
Abstract
Background and Introduction
The Veterans Health Administration (VHA) delivers healthcare services to 6.3 million Veterans annually. In fiscal year (FY) 2000, VHA, in caring for a Veteran population that is older, 1 sicker, 2 and poorer 2 than the general U.S. population, piloted a chronic disease management (CDM) program3 testing the hypothesis that care coordination, supplemented with home telehealth (HT) monitoring devices, reduces hospitalization of patients with high-prevalence chronic conditions (e.g., diabetes, heart failure, etc.). Modeled on the U.S. Institute of Medicine recommendations, 4 the pilot aimed to develop a program to expand non-institutional care 5 (NIC) to help Veterans age in place and to prevent avoidable nursing home (NH) admissions. VHA's enrollee projection model 6 had identified the need for VHA to expand NIC services 400% (to 101,301 patients) by FY 2012 (Fig. 1). Pilot testing was in Florida, southern areas of Georgia, and Puerto Rico, where large influxes of Veterans 7,8 were increasing the need for NIC services.

Projected number of Veterans with noninstitutional care needs, 2002–2011.
Patients selected on disease-specific criteria received HT devices and associated care coordination services. Care coordinators (nurses or social workers) reviewed risk-stratified, 9 asynchronously received HT data 10 (e.g., vital signs, symptoms, illness-promoting behaviors, and condition-specific knowledge deficiencies) in order to manage the care of “at-risk” patients, promulgate self-management, 11 and preempt crisis intervention. If patients acutely deteriorated, they accessed usual urgent care services (e.g., 911 or emergency room [ER]).
Evaluation in FY 20034 showed high patient satisfaction, 40% fewer ER visits, 63% fewer hospitalizations, 60% shorter hospital length of stay (LOS), 64% reduction of NH admissions, and 88% reduction of NH LOS. These results justified VHA's system-wide implementation of HT 12 that created its national care coordination HT (CCHT) program with a mission to make Veterans' homes their preferred site for care.
Assessment of activities of daily living 13 and instrumental activities of daily living, 14 using VHA's continuum of care form, categorized all CCHT patients according to complexity as NIC (CCHT-NIC), chronic care management, acute care management, or health promotion disease prevention. CCHT was standardized with development of (1) an operations manual, (2) training curriculum, (3) staff competency testing, (4) information technology platform, (5) clinical coding schema, and (6) quality management processes. 15 Over a 10-year period, CCHT patient numbers increased from 2,000 to 89,000 (Fig. 2) with CCHT programs in all 152 Veterans Administration medical centers.

Veterans Health Administration home telehealth census (point prevalence), 2003–2013.
Ongoing CCHT evaluations showed improved health-related quality of life, 16 reductions in unscheduled primary care visits, 17 50% fewer hospitalizations, 18 11% fewer ER visits, and LOS 17 shortened by 3 days and validated the efficacy of daily monitoring. 18 A retrospective 2008 VHA study 19 showed 19% fewer hospitalizations and LOS reductions of 25% for a cohort of 17,025 CCHT patients with 86% mean satisfaction scores and average annual costs for CCHT of $1,600 (versus in-home care of $13,121 or NH care of $77,745). Ongoing quality management data substantiate these findings.
Similar challenges and aspirations led other healthcare systems, 20,21 academic institutions, 22 and home care organizations 23 to evaluate HT. Systematic reviews found HT promising, yet unproven. 24 –29 Critiques of the VHA's 2008 study 19 included regression to the mean 30 and not accounting for concurrent Medicare 31 services. Randomized control trials (RCTs) of HT by the Mayo Clinic 32 and the United Kingdom's Whole System Demonstrator 33,34 (WSD) question HT's value for CDM. The Mayo and WSD studies show conflicting effects of HT on mortality (increased in the Mayo study and reduced in the WSD study). Determining whether HT is effective is critical for policymakers, 35,36 entrepreneurs, 37 clinicians, 38 and mobile health 39 proponents seeking scientific confirmation of its effectiveness. 40
Materials and Methods
In FY 2013, VHA reviewed FY 2009–FY 2012 administrative data (routine administrative data FY 2009–FY 2012 obtained from the VHA Allocation Resource Center [Bedford, MA] and VHA Support Services) and identified CCHT-NIC patients (n=26,751) and a matched cohort group (MCG) of 4,719,165 non-CCHT patients. Both cohorts were patients with complex chronic conditions (see Appendix) who were not receiving long-term institutional care services (e.g., NH care). All MCG patients were actively receiving VA healthcare services (vested), a component of which was in-home, support services as an indicator of their NIC status. Selection criteria for both cohorts are given in Tables 1 –3. This process yielded 4,999 CCHT NIC patients and a MCG of 183,872 non-CCHT patients for the comparative analyses.
