
Abstract
Introduction
Arterial hypertension is one of the most widespread diseases. Its prevalence is 50% in persons older than 60 years and 75% in persons suffering from obesity. 1,2 Arterial hypertension is the main risk factor for cardiovascular mortality. 3 One contributing factor is the fact that fewer than half of patients diagnosed with arterial hypertension are treated adequately, regardless of the antihypertensive medication used in treatment. 4
We have previously demonstrated that telemetric blood pressure (BP) measurement (TBPM)-adjusted BP treatment will lead to a better BP control after 3 months of intervention and that more patients will reach the recommended target BP. 5 In the control group only 36% of patients could achieve BP below 140/90 mm Hg, as in other BP trials. 2 Utilization of TBPM in the initial titration period proved even more advantageous for the stricter BP adjustment of high-risk patients (>125/75 mm Hg).
The continuous transfer of BP values to the treating physician enabled constant interaction with the patient when necessary. Positive effects by TBPM on BP treatment have been reported 6 –9 and have been explained by better adherence. 10 –12 Furthermore, it is assumed that a larger number of interventions, such as reminders to take medication or changes of medication, will result in a quicker and more accurate BP control in the TBPM group (TBPM-G).
These data indicate that TBPM is superior to a single 24-h BP measurement with regard to a quick and practicable titration of drug dosage until the BP target is achieved. Besides giving a higher confidence in the medical therapy, TBPM also helped in the identification of previously inadequately treated patients. It enables the physician to bridge the diagnostic gap, especially in the period of initial BP adjustment or change of therapy. TBPM seems to be as least as good as home measurements by the patient him- or herself, while avoiding known problems of incorrect documentation of data. 13
The initial 3-month interventional study did not assess the long-term effect of TBPM-guided BP treatment. This is done in the current analysis with an average follow-up of 20 months.
Portions of this study have been presented previously in abstract form in journal supplements or congress abstract books. 14 –17
Subjects and Methods
Sixty patients previously participated in a randomized, nonblinded, controlled intervention study. All patients included in the study were female and male whites from the region of the southern Lower Saxony. They were recruited from the hypertension outpatient clinic of the Nephrologic Center of Goettingen, Goettingen, Germany. During the intervention 3 patients dropped out. 5 Therefore, only 57 patients were eligible for the follow-up study. Of these, 17 patients were lost to follow-up as they did not want to participate or could not be contacted as they moved. Therefore, 40 patients with initial inadequately treated arterial hypertension (ambulant BP measurement [ABPM] controlled) were included in the final interpretation. Of these, 18 patients had received TBPM (TBPM-G) over the course of 3 months, whereas the control group received standard care (C-G) during the intervention period. Dropouts occurred because of relocation or a follow-up by primary care sites.
Interventional TBPM
Previously the TBPM-G patients were assigned to two subgroups with different alarm algorithms and BP target values depending on the risk profile (no risk profile [130/80 mm Hg in ABPM] versus suffering from diabetes mellitus or renal failure [125/75 mm Hg in ABPM]). The C-G patients received standard treatment such as the implementation of BP self-measurements and documentation of the values in a BP diary.
In addition, the experimental group in the previous study was supplied with a telemetry device (Stabil-O-Graph™; IEM GmbH, Stolberg, Germany) for the daily transfer of BP values measured at home to the treating physician. An alarm report was sent via e-mail to the physician (Fig. 1) if one of the alarm criteria for TBPM (Table 1) was met. In case of an insufficient BP control or noncompliance, the physician was able to counteract, for example, in the form of changing medication or intervention via phone. After 3 months a significantly better adjustment of BP was observed in ABPM of the experimental group 5 (Table 2).
