
Abstract
Introduction
Diabetes is at epidemic levels and now impacting 29.1 million individuals in the United States. 1 Type 2 diabetes (T2D), characterized by insulin resistance and insulin insufficiency, is the predominant form of diabetes (90–95% of cases) and is linked to obesity, aging, and individual genetic vulnerability. 2 Landmark studies of T2D have demonstrated significant clinical benefit from intensive management of elevated blood glucose (BG), blood pressure (BP), and blood lipids. 3 –5 However, there is a significant gap between evidence-based recommendations for T2D and the medical care currently delivered. Only 19% of diabetes patients in the United States meet recommended goals: hemoglobin A1c (HbA1c)<7%, BP<130/80 mm Hg, and low-density lipoprotein<100 mg/dL. 6
The percentage of patients receiving recommended annual screenings for early detection of diabetes-related changes in the eyes, kidneys, and feet also remains suboptimal. 1 From the patient's perspective, T2D is a complex and demanding chronic illness. Patients must initiate or modify many daily lifestyle behaviors to benefit from the treatment plan, including physical activity, eating, medication taking, monitoring of BG and BP, problem solving (especially for BG for high and low levels and during sick days), reduce risks of diabetes complications, and develop coping skills. Diabetes self-management education, delivered in individual or group outpatient sessions, is the cornerstone of clinical support for behavior change. 7
Scalable, population-based healthcare models are urgently needed to meet the growing public health challenge of T2D. 8 These models should incorporate a team approach and care delivery strategies such as telehealth with a focus on daily patient self-management support and early detection of avoidable medical complications and crises. 9,10 Nurse-led telehealth has emerged as a patient-centered strategy for the delivery of diabetes self-management education that leverages communication and information technologies to provide more timely and convenient support in the patient's home. 11 Remote home monitoring (RHM) for T2D typically involves regular BG and BP tracking to provide reminders, alerts, and feedback to the patient and support daily self-management behaviors. 12 Brief outbound nurse calls are often provided in response to device alerts, to provide targeted self-management education, and to coordinate referrals into clinic services. Diabetes telehealth interventions have been shown to successfully augment traditional face-to-face care and significantly improve BG control (e.g., a clinically relevant 0.5% HbA1c drop over 6 months). 13 Furthermore, we recently reported that a long-standing “virtual diabetes nurse” program for urban poor Medicaid T2D patients that was reimbursed by the hospital's own health plan and was co-managed with the patient's own provider reduced HbA1c by 1.8%. 12
In this pilot study, we evaluated the benefit of adding a cellular pillbox (i.e., the MedMinder™ [MedMinder, Needham, MA]) to an existing BG meter and BP cuff device suite as part of a nurse-led telehealth model, focusing on device usability, program satisfaction, and clinical benefit. User-friendly cellular pillbox technologies such as the MedMinder are now widely available and may improve patient medication adherence and telehealth program outcomes. Cellular pillboxes provide automatic data upload via a cellular communications network to the “cloud.” They provide the patient with daily organization of pills, adherence reminders, and feedback on adherence patterns, and provide clinicians with alerts and clinical decision support (CDS) summaries to inform treatment decisions.
Materials and Methods
We used a single sample, pre–post study design. We targeted poorly controlled T2D patients seen at a local community health center. The clinic is located in a medically underserved, urban neighborhood where the mean annual family income is less than $20,000. The clinic includes a diverse population of ethnic and socioeconomic groups (45% Hispanic, 25% white, 25% African American, and 5% other). The clinic population comprises Medicaid 67%, Medicare 24%, commercial insured 8%, and self-pay insured 1%. Study eligibility included the following: being a T2D patient seen within the previous 12 months at the clinic, not on multiple daily insulin therapy, HbA1c level between 7% and 11% at baseline, age >50 years, no serious psychiatric or medical health complications present, English speaking, and the patient's provider approves his or her participation in the program. The study was approved by the Institutional Review Board at our institution.
The Diabetes Telehealth Program
Each patient enrolled in this study received three monitoring devices (BG monitor, automatic BP cuff, and MedMinder pillbox), all marketed by Ideal Life® (Toronto, ON, Canada). We incorporated these devices into a program designed to involve minimal burden to clinical nurse care coordinators (i.e., only 4 h of involvement per week in total as well as minimal clinician training) that functioned as a nonurgent service to complement usual medical care.
