, exercise energy expenditure; EG, experimental group; EI, energy intake; FTF, face-to-face; MVPA, moderate to vigorous physical activity; PA, physical activity; WC, waist circumference.
Most of the studies used reliable measures to assess outcomes. The majority used a calibrated weight scale with the participant wearing light clothes and no shoes. To measure physical activity and dietary intake, various questionnaires were used. Of the eight studies, four used the Paffenbarger Physical Activity Questionnaire 32 to measure physical activity, and three studies used the Block Food Frequency Questionnaire 33,34 to measure dietary intake. The majority of the studies stated their measurements clearly, using tools that had been tested for their validity and reliability through previous research studies. (For more specific details on this result, see Table 3.)
Quality of Study Design
The range of study design quality scores across the studies was from 55.6% to 100%. The average score was 80.9%, which is moderate. Table 4 shows the results of the study design quality assessment and characterized results of effectiveness in maintaining weight loss. All studies met the individual randomization, control group, and pre- and posttest design standards. Three studies reported that they conducted paired, blocked, or stratified randomization, 7,17,31 whereas other studies mentioned randomization briefly. Six studies had a non-technological comparison group, such as face-to-face counseling, 7,15 personal contact, 21,31 frequent in-person contact, 19,20 and minimal in-person contact. 19,20 All studies tested the effectiveness of designed technology-based interventions except the study of Thorndike et al. 17 ; its maintenance intervention consisted of two components: Internet and personal contact. The average retention rate for all of the studies was 84.7%, but three studies' retention rates did not exceed 80%. 17,19,20 Three studies reported significant differences among groups at baseline on some variables, 9,15,17 and one study did not mention any group differences at baseline. 21 A majority of the studies conducted analyses with consideration of missing data that maintained the fidelity of the randomization such as the baseline-observation-carried-forward method, 9,17 intent-to-treat analysis, 19,20 missing-at-random assumption, 15 or imputation. 31 All studies mentioned their measurement validity information, except the study by Thorndike et al. 17 ; these investigators mentioned their measurement methods but did not fully describe their validity or make references about nutrition behavior and overall health.
Quality of Study Design Scores and Effectiveness of Maintaining Weight Loss
The quality of study design scoring was adapted from that of Norman et al. 8
Mean score of total percentage, 81.96%.
Direction of the effectiveness of maintain was coded as follows: “++”=technology-based intervention resulted in significant maintenance in weight loss compared with pure control group; “—”=technology-based intervention resulted in no significant maintenance in weight loss compared with pure control group; “+”=technology-based intervention resulted in significant maintenance in weight loss compared with non-technology comparison group; “−”=technology-based intervention resulted in no significant maintenance in weight loss compared with non-technology comparison group.
N, no; UK, unclear/unknown; Y, yes.
Effectiveness in Maintaining Weight Loss
There were various results in terms of effectiveness in maintaining weight loss. The researchers in three recent studies concluded that technology-based maintenance interventions did not improve outcomes 17 or work better than self-direction in sustaining weight loss. 9,21 However, several studies reported that technology-based maintenance interventions allowed for sustained weight loss better than that of the control group 7,15,19,31 but not better than non–technology-based maintenance interventions. 7,15,31 Therefore, the results of the effectiveness of technology-based WLMIs were mixed in the primary research studies.
Discussion
In a search of the literature, eight studies were identified. Those selected for review were randomized controlled trials to evaluate the effectiveness of technology-based WLMIs in sustaining weight loss. Neve et al. 11 also conducted a systematic review with meta-analysis to evaluate the effectiveness of Web-based interventions, published in 2010. They concluded that Web-based interventions have the potential to achieve outcomes to change other lifestyle behaviors; however, they also questioned the effectiveness of Web-based interventions for weight loss and weight-loss maintenance. 11
Khaylis et al. 4 also qualitatively reviewed the efficacy of technology-based WLIs and identified the five components necessary to succeed in enabling a successful weight-loss program: “self-monitoring, counselor feedback and communication, social support, use of a structured program, and use of an individually tailored program.” They concluded that long-term results are varied, although the short-term goals of technology-based intervention programs have been accomplished.
This review article supports previous review studies that report that long-term WLMI studies using technology have mixed findings. The article adds to the literature beyond previous reviews of long-term outcomes of WLI with its specific focus on the use/testing of technology-based interventions that were implemented during the maintenance phase (not just follow-up after a technology-based intervention). From this review, it is evident that there is a strong need to find an effective way to improve study interventions and protocols that will affect the weight-related outcome.