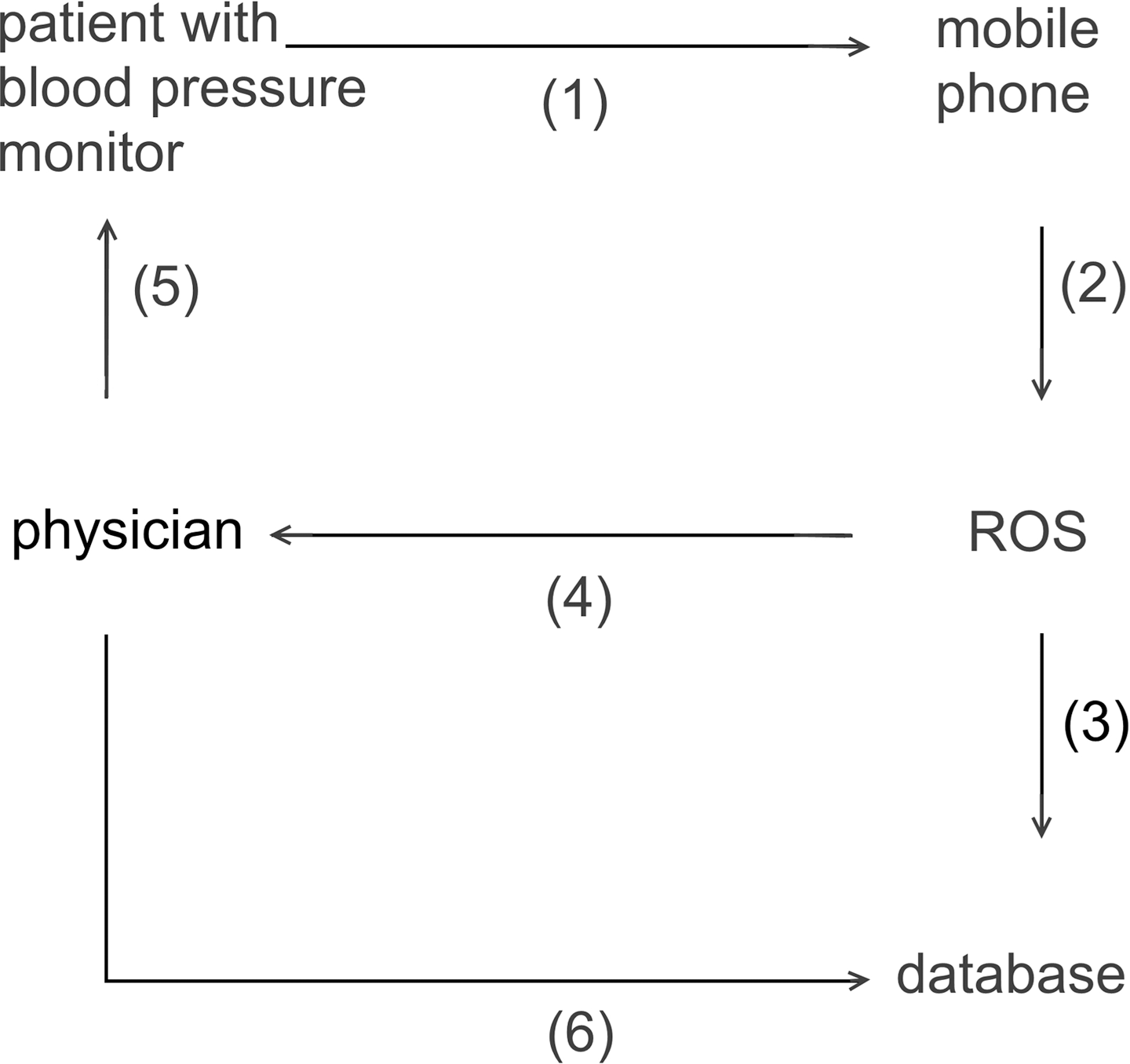
The concept of data management: (1) The blood pressure data from the patients were transmitted by the Stabi-o-graph via Bluetooth to the mobile phone; (2) the mobile phone sent the encrypted data via short message service to the remote operating system (ROS), and the ROS decoded the data and transmitted them to a central database; (4) if alarm criteria were met, an alarm report was sent via e-mail to the physician, (5) followed by contacting the patient by phone to resolve problems of compliance or existential orientation, as well as further steps in therapy; and (6) the physician was able to access the data and administer to the patient.
Alarm Criteria for Telemetric Blood Pressure Monitoring
This table is modified from that of Neumann et al. 5 Renal insufficiency was defined as an estimated glomerular filtration rate of <60 mL/min/1.73 m2 using the MDRD formula.
BP, blood pressure.
Results and Structural Overview of Study Groups over Time
ABPM, ambulant blood pressure measurement; ACE, angiotensin converting enzyme; C-G, standard-care control group; F, female; M, male; NA, not available; SD, standard deviation; TBPM-G, telemetric blood pressure measurement group.