The role of the two clinical nurse care coordinators (RNs), here referred to as nurse interventionists, was to make three brief, scheduled outbound calls to study participants at Weeks 2, 4, and 8 of the 3-month program and to respond to incoming RHM alerts as needed throughout the program. The nurse interventionists worked with a supervising physician (A.B.) who served in a liaison role with the primary care providers of participating patients. Providers received an RHM report for each of their patients enrolled in the study at the end of the program. This report summarized BG and BP excursions (Fig. 1), as well as weekly medication adherence (percentage of prescribed medication cup doses taken each week), summarized in a calendar-style format along with a summary index (from 0 to 100) for medication adherence achieved (Fig. 2). Telehealth nurses were instructed to handle incoming RHM device alerts using standard clinic triage procedures for confirmed high readings. RHM alerts could, if judged by the nurse to be significant, trigger an outbound call to the patient to check that the reading was accurate (and ask the patient to repeat the measurement) or to arrange for a provider visit, additional services, or use of the emergency services, as needed.
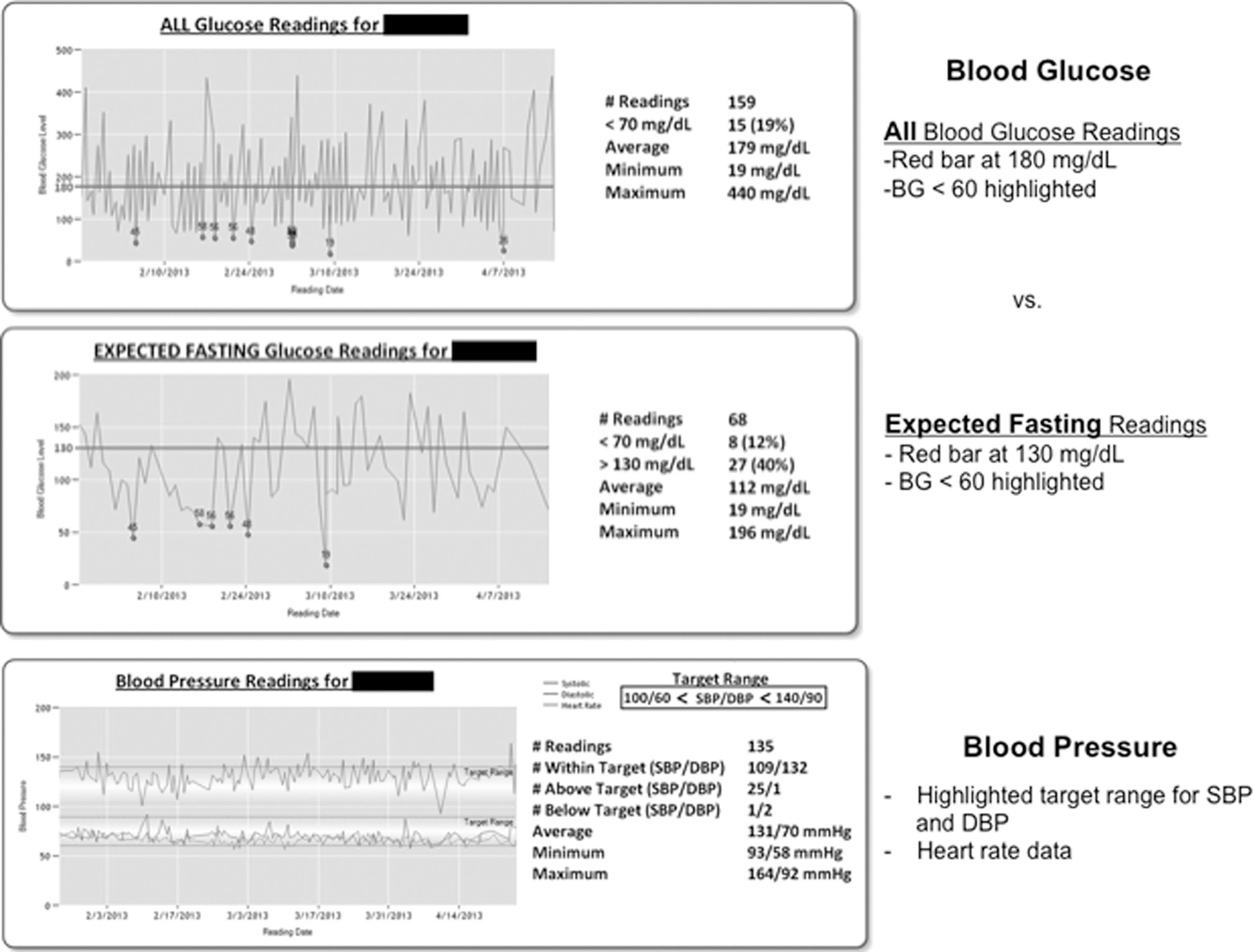
Example of a clinical decision support report for providers, showing blood glucose (BG) and blood pressure testing results over 3 months for a study participant. DBP, diastolic blood pressure; SBP, systolic blood pressure.