Selection Criteria for Including Care Coordination Home Telehealth Patients in the Retrospective Analysis and the Resulting Numbers
Vested patients have been inpatients or had a comprehensive health exam in a Veterans Health Administration (VHA) facility in the past 3 years.
CCHT, care coordination home telehealth; FY, fiscal year; NIC, noninstitutional care.
Selection Criteria for the Matched Cohort Group for the Retrospective Analysis and the Resulting Numbers
Vested patients have been inpatients or had a comprehensive health examination in a Veterans Health Administration (VHA) facility in the past 3 years.
CCHT, care coordination home telehealth; FY, fiscal year.
Contrasted Selection Criteria for the Matched Cohort Group and the Care Coordination Home Telehealth–Noninstitutional Care Group at Fiscal Year 2009 Baseline
All statistical analyses were done using SAS software.
Vested patients have been inpatients or had a comprehensive health examination in a Veterans Health Administration facility in the past 3 years.
CCHT, care coordination home telehealth; FY, fiscal year; MCG, matched cohort group; NIC, noninstitutional care.
Comparative analyses were undertaken for outcomes for cost and healthcare utilization using the Statistical Analysis System (SAS) software program (SAS Institute, Cary, NC).
Results
Equivalence of CCHT-NIC and MCG at FY 2009 Baseline
Table 4 compares routine demographic, cost, and utilization data for CCHT-NIC and MCG patients for FY 2009 (i.e., the pre-CCHT enrollment baseline).
Comparison of Demographic and Healthcare Resource Utilization Data for the Matched Cohort Group and the Care Coordination Home Telehealth Group: 2009 Baseline Data
Data are mean (standard deviation) values.
CCHT, care coordination home telehealth; MCG, matched cohort group; NIC, noninstitutional care; VHA, Veterans Health Administration.
To address the standard deviations in these data relative to their mean values and to prevent outlier effects from skewing the pooled statistical analysis of mean CCHT-NIC and MCG variables, data were logarithmically transformed, giving a p value of 0.7, thus confirming the comparability of the two cohorts.
Comparative Outcomes of CCHT Patients Versus MCG in FY 2012
Table 5 gives cost and utilization data for CCHT-NIC and MCG patients in FY 2012 (following a minimum of 12 months of CCHT-NIC care).
2012 Comparison of Demographic and Resource Utilization Data Between the Matched Cohort Group and the Care Coordination Home Telehealth–Noninstitutional Care Group
Data are mean (standard deviation) values.
CCHT-NIC, care coordination home telehealth–noninstitutional care; MCG, matched cohort group.
To account for the standard deviations in these data relative to their mean values and to prevent outlier effects from skewing the pooled statistical analysis of mean CCHT-NIC and MCG variables, data were logarithmically transformed, giving a p value of 0.001 for the probability that the two groups differ.
Figures 3 –5 show changes in mean costs of care and other outcome data for CCHT-NIC and MCG for FY 2009–FY 2012.

Expenditures for care coordination home telehealth–noninstitutional care (CCHT-NIC) versus matched cohort group (MCG) for fiscal year (FY) 2009 and 2012.

Admissions for care coordination home telehealth–noninstitutional care (CCHT) versus matched cohort group (MCG) for fiscal year (FY) 2009 and 2012.