Long-Term Follow-Up
In order to evaluate the long-term effects of BP treatment by TBPM, follow-up ABPMs of a subset of participants of the primary study were carried out on average 18 months after the end of the initial study. The patients were diagnosed again as part of a routine reappearance in the hypertension outpatient clinic of the Nephrologic Center of Goettingen by an ABPM.
The average BP values as well as achievement of the target BP values in the experimental and control group are compared with measurements taken at the start and end of the primary observation period, respectively.
After agreement of the local ethics committee to the amendment of the former study 5 and receipt of information and written consent of the patients, initially 60 persons with uncontrolled hypertension (ABPM according to European Society of Hypertension [ESH]/European Society of Cardiology [ESC] guidelines) of the hypertension outpatient clinic of the Nephrologic Center of Goettingen were included in the follow-up.
Statistics
For data interpretation we used Microsoft (Redmond, WA) Excel® (2002) and SSPS version 16 software (SPSS Inc., Chicago, IL). Levene's test was performed to evaluate homogeneity of variances. To test the significance of our results we applied chi-squared tests as well as paired and unpaired t tests. A two-tailed statistical power-calculation test of average was performed (91% at a confidence level of 5%). We assessed a p value below 0.05 as an indicator for significance. The examination was based on percentile distributions of BP values.
Results