Example of a clinical decision support report for providers, showing medication (med) adherence results over 3 months for a study participant.
Device readings were uploaded automatically from the devices to a secure vendor Web site, and the data were then pushed to an existing “diabetes dashboard” CDS application 14 that was used to access the device alerts and summary reports.
Procedures and Assessments
At baseline and 3-month follow-up research visits, a nurse research coordinator obtained informed consent, taught the patient to use the RHM devices, performed a point-of-care HbA1c test (DCA 2000™; Siemens Corp., Washington, DC), guided the patient through the study questionnaires, and measured vital signs (weight, height, BP). A review of each patient's medication list was generated from the electronic medical record and baseline patient interview to set up the MedMinder pillbox with medications to manage hyperglycemia, hypertension, and dyslipidemia for up to four daily dosing times. A research technician used the secure vendor Web site to set up RHM device assignments and alert settings. Study patients were requested to conduct a minimum of one daily fasting BG reading (or more frequent testing if instructed by their provider), take a BP reading at least three times per week, and take medication doses daily within 2 h of the patient's preferred dosing start time (e.g., 7 a.m.–9 a.m. for a morning medication dose).
The following “high-risk” alert settings were used for the RHM devices based on provider discussion and consensus: hypoglycemia, BG <60 mg/dL; hypertension, systolic BP >200 mm Hg; hypotension, systolic BP <80 mm Hg; low BG meter device use, no data for >2 days in a row; low BP meter device use, no data for >7 days in a row; and low pillbox device use, no data for >2 days in a row.
Within a week of enrolling a patient, a research technician called the patient at home to ensure competency in using the devices, proper device setup with successful transmission of data to the clinical team, implementation of device use guidelines, adjustment of pillbox dosing times/schedule if necessary, and response to device-related questions and to provide a reminder that the patient would hear from a telehealth nurse by telephone within 2 weeks for the first outbound telehealth support call. At the 3-month follow-up, patients completed questionnaires assessing usability and satisfaction with the telehealth program using a 5-point Likert scale (“disagree strongly” to “agree strongly”). Similar questionnaires were given to the nurse interventionists and participating clinic providers.
Results
Of the 107 patients eligible for this study, 64 were not reachable by phone or did not wish to participate (Fig. 3). Eligible enrolled versus nonenrolled patients did not differ by age (60.4±7.0 years versus 62.8±6.3 years, p=0.10) or gender (46.7% female versus 51.5% female, p=0.83).

CONSORT flowchart showing study recruitment and patient engagement.
There was a very high retention rate for those enrolled, with 29 of 30 completing the study (96.6% completion rate). The mean age of the study population was 60.6 years, 73% were African American and 26% were Hispanic, 56.7% had a high school education or higher, and 33.3% were employed (Table 1). Mean HbA1c level was 8.3%, and mean body mass index was in the obese range (31.8 kg/m2). There was an average of 2.14±0.45 daily oral agent medication doses per dispensed pillbox. The majority of pillboxes (n=22) were configured with twice-daily medication doses (morning, evening), five were configured with three daily dosing times (morning, midday, evening), and one was configured with one daily dose. The doses contained an average of 1.9 medications per dosing time, with a range of one to four oral medications. Results showed (based on patient self-report) that 55.2% of patients placed their RHM devices in the bedroom, 10.3% in the dining room, 10.3% in the kitchen, 10.3% in the living room, and 13.8% in other places.
