
Abstract
Introduction
The American Telemedicine Association defines telemedicine as the use of medical information exchanged from one site to another via electronic communications to improve a patient's clinical health status. 1 There are telemedicine applications on electronic health (e-health), for example, teleconsultation between professional groups. However, some of the current telemedicine applications do not use the Internet. The World Health Organization defines e-health as the transfer of health resources and healthcare by electronic means. 2 Mobile health (m-health) can be defined simply as the use of wireless technology to deliver health services and information in mobile communication devices such as mobile phones, tablet computers, monitoring devices, smartphones, etc.
A review of the literature suggests that there is a lack of concrete evidence with which to fully assess the economic impact of telemedicine, e-health, and m-health systems. 3 There are several different costs associated with the development and implementation of these systems. Some of the costs, among others, are equipment costs, staffing costs, and communications costs. Two of the most common economic evaluation methods are cost-utility analysis (CUA) and cost-effectiveness analysis (CEA). CUA is used especially in health technology assessment. The main objective of CUA is to estimate the ratio between the cost of a health-related intervention and the benefit it produces in terms of the number of years lived in full health by the users. In health technology assessments, the benefits are usually expressed in quality-adjusted life years. 4 The National Institute for Health and Clinical Excellence defines quality-adjusted life years as a “measure of a person's length of life weighted by a valuation of their health-related quality of life.” The weights for quality-adjusted life years are derived by eliciting individuals' preferences for different states of health. 5
CEA, which is similar to CUA, is typically expressed in terms of a ratio where the denominator is a gain in health from a measure (for example, years of life) and the numerator is the cost associated with the health gain. 6,7 Nowadays, the introduction of new e-health and m-health technologies would substantially increase the cost-effectiveness of a healthcare system. 3 Most cost-effectiveness studies demonstrate that telemedicine can reduce costs. Some of these research works are analyzed in this article. The main objective is to review all studies in the literature of cost-utility and cost-effectiveness done for telemedicine, e-health, and m-health systems. For this, a search of related works is executed in several academic databases and systems such as PubMed, Scopus, ISI Web of Science, and IEEE Xplore.
Materials and Methods
A review of the published works related to cost-utility and cost-effectiveness in telemedicine, e-health, and m-health systems was developed and took place up to February 2014. The review was a literature study where different academic systems and databases were used. These systems were PubMed, IEEE Xplore, Scopus, and ISI Web of Science. Table 1 shows the search strategy used in this research.
Search Strategy
There were no limitations in publication date. Each related research study was obtained independently of the date of its publication. Figure 1 shows a flowchart with the steps followed in this review.

Flowchart of the steps followed in this review.
All the articles returned a total of 98 results, of which 63 were duplicated or with an irrelevant title for this research. The majority were duplicated. Of the remaining 35 articles, all resulted in relevant contributions.
Two requisites were considered for the inclusion of an article as relevant: the article must be written in English, and it has to involve a study of cost-utility and/or cost-effectiveness of e-health, m-health, and telemedicine systems.
The selection process of the articles was done by reading the titles and abstracts of the results obtained by one of the authors. A classification of the articles was obtained by reading their abstracts as well as the whole article when required. This study presents some limitations in the methodology followed for the review, which is typical in this type of review. 8
Results
As mentioned in Materials and Methods, in total, 35 relevant articles were found. Their publication dates spanned from 1998 to 2013, except for m-health, where there were no constraints in the dates. Figure 2 shows the percentage of studies published with respect to the research terms.

Percentage of studies found.
Figure 3 shows the number of results obtained for each search term in the different systems and databases. In total, 98 studies (see Fig. 1) were found, but 63 were duplicated or with an irrelevant title for this research. The final number was 35 articles. Figure 4 shows the number of articles versus publication date. Most of the studies are about cost-effectiveness in telemedicine. Some of the most relevant cost-utility and cost-effectiveness studies are briefly described in the following paragraphs.

Number of articles about cost-utility and cost-effectiveness in the literature using different scientific databases.