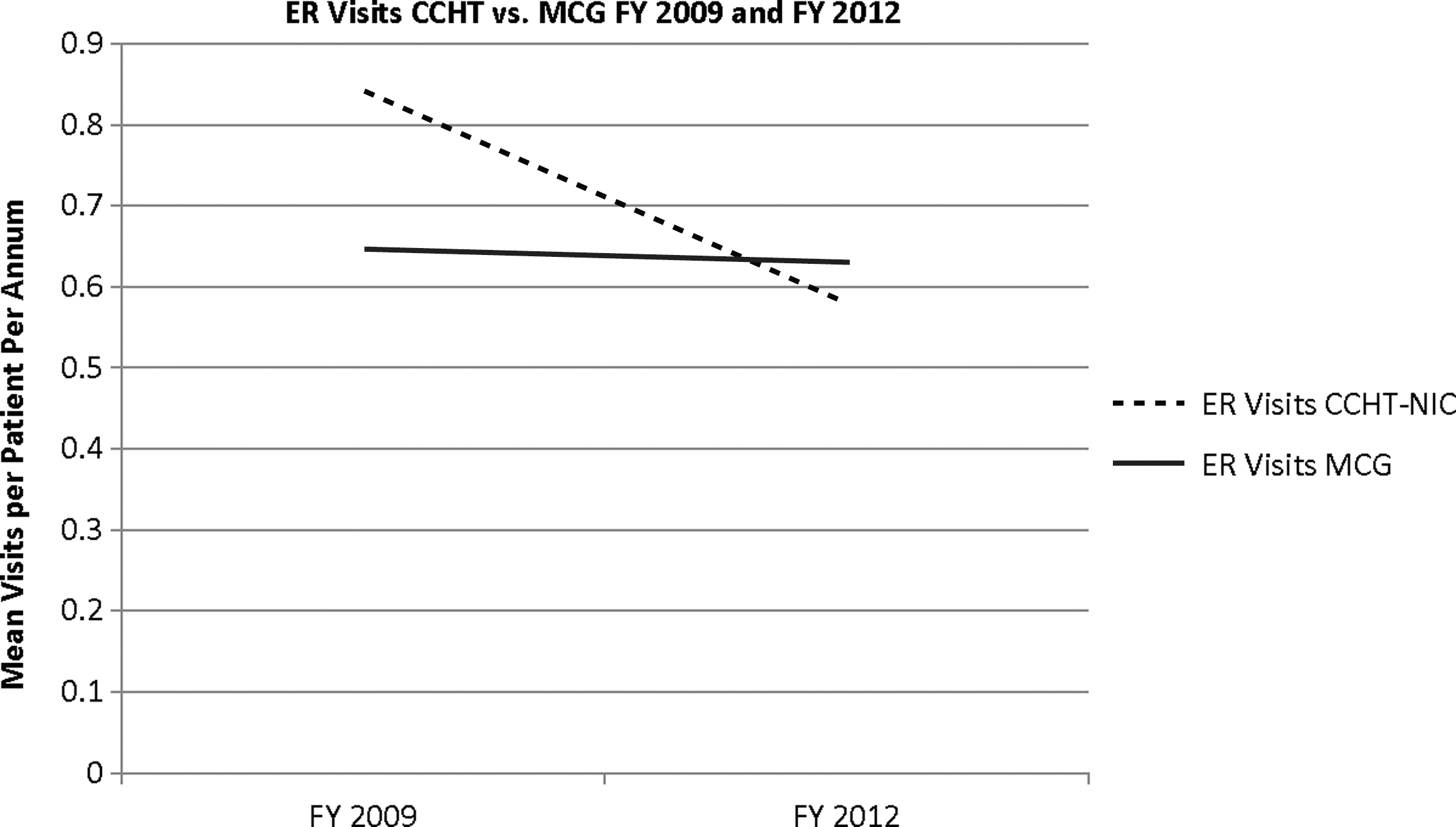
Emergency room (ER) visits for care coordination home telehealth–noninstitutional care (CCHT-NIC) versus matched cohort group (MCG) for fiscal year (FY) 2009 and 2012.