At the start of this follow-up, 40 patients (TBPM-G, n=18; C-G, n=22) were available for examination ( Table 2 ). Their average number of practice consultations was 2.6±1.2 per year, whereas the recommended frequency was two per year for no-risk patients and four per year for patients with impaired renal function, respectively.
ABPM
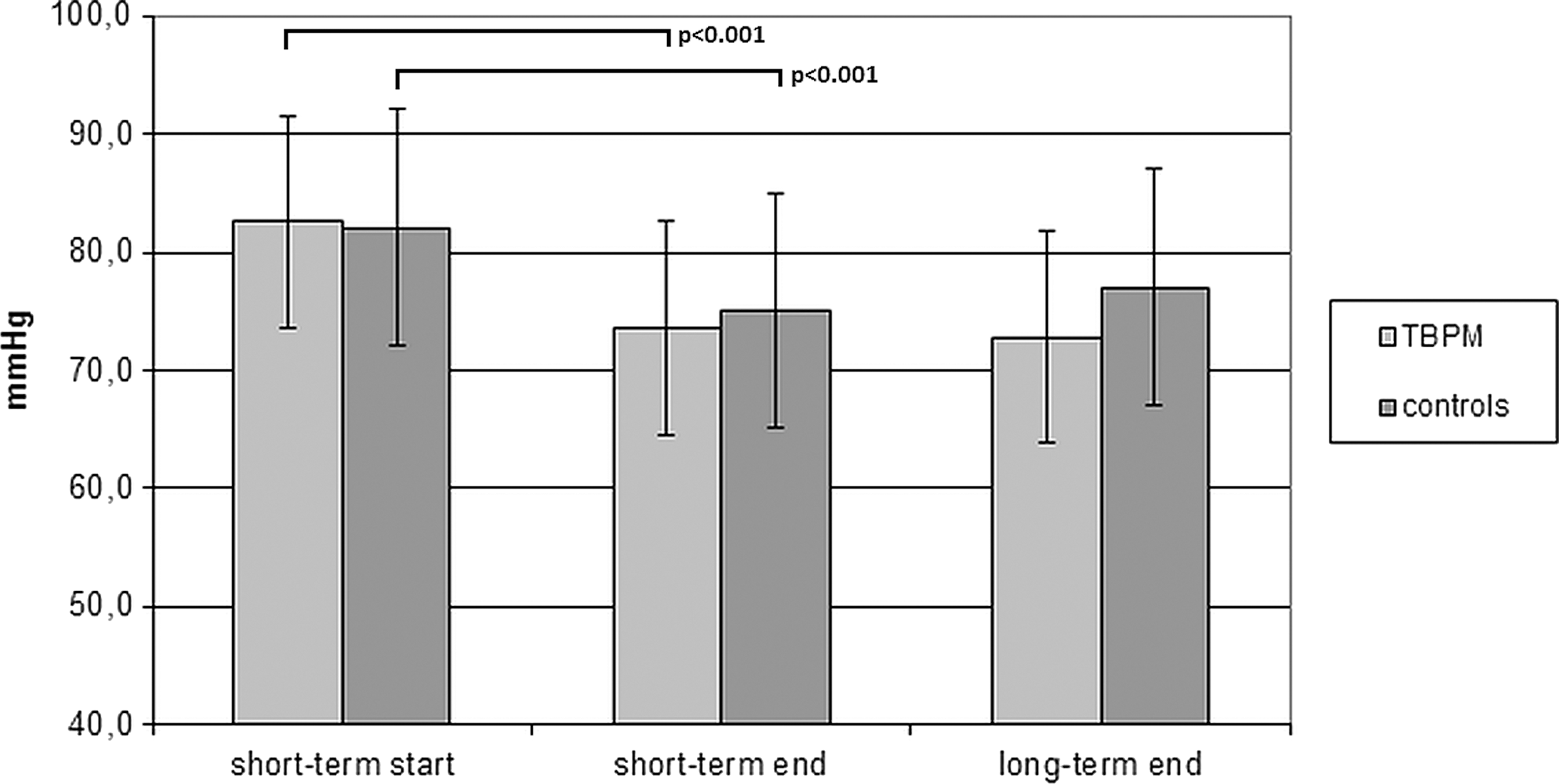
After an observation period of 3 months, with the help of a telemetry intervention in the TBPM-G, BP (systolic/diastolic) was decreased from 143.3±11.0/82.6±10.5 mm Hg to 126.5±6.5 (p<0.001)/73.6±7.3 (p<0.001) mm Hg. In controls, BP (systolic/diastolic) was decreased from 141.4±12.6/82.1±6.5 mm Hg to 131.6±11.8 (p<0.001)/75.1±8.2 (p<0.001) mm Hg. The differences amounted to −16.8 mm Hg (systolic)/−9.0 mm Hg (diastolic) in the experimental group and −9.8 mm Hg (systolic)/−7.0 mm Hg (diastolic) in controls (p=0.040 for systolic; p=0.356 for diastolic). 5
After an observation period of 617.7±139.0 days, on average, in the TBPM-G there was a further decrease of BP (systolic/diastolic) to 121.2±11.2 (p=0.175)/72.8±10.9 (p=0.474) mm Hg. In controls, there was a change to 130.7±10.4 (p=0.917)/77.0±7.1 (p=0.141) mm Hg after an observation period of 576.7±133.1 days on average (Figs. 2 and 3). Thus the respective changes in the experimental group and C-G were −4.1/−0.2 mm Hg (p=0.286) for systolic BP and −1.7/+2.1 mm Hg (p=0.356) for diastolic BP.

Effect of telemetric blood pressure measurement (TBPM) on ambulant blood pressure measurement, shown by differences between the control group and the TBPM group concerning the mean diastolic blood pressure during the short-term intervention period and after long-term follow-up.