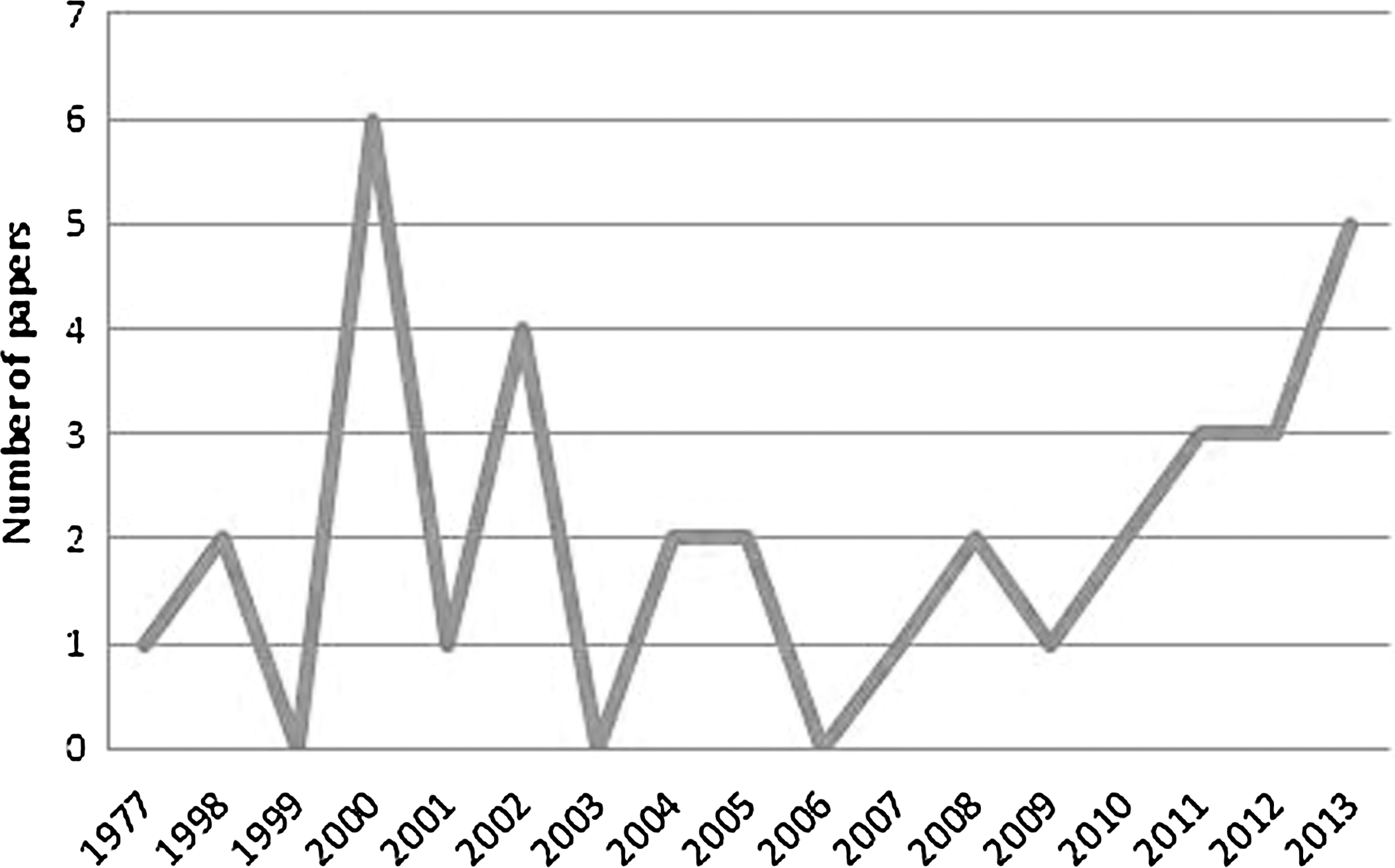
Number of articles in the review versus publication date.