Discussion
In the current analysis, the CCHT-NIC group and the MCG had a p value of 0.7, thus confirming the comparability of the cost of the two cohorts at baseline in FY 2009. After CCHT care for ≥12 months, CCHT-NIC patients had significantly lower (p<0.001) healthcare costs; MCG patients' mean costs for care increased 48%, from $20,937 (FY 2009) to $31,055 (FY 2012), whereas the corresponding mean costs for CCHT-NIC patients' costs fell 4%, from $21,071 to $20,206. A range of associated cost drivers was examined but not statistically tested, including ER encounters, hospital admissions, and clinic visits. Average Medicare (Center for Medicare and Medicaid Services) costs for MCG patients at FY 2009 baseline were 66% more than for CCHT-NIC patients ($1,661) and increased 56% ($2,328) by FY 2012, whereas those for CCHT-NIC patients increased $1,078 (43%). Pharmacy costs rose by 22% ($470) over baseline for CCHT-NIC patients versus 15% for MCG patients ($326), a finding ascribed to improved medication management and improved compliance. These striking findings for HT intervention agree with previous findings for the same model of care. 19 In this case the matched cohort analysis reinforces the findings. It is possible that the MCG was not equivalent to the HT group, but the degree of matching at baseline makes this unlikely.
Final cohort selection criteria (see Tables 1 and 2) precluded direct mortality comparisons between the CCHT-NIC group and the MCG. In order to do a valid mortality comparison, the temporal criteria was eliminated (i.e., having care in FY12 and being enrolled for 12 months) which increased the CCHT-NIC cohort to 9,585 patients (Table 1) and the MCG cohort to 227,228 patients (Table 2). Using administrative data to calculate deaths within the two cohorts yields a mortality rate for CCHT patients receiving NIC of 9.8% versus 16.58% for similarly matched non-CCHT patients.
In itself, the current matched cohort analysis falls short of an RCT in assuring CCHT-NIC and MCG patients were identical at baseline. However, it offers significant assurance of their comparability. Outcome analyses using these cohorts to evaluate the CCHT-NIC group corroborate VHA's 2008 case report 19 findings and provide consistent evidence for HT's effectiveness, when used within VHA's CCHT-NIC model of care. Such positive findings raise questions about why systematic reviews of HT 24 –28 in VHA are equivocal and recent RCTs of HT are negative. VHA's current analysis excludes regression to the mean and concurrent Medicare usage as possible reasons, leaving (1) different study populations, (2) different care models, (3) electronic health record (EHR) usage, (4) nonstandardized/inconsistent care models, (5) different/inadequate evaluation methodologies, and (6) influences from the overarching healthcare system, as other explanations.
Mayo and WSD populations appreciably differ from CCHT-NIC patients. In the Mayo study, patients were frail elderly—on average, 14 years older than CCHT-NIC patients. WSD did not specify the demographics or medical diagnoses of its study population, but including cognitively impaired patients suggests some were elders. VHA would have provided the Mayo study patients, 41 ones specifically excluded from this current VHA analysis, with supplemental healthcare services (e.g., home-based primary care 42 ).
Asynchronous symptom and biometric assessments in the Mayo study with referral of acute events to 911 or an ER corresponded with CCHT-NIC, but timely outpatient visits, nurse-generated after-discharge phone calls, and access to phone nursing and urgent clinic/ER visits for control patients as the sole intervention for their HT population were likely insufficient. The WSD study's HT interventions varied but were based on asynchronous review of vital signs/symptoms by primary care clinicians and included self-management and health education, suggesting the WSD model broadly aligned with CCHT-NIC. However, the specifics of what the Mayo and WSD studies meant by vital sign monitoring, self-management, and their health education processes were unclear beyond using HT technologies. Mayo's physician-led medical care team and WSD's unspecified clinical support may represent a “medical model” 43 of care (i.e., technical adviser) approaches. If so, these contrast with the VHA's program, 3 which uses a biopsychosocial 44 model in which CCHT care coordinators give more than technical advice. VHA learned the importance of this distinction in FY 2006–FY 2007 when a legacy CCHT program (having a medical model approach) had 40% greater utilization (unpublished VHA data), and, once identified, this program converted to the standardized model with similarly consistent outcomes.