Effect of telemetric blood pressure measurement (TBPM) on ambulant blood pressure measurement, shown by differences between the control group and the TBPM group concerning the mean systolic blood pressure during the short-term intervention period and after long-term follow-up.
BP Target Values
The defined target BP values were achieved by 54% (n=15) of the patients in the experimental group and by 36% (n=10) of the C-G patients (p=0.007, chi-squared test) after the initial 3-month period (Fig. 4). In subgroup 1 (BP target value of 130/80 mm Hg), 57% of the experimental group (n=8) and 46% (n=6) of the C-G achieved the required target value (p=0.120, chi-squared test). In subgroup 2 (BP target value of 125/ 75 mm Hg), only 19% (n=3) of the C-G and 50% (n=7) of the experimental group achieved the required target value (p<0.001, chi-squared test). 5
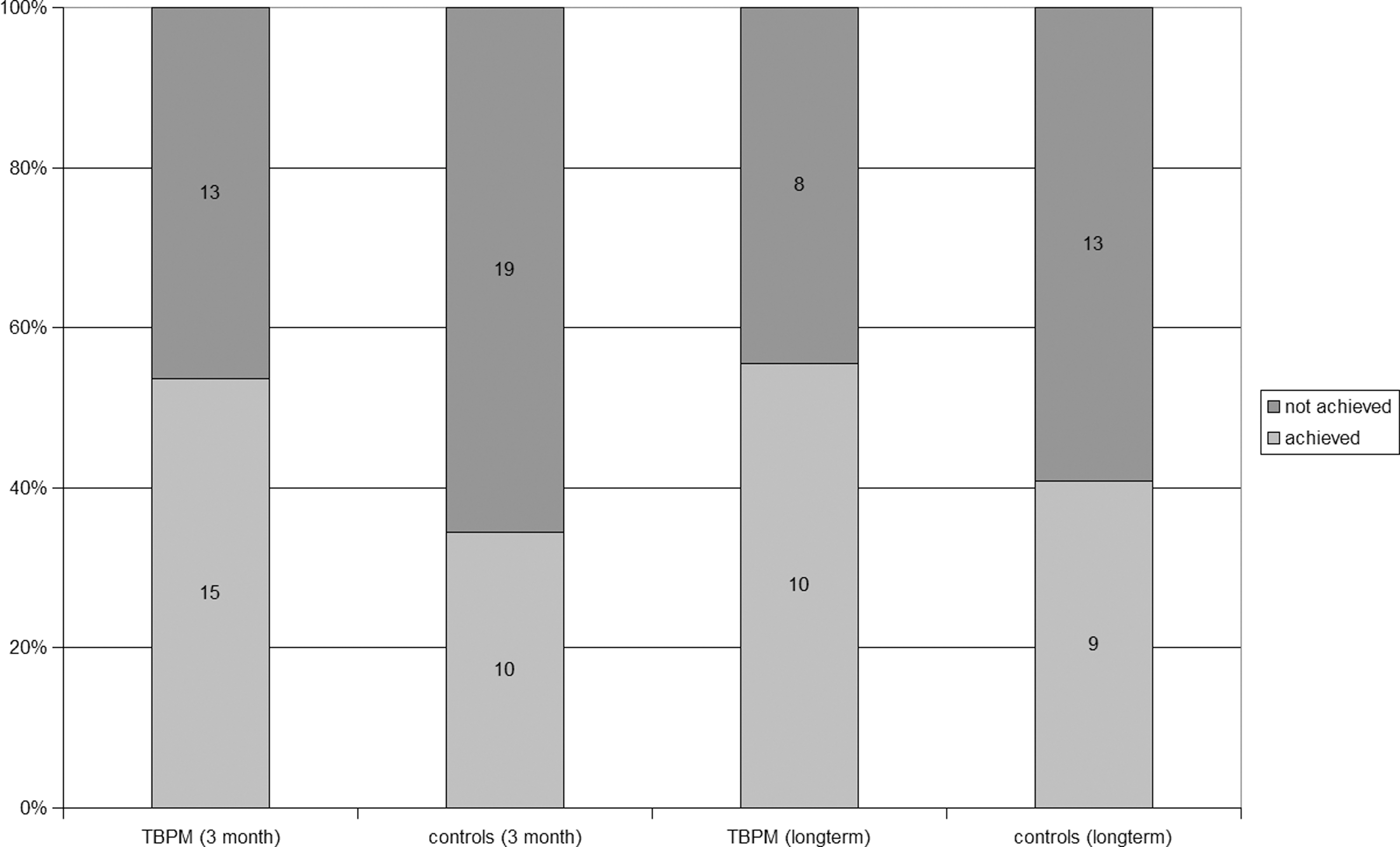
Final and follow-up by distribution of absolute numbers and percentages of achieved and not achieved blood pressure targets after 3 months and the long-term period in the telemetric blood pressure measurement (TBPM) group and controls.
After 617.7 and 576.7 days, 56% (n=10) of the experimental group and 40% (n=9) of the control group achieved the target value (p=0.024, chi-squared test) (Fig. 4). In subgroup 1 (BP target value of 130/80 mm Hg), 67% (n=6) of the experimental group and 50% of the C-G achieved the required target value (p=0.011, chi-squared test). In subgroup 2 (BP target value of 125/75 mm Hg), on the other hand, only 33% (n=4) of the C-G and 56% (n=5) of the experimental group achieved the required target value (p=0.001, chi-squared test).