Suggested Guidelines for Technology-Based Maintenance Interventions
From the above review of eight studies, six guidelines have been derived that suggest ways to use technology-based WLMI methods effectively: • Tailor the technology-based maintenance intervention for specific subjects.
17,31
• To improve retention rates, develop additional sessions for special concerns.
15
• Consider having participants keep weekly self-weighing and diet logs.
7,9,15
• Check participants' technical abilities.
21
• Consider an occasional personal contact component to complement the technology-based maintenance intervention.
20,31
Svetkey et al. 31 elaborated that it is very important to provide more tailored interventions to achieve greater benefits because different individuals may prefer different types of interventions. They also reported that social support, reengagement, and motivation may need to be strengthened for long-term success. Thorndike et al. 17 conducted a wellness program to modify employees' diet and exercise behaviors. The researchers focused on a specific population (employees) in a specific environment (a workplace). They reported that the employees became less motivated to participate in the less intensive 9-month maintenance intervention and that utilization of the Web site was relatively low in comparison with the 10-week intervention. These results showed that long-term maintenance interventions may need more specific intervention strategies focused on the workplace and on the employees. Therefore, more tailored interventions are needed on long-term aspects 31 for specific subjects and environments. 17
Generally, 20–25% attrition rates were observed in behavioral weight-loss programs. 34 The retention rates of the eight primary studies were in this range, but investigators could improve their retention rates by using additional sessions to satisfy participants. Perri et al. 15 designed additional sessions for women in rural areas, such as low-calorie cooking techniques and performance for a healthy eating plan while away from home, to cope with the lack of family or friend support while losing weight. It is interesting that these researchers reported the highest retention rate among eight studies. Therefore, it is possible to conclude that the special additions make participants more likely to stay in the study.
Cussler et al. 9 stated that there was considerable variation in weight changes during the 12-month weight maintenance period within the Internet group. The weight change range was 12.2–20.9 kg, so the authors assumed that the amount of weight change might reflect differences in the degree of Internet usage during the maintenance period. In addition, Harvey-Berino et al. 19 tested participants' computer experience and comfort, attendance, and adherence. It was surprising that the attendance rate was better for the in-person group than for the Internet group. Moreover, the technology group's retention rate was relatively low in the majority of studies. These results indicate that investigators should simplify the interface, make it more convenient to use, and encourage participants to use technology more frequently.
Cussler et al. 9 also reported that the diet log was correlated with a change in weight (p<0.05). The authors mentioned that the logs helped participants feel at ease and might have encouraged more mindful eating habits. Perri et al. 15 also mentioned that completing the food logs mediated between extended-care counseling and long-term weight-loss success had a direct effect on the self-regulation theory (self-monitoring). Wing et al. 7 also reported that daily self-weighing was associated with effective weight maintenance.
Harvey-Berino et al. 19 –21 tested the acceptability for participants of their group assignment. In early studies they found that some participants did not have a computer equipped with technology such as a sound card and speakers. 21 Use of the Internet and mobile phones became more popular with middle-aged or elderly people. However, there can still be barriers to the effective use of these technologies. Investigators should check the participants' abilities and their devices to make sure participants can use the technology properly.
Svetkey et al. 31 concluded that personal contact interventions were effective across all subgroups. Although the intervention contact was only a 10–15-min telephone conversation, it still increased the effectiveness of weight-loss maintenance. Researchers suggested that occasional personal contact may be needed to augment technology-based interventions. Other studies reported that face-to-face contact produced the best outcomes. 7 Therefore, personal contact can be added to technology-based interventions to increase the likelihood of weight-loss maintenance.
Limitations
There are several limitations in this article. First, publication bias should be considered. Only electronic databases were searched. At RCT.org, many studies are listed as currently being implemented throughout the United States. Because of time-consuming data collection and publication processes, it takes significant time to prepare articles for publication. In addition, some studies are not published, including those with nonsignificant results or negative results. Second, only English-language journal articles were included. Issues related to being overweight and obese exist all over the world. More evidence might be published in languages other than English. Third, only a few studies were included. Previous studies included large ranges of intervention periods for weight-loss programs that were implemented. In this article, the focus was on long-term, technology-based WLMIs. It was difficult to find articles that satisfied both criteria (i.e., use of technology and application over the long term). In a few years, more studies will be published that will meet the inclusion requirements. Fourth, there was a lack of weight change data in the original studies. One study did not report body weight changes in each group, making it difficult to compare its results with those of other studies. 21 In addition, some studies provided either a standard deviation or a confidence interval for weight change, but other studies provided only weight change. If there were more data, a meta-analysis could have been conducted. Fifth, there is considerable risk of bias in individual studies and across studies. To enhance the validity of study review, pairs of reviewers or peer reviewers can work independently. In this article, no assessment of risk of bias was performed.