Baseline Characteristics of Diabetes Telehealth Patient Population (n=30)
Data are mean±standard deviation values or number of patients (%) as indicated.
In total, 78 alerts (2.6 per patient on average) were generated from the RHM devices over 3 months (n=72 for BG <60 mg/dL and n=6 for BP >200 mm Hg). Only five (6.4%) of these alerts required an additional, unscheduled outbound telephone call from one of the nurse interventionists. Many alerts were considered by the study nurses to be clinically unremarkable and thus did not warrant an outbound call to the patient (typically several days after the event) when normal readings were subsequently seen in the charts based on more recently uploaded RHM data.
Use of the BG meter and BP cuff was required in our study protocol, but although use of the pillbox was encouraged at the baseline research intake visit, it was not presented to the patient as mandatory for participation in the study. However, the majority of patients (93.3%) agreed to take the pillbox home. Two patients who refused the pillbox commented that they already had a standard (nonelectric) plastic pillbox at home and that switching to the “nonportable” MedMinder device was incompatible with their work/living schedule (i.e., shift work). However, these 2 patients did agree to take home the BG meter and BP cuff and to receive scheduled nurse calls and were retained in the study. Of the 28 pillboxes that were taken home, five (17.9%) were discontinued by the patient for several identified reasons: concern about the safety and children in the house having access to their medications (i.e., fears from using an unlockable pillbox), early patient exclusion from the study, and inability of the patient to align his or her work/life schedule with the available pillbox dosing times (i.e., morning, lunchtime, evening, bedtime).