Discussion
The use of telemetry is seen as a promising technique. 18 –20 Yet, long-term effects of telemetry methods have not been examined. 21 This study was able to demonstrate that the group with an initial TBPM-guided decision algorithm achieved a better long-term BP control, even after the TBPM intervention was stopped after the initial study period of 3 months. In patients with a BP target of <125/75 mm Hg, the rate was significantly lower than in a patient group with a BP target of <130/80 mm Hg, but the rate was always better in the TBPM-G. In the standard treatment group the rate was around 40%, whereas nearly 60% reached it in the TBPM-G. It is interesting that the BP achievement rate remained stable during the long-term follow-up period. The fact that BP values in both groups did not deteriorate might be explained by the compliance-supporting effect of taking part in a study. 5 Our data suggest that the failure to obtain high-quality ambulatory BP values will lead to a worse titration and individualized BP medication, which will lead to a long-term failure to achieve the recommended BP values. Thus, patient noncompliance is only one of the reasons why BP control is often not satisfactory; physicians' lack of knowledge of quality home BP readings is a second important reason. 22
In the present article, we show for the first time that in addition to immediate effects there is also a long-term effect of TBPM. This effect seems to be able to improve the treatment quality, which has remained static for 10 years on a quite similar level, depending on social economics and sequelae. 23 The positive outcome on long-term BP control can be explained by the optimized therapy adjustment in the titration period as well as to an increase of patient adherence during follow-up.
It has been shown that suboptimal adjustment of antihypertensive therapy (number of drugs and dose too low, combination therapy insufficient, stoppage of drugs due to side effects) nonadherence was the main problem in an effective hypertension therapy. 24,25 A good compliance is especially needed if three to four antihypertensives are needed to achieve the target BP value 26 –28 because an inverse relationship of the number of drugs and compliance has already been described. 29
TBPM can add to compliance to achieve an individually optimized treatment regimen because it involves the patient actively in his or her therapy even beyond its actual scope. Thus not only are monitoring and an optimized BP adjustment possible during the titration phase, but also a long-term modification of the patient's attitude toward his or her disease and an understanding of the necessity of an effective therapy seem to happen. These are important mainstays for fostering compliance. 30,31 It has already been shown in patients with heart failure that compliance improves when telemetry is used. 32 Furthermore there is a significant association among good compliance of a patient suffering from high BP, the resulting BP control, and the therapeutic outcome. 33
With regard to the effect of TBPM on long-term BP control, the requirements of the recent ESH/ESC guidelines, 34 and promising results of other studies, 8,9,35,36 we recommend the following procedure for management of hypertension: Initially a 24-h ABPM should be obtained 37 to assess the current BP control. If the result is not satisfactory, a 4-week optimization should be tried. If this does not lead to reaching the BP targets, an 8-week “interventional” telemetry should be carried out to optimize the BP medication to achieve the optimal control in this individual patient. 5 During follow-up, annual 24-h ABPMs should be carried out to assess the current BP control and to re-adjust the medication if necessary. According to the current ESH/ESC guidelines for self-measurement at home, 38,39 this procedure should be accompanied by self-measurements at home (measuring 1 whole week in 3 months).
In conclusion, our data suggest that telemetric assessment will lead not only to a better short-term BP control but also to a better long-term control. Whether these findings will also translate into a better outcome needs to be clarified in larger prospective studies. In addition, the cost-effectiveness needs to be analyzed. The latter is currently under investigation by the EDiMed (Assessment of the efficiency of service configurations in telemedicine), a national project supported by the Federal Ministry of Education and Research in cooperation with the University of Augsburg (Center for Performance Research & Analytics), the University of Goettingen (Professorship for Information Management), the University Medical Center Goettingen (Department of Medical Informatics), the University of Kassel (Department of Information Systems), the University of Bielefeld (Department of Health Economy and Health Management), and the Blutdruckinstitut Göttingen e.V. The collection of data on a larger sample of interventional TPBM patients is projected to be the subject of the ESH-affiliated BRAVE Foundation (Beneficence for research on arterial hypertension and vascular risk and education e.V.) at a European level in the near future as EUSTAR (European Society of Hypertension Telemedicine in Arterial Hypertension Register,
What is known about this Topic
• Far less than half of the diagnosed hypertensive patients are treated adequately and reach target BP values. 1
• TBPM enables a better BP monitoring than office BP in standard outpatient care in an ABPM controlled study design. 5
• This study's defined alarm criteria/algorithms proved to be practicable. 5
What this Study Adds
• A 3-month TBPM intervention results in a long-lasting effect on BP control.
• Based on ABPM, the difference between patients after TBPM and patients undergoing standard outpatient care remained unchanged after a total observation period of about 20 months.
Footnotes
Disclosure Statement
No competing financial interests exist.