Rachapelle et al. 9 studied the cost-utility of telemedicine in the screening of a telemedicine diabetic retinopathy screening program in rural Southern India that conducts one-off screening camps in villages. The Markov model was used, and they concluded that the results are dependent on the administrative costs of establishing and maintaining screening at regular intervals and on achieving sufficient coverage. 9 Lokkerbol et al. 10 presented the benefit-to-cost ratio of the current Dutch healthcare system for depression, and they investigated whether offering more online preventive interventions improves the cost-effectiveness overall. The conclusions indicate that for a healthcare system for depressive disorders to remain economically sustainable. 10 Mistry and Gardiner 11 showed that prenatal detection for congenital heart disease would be cost-effective using telemedicine screening. Naveršnik and Mrhar 12 examined the cost-effectiveness of the Improvehealth.eu service. A baseline model was used to evaluate the cost and effects of the intervention. The results show that e-health service was favorable because of the low cost and high efficacy of the intervention. 12
Franzini et al. 13 estimated the costs and cost-effectiveness of a telemedicine intensive care unit program. After this study, hospital administrators concluded that a tele-intensive care unit program aimed at the sickest patients is cost-effective. 13
Pyne et al. 14 examined the cost-effectiveness of a rural telemedicine-based collaborative care depression intervention. They concluded that it was effective but expensive. 14
Crow et al. 15 carried out a study to examine the cost-effectiveness of telemedicine delivery of cognitive behavioral therapy for bulimia nervosa. In this research work, cognitive behavioral therapy delivered face-to-face and via telemedicine was similarly effective, although telemedicine delivery cost substantially less. 15
Ehlers et al. 16 analyzed the budgetary impact and cost-effectiveness of the national use of thrombolysis with alteplase for acute ischemic stroke via telemedicine in Denmark. Jackson et al. 17 evaluated the cost-effectiveness of telemedicine and standard ophthalmoscopy for retinopathy of prematurity management. The results show that standard ophthalmoscopy for retinopathy of prematurity management and telemedicine are highly cost-effective compared with other healthcare interventions. 17
Bernal-Sánchez et al. 18 evaluated the cost-effectiveness of the Telemedicina Anáhuac project, which provides virtual satellite medical care via fixed teleconsultations and movable units in marginal and rural areas.
Hailey 19 indicated the importance of CEAs of telemedicine services. Johnston et al. 20 estimated the cost-effectiveness of the technology transfer teleophthalmology project in terms of a cost per disability-adjusted life year averted. The authors found the technology transfer project to be cost-effective in reducing the burden of eye disease. 20 Aoki et al. 21 conducted a CEA to investigate the clinical and economic impact of teleophthalmology in evaluating diabetic retinopathy in prison inmates with type 2 diabetes.
Agha et al. 22 studied the cost-effectiveness of outpatient pulmonary subspecialty consultations via telemedicine. They concluded that telemedicine is a cost-effective alternative for the delivery of outpatient pulmonary care for rural populations. 22
Stoloff et al. 23 studied the demand for telemedicine and the cost-effectiveness of various technologies such as telephone and fax, e-mail and Internet, video teleconferencing, teleradiology, and diagnostic instruments, as well as their bandwidth requirements for a shipboard telemedicine service.
Continuing with the bibliographic description, Ikonomidis et al. 24 analyzed the cost-effectiveness of telemedicine for remote diagnosis in congenital heart disease, and van Os-Medendorp et al. 25 showed the cost-effectiveness of an e-health system for patients with atopic dermatitis.
Smit et al. 26 proposed an alcohol model (ALCMOD) to estimate the cost-effectiveness of competing healthcare systems in curbing alcohol use in the Dutch healthcare system. Other authors studied the cost-effectiveness of a telemedicine intensive care unit program. 13 Heinen-Kammerer et al. 27 analyzed the cost-effectiveness of a system for the prevention of myocardial infarction, and Janssen et al. 28 did likewise for a telemedicine program for patients with chronic heart failure. Yang et al. 29 analyzed the cost-effectiveness of a pediatric critical care telemedicine program.