Overall, the RHM device use data showed a pattern of consistent and high use of the three devices over the 3-month program. Patients with hypertension were expected to test BP levels at least three times a week, and this was exceeded for all 12 weeks, with a range from 4.9 to 6.3 (Fig. 4). Patients were instructed to test BG daily, and this criterion was met for all 12 weeks of the program, with a mean weekly frequency ranging from 7.0 to 9.3 (Fig. 5). The average medication adherence using the pillbox (calculated each week as the number of pillbox bins opened each day divided by the total number of bins prescribed to be opened) was above 80% from Week 2 to Week 12 and was above 90% for a brief window from Week 3 to Week 5 (Fig. 6).
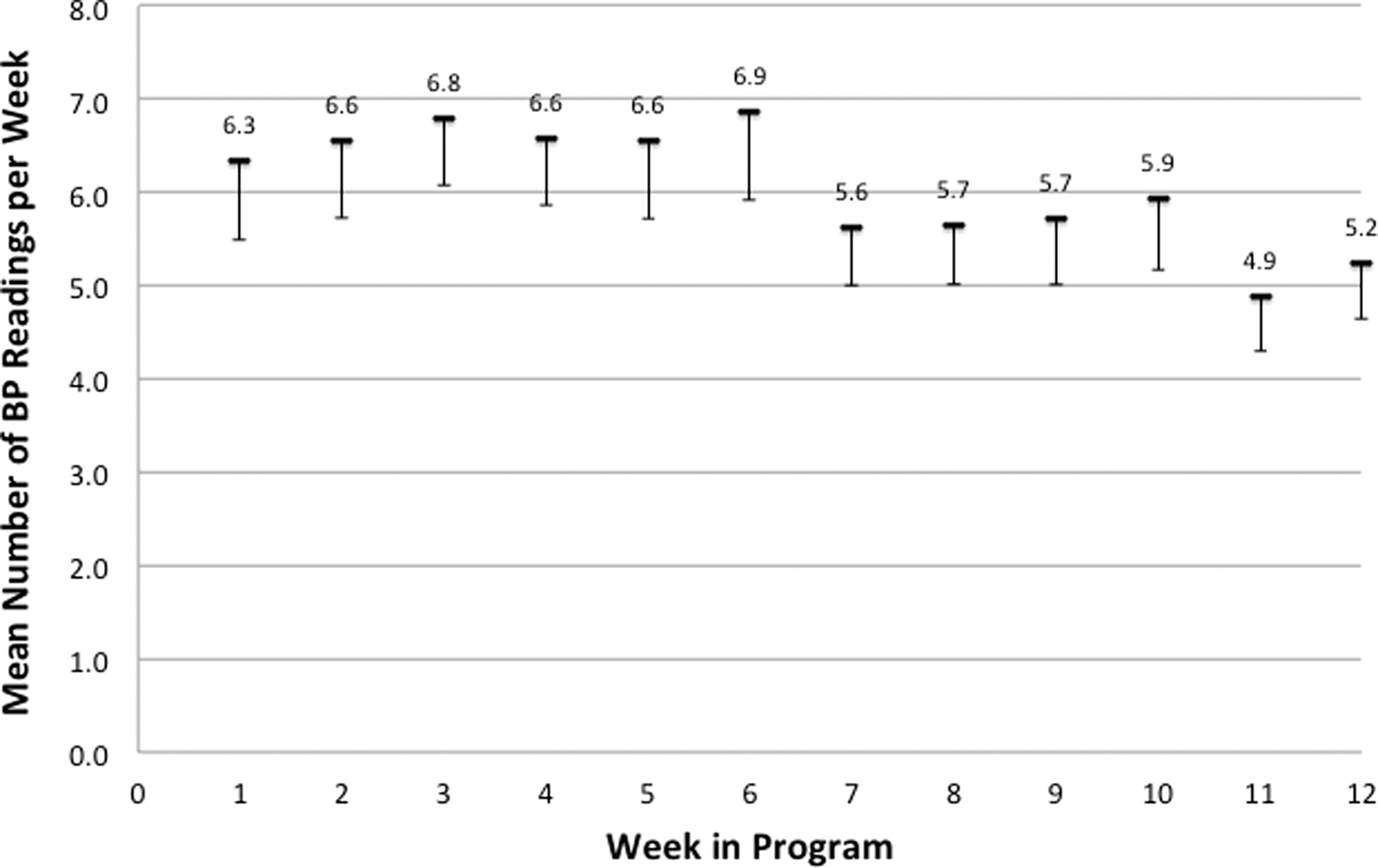
Mean weekly blood pressure (BP) testing over 3 months for participants enrolled in the diabetes telehealth program.
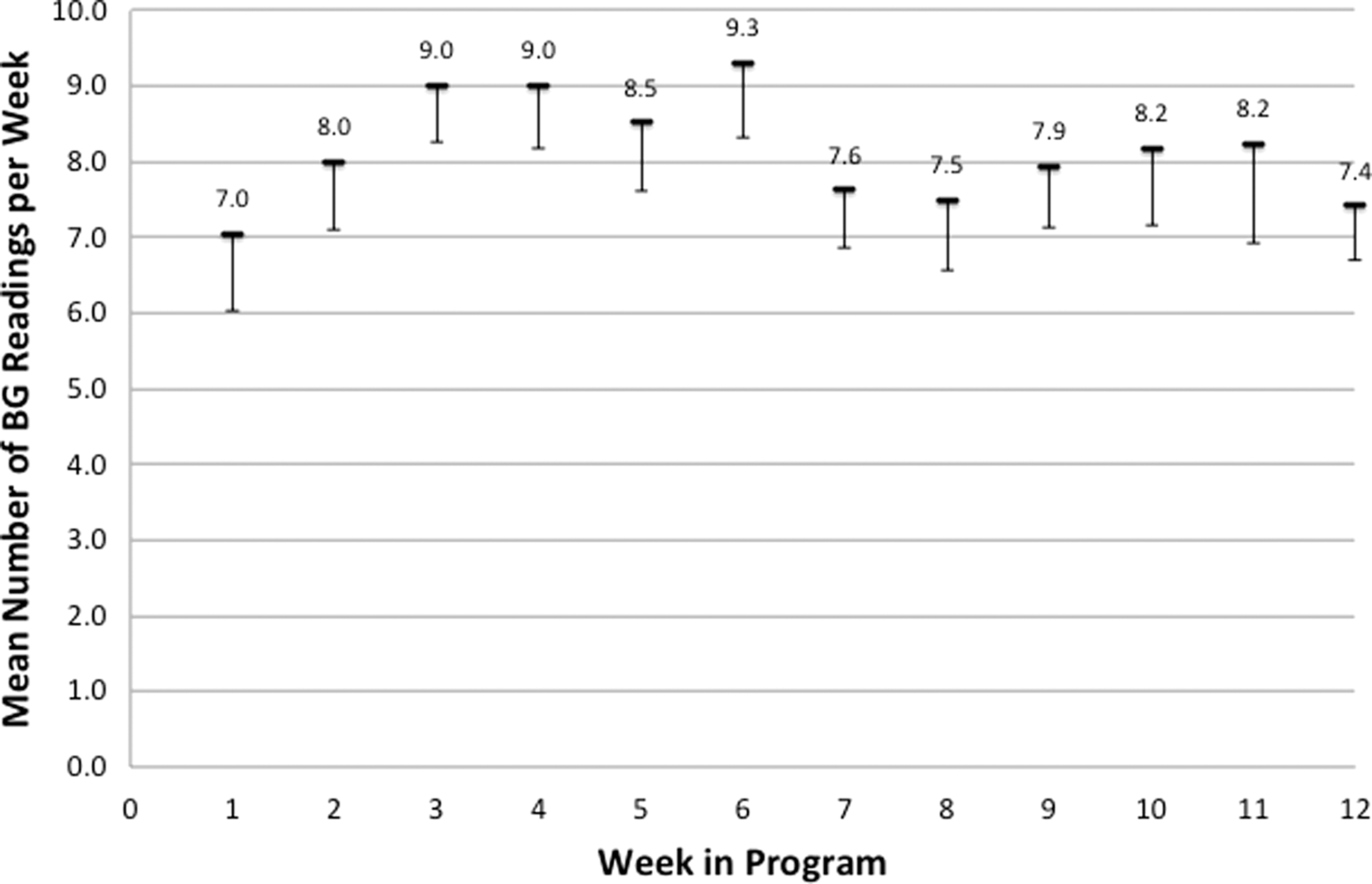
Mean weekly blood glucose (BG) testing over 3 months for participants enrolled in the diabetes telehealth program.

Mean weekly medication adherence over 3 months for participants enrolled in the diabetes telehealth program.
Patient ratings of pillbox ease of use, helpfulness in organizing medications, ability to fit into routines, convenience of the location of pillbox in the home, and ease of refilling were almost all (i.e., 90%) given as “strongly agree” (Table 2). Similar positive ratings were consistently found for the BG meter and BP cuff (88.8% and 84%, respectively, were “strongly agree”). Patient satisfaction ratings with the telehealth program were strongly loaded toward “strongly agree” and “somewhat agree” for items assessing happiness with device training and feelings of support from diabetes team, and all patients reported they would either “strongly agree” (n=25) or “somewhat agree” (n=4) that they would recommend the program to other T2D patients based on their experience (Table 3).