CCHT-NIC uses VHA's integrated EHR that provides information 45 supporting interdisciplinary clinical decision-making. 46 Mayo and WSD studies and systematic reviews of HT do not detail EHR usage and its operation across the continuum of care. Care coordination, information technology, and quality management tools (elements of VHA's CCHT program) are well described, 15 and they reduce mortality and hospitalizations in CDM. 47 CDM patients usually have several volumes of written charts, often inaccessible while the individuals are in transit between sites of frequent clinic visits and hospital admissions. CDM patients often have multiple comorbidities, and, in VHA's experience, HT monitoring data alone are insufficient to deliver CCHT-NIC effectively. An EHR and its access to history, progress notes, medications, lab results, etc., are needed. Isolated HT monitoring data promote reactive decision-making.
CCHT-NIC provides routine national services that have benefited from the economies of scale, 48 process re-engineering, 49 associated training/quality management processes, 50 financial allocation systems, 51 and consistency arising from 10-year standardization of its clinical, technology, and business processes. Possible inconsistency of the Mayo program and the 397 practice sites assessed by WSD make these clinical models unclear and subject to variations due to setup and program development.
Data collection instruments and evaluation methodologies differ in all published HT studies. For example, the Mayo Clinic and WSD evaluations were research studies, whereas CCHT-NIC is an ongoing evaluation of a mature self-sustaining program. Patient populations, models of care for HT, and organizational reasons to evaluate HT are different for VHA's CCHT-NIC and both the Mayo and WSD programs. As a result, evaluation strategies and methodologies were necessarily different. Although theoretically of superior methodology, the Mayo Clinic and the WSD studies (RCTs) were not free from bias (e.g., neither patients nor controls were blinded to the intervention). In contrast, systematic studies of HT are confounded by questionable methodologies. 52
The VHA implemented CCHT-NIC in a U.S. federal government healthcare system, the Mayo Clinic is a not-for-profit medical practice, and the WSD was within the United Kingdom's National Health Service. Each has a different culture, mission, patient population, care delivery system, and reimbursement mechanism. These noncomparable settings and varied implementation may, in part, account for the contradictory outcomes.
Conclusions
VHA's routine use of HT has been successful in coordinating the care and more efficiently managing patients with complex chronic conditions—ones whom healthcare systems delivering services to rapidly aging populations with multiple comorbidities are challenged to serve. VHA's model of CCHT supplements traditional ambulatory care using an innovative CDM model and results in significantly reduced healthcare utilization. VHA's consistent demonstration of these benefits is at variance with the findings of other national/international healthcare systems whose evaluations of HT show equivocal or negative impacts. Reasons for these inconsistent experiences are variations in the populations treated, models of care adopted, EHR use, standardization/consistency of care models, evaluation methodologies, and implementation in dissimilar healthcare systems. In determining the efficacy of HT, it is important to move beyond fixation on the technology. HT implementations must be placed within the context of a care model that coordinates care to improve population healthcare, and demonstrably links the necessary healthcare assets to do so, across the continuum of care. Resolving whether HT is effective in CDM is of critical importance. In the VHA, CCHT mitigates the effect an increasing prevalence of chronic disease is having on healthcare costs and allows people to remain living independently in their own homes and local communities who would otherwise need long-term institutional care, whereas many other organizations are hesitant to adopt this healthcare innovation and realize these benefits.
Footnotes
Disclosure Statement
No competing financial interests exist.
S.K. and M.Y. had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Appendix: Chronic Disease Criteria Used for Patient Selection in the Matched Cohort Group and Home Telehealth Groups
| CHRONIC CONDITION |
|---|
| Arthritis |
| Congestive heart failure |
| Chronic obstructive pulmonary disease |
| Dementia |
| Diabetes |
| End-stage renal disease |
| Human immunodeficiency virus |
| Hypertension |
| Ischemic heart disease |
| Multiple sclerosis |
| Mood disorders |
| Posttraumatic stress disorder |
| Paralytic disease |
| Schizophrenia |