Bracale et al. 30 carried out the CEA for a Telemedicine—Islands project. As for cost-effectiveness studies about m-health services, Zurovac et al. 31 examined the cost-effectiveness of text-message reminders sent to health workers' mobile phones. They concluded that a simple text-messaging intervention improving health worker adherence to malaria guidelines is effective and inexpensive. 31
Discussion and Conclusions
In the systematic review different studies have been found. Several works dealt with cost-effectiveness in telemedicine systems for diabetic retinopathy screening. 9,17,21 The different cost-effectiveness studies demonstrated that teleophthalmology holds great promise for reducing the cost of inmate care and reducing blindness caused by diabetic retinopathy. Other studies concerned the cost-effectiveness of prenatal detection of congenital heart disease using telemedicine screening. 11 The benefits of telemedicine to rural communities and consumers are presented in the different studies. 14,22 The CEA for the Telemedicine—Islands project was done by Bracale et al., 30 rural telemedicine collaborative care intervention for depression by Pyne et al., 14 cognitive behavioral therapy for bulimia nervosa by Crow et al., 15 and telemedicine services for the delivery of outpatient pulmonary care for a rural population by Agha et al. 22
Many articles are reviews of cost-effectiveness studies of telemedicine systems and the importance of performing a good analysis. 32 –38 All reviews are from 1998 to 2002.
The economic impact of telemedicine is a collaborative and complex process in which different economic, social, and political actors can be involved. Most research studies in the literature have concluded that telemedicine systems are cost-effective; however, in this article, two studies have been found (Whitten et al. 39 and Mistry 40 ) in which the cost-effectiveness of telemedicine is not an explicit conclusion. 39,40 It might be concluded that there are too few articles about the cost-effectiveness of e-health and m-health systems in the literature.
Whitten et al. 39 indicated that there was no good evidence that telemedicine is a cost-effective means of delivering healthcare. 39 In this research work, the authors identified 55 articles that provided cost data on telemedicine interventions, and of these, only 24 stood up to a full review using an established instrument for assessing the quality of economic evaluations.
The vast majority of investigations are pragmatic assessments that add poorly to the knowledge concerning the costs and benefits of introducing telemedicine into the clinical practice. The authors make both a quantitative and a qualitative study. Most studies entirely equated benefits with cost savings, with no analysis of changes in benefit to patients.
Also, Mistry 40 identified 15 CEAs and 7 CUAs. In the results of her review there was no further conclusive evidence that telemedicine and telecare interventions are cost-effective as compared with conventional healthcare. 40 How can this be? The author indicates that some of the analyzed studies were pilot services, so that the costs and benefits may not reflect the true costs and benefits when the service comes into routine use. In many studies, indirect costs were often omitted. Moreover, most of the studies were for a period of less than 2 years. Other “matters” worthy of note in the conclusions of that research work were that the studies have small sample sizes and, moreover, that the costs were not compared with a baseline. This review work shows that telemedicine is a broad term, and if further reviews or analyses are undertaken, then they need to be categorized (real-time systems, store and forward, etc.). For this reason, the author assumed that it is unrealistic to attempt to make broad generalizations about the cost-effectiveness of telemedicine.
Some of the main limitations of the economic evaluations of the telemedicine, e-health, and m-health systems detailed are as follow: disparate estimation methods, lack of randomized control trials, lack of long-term evaluation studies, small sample sizes, and absence of quality data and appropriate measures.
With regard to the cost-effectiveness of m-health applications and services, there is only one study about the cost-effectiveness of mobile services before 1998. 41 One of the newest scientific works uses a health economic (Markov) model to synthesize clinical and economic evidence and to compute population-level costs and the effects of interventions. 10
At this point, it is noteworthy that one of the main limitations of this research work is that through scientific research it cannot be concluded with absolute certainty that there may not be many studies about the cost-utility and cost-effectiveness of e-health, m-health, and telemedicine systems because there are confidential studies carried out by private companies and different public health systems, which are not directly accessible to the public. In this work, the authors have often only considered the reviews published in the literature.
Future work will evaluate the cost-utility and cost-effectiveness of an m-health application for managing and educating patients with cardiopathies. Different scenarios will be proposed to analyze the cost-effectiveness and cost-utility of this application.
Footnotes
Acknowledgments
This research has been partially supported by the European Commission and the Ministry of Industry, Energy and Tourism under the project AAL-20125036 named “WetakeCare: ICT- based Solution for (Self-) Management of Daily Living.”
Disclosure Statement
No competing financial interests exist.