Conclusions
The current obesity epidemic is problematic in the United States and worldwide as well. Overall, investigators of most of the studies agreed that technology could be a more effective tool in preventing weight gain than self-directed maintenance alone. However, some questions remain about the efficacy of technology-based WLMIs. In this review, results of the effectiveness of technology-based WLMIs were mixed. Therefore, this article has discussed potential strategies and approaches to improve the effectiveness of technology-based WLMIs.
This review provides important information to both patients and healthcare providers. Healthcare providers can suggest technology-based WLMIs to their patients and can include information about the strengths and weaknesses of each of the interventions. Moreover, suggested guidelines in this article can aid in planning further research design and implementation.
Further studies are needed to better evaluate the efficacy of technology-based WLMIs. Even longer maintenance intervention periods are needed to better evaluate the effectiveness of technology-based maintenance interventions. Moreover, this review included only eight studies; more primary studies are needed to evaluate reliable results. Meta-analysis also can be useful to examine actual body weight changes during the long-term period.
Footnotes
Acknowledgments
We would like to thank Dr. Diane Treat-Jacobson, Dr. Casey Hook, and Dr. Ulf Bronas for their generous support, feedback, and comments on this article.
Disclosure Statement
No competing financial interests exist.
Study Quality Coding Criteria
| TABLE HEADING | SCORING CRITERIA |
|---|---|
| Individual randomization | Were participants randomized to study conditions? If so, was randomization at the individual level? Stratified and blocked randomization is acceptable. Studies that used individual randomization combined with a small proportion of randomized matched pairs are considered Y. Appropriately designed and powered group randomization would also be acceptable if the group was also the unit of analysis. Individual randomization is N when the authors fail to mention randomization, specify that another method of assigning group status was used, or randomize at the group level and analyze at the individual level. |
| Control group | Did the study include a comparison group? The comparison group could be a no treatment as usual or an alternate treatment group. |
| Isolate technology | Did the study design allow for test of effectiveness of the technology (e.g., Web-based delivery versus no treatment)? To isolate the technology, the authors had to test the technology alone and compare with a group with no technology (Y). Packaged interventions where the technological components can't be parsed out are coded as not isolating the technology (N). |
| Pre-/posttest design | Was assessment of behavior completed preintervention and postintervention? |
| Retention | Was study retention at least 80% of the subjects who initially agreed to participate the study? Retention is calculated for the entire sample and not by group. For studies that did not report retention or dropout rates, retention can be calculated using the sample size used for analyses (e.g., 300 were randomized, but only 250 were included in analyses=83.3% retention). |
| Baseline group equivalent | Were tests conducted to determine if groups were equivalent at baseline in important variables (e.g., gender, age, weight)? If no tests mentioned, then UK. If subset of test indicated any group differences at baseline, then N. |
| Missing data | Were analyses conducted with consideration of missing data that maintain the fidelity of the randomization (e.g., intent-to-treat, imputation)? Listwise case deletion (completer analysis)=N if this was the only analysis conducted. If 100% retention, then completer analysis is appropriate=Y. If authors compared the “dropped subgroup” with the selected or randomized sample, but did not consider the impact of the dropped subgroup on randomization (e.g., intent-to-treat or imputation), then code as N. |
| Sample size calculation | Was power analysis reported to determine study sample size? |
| Validity of measures | Did description of measures include reliability and validity information? If reference or coefficients, then Y. If a well-established measure that is known to be validated was used, then Y. For objective measures without validity evidence, if the objective measure is used as a proxy (e.g., food receipt for nutrition intake), then N. If the objective measure is used as a direct measure of behavior (e.g., food receipts for food purchase), then Y. If validity not reported and measure unknown, then UK. |
| Total | Percentage of Y values (%) |
The study quality coding criteria were adapted from those of Norman et al. 8
N, no; UK, unclear/unknown; Y, yes.