Patient Feedback on Remote Home Monitoring Device Usability (n=29)
BP, blood pressure.
Patient Satisfaction with the Diabetes Telehealth Program
RHM, remote home monitoring; T2D, type 2 diabetes.
The majority of the 11 participating clinic providers endorsed that they “strongly agreed” that the CDS report summarizing BG values, BP values, and medication adherence was clear and easy to understand (Table 4). All providers wanted these reports to be made available in future within the hospital system's electronic medical record, and 8 of the 11 providers (72%) reported they “strongly agreed” that hard copy (paper) reports were also wanted. Study nurse interventionists tended to “somewhat agree” with the questionnaire items assessing their satisfaction with the program (Table 5).
Primary Care Provider Feedback on the Clinical Decision Support Report
One provider did not respond to the medication adherence calendar questions.
BG, blood glucose; BP, blood pressure; EMR, electronic medical record.
Telehealth Nurse Satisfaction with the Program
DSM, diabetes self-management; PCP, primary care provider.
Discussion
The current study showed that T2D patients taking part in a brief diabetes telehealth program focusing on daily medication adherence rated the usability of our BG meter, BP cuff, and pillbox RHM device suite highly for its ease of use, usefulness, and convenience when used in the home. Patients also rated program satisfaction highly in terms of support from the diabetes care team, helpfulness of nurse outreach calls, and their wish to keep using the program if it were available and indicated that they would recommend the program to other patients. Improvement in BG control was clinically and statistically significant with an HbA1c drop of 0.6% observed over the 3-month program. This benefit was achieved with minimal nurse outreach (three brief scheduled calls), minimal nurse and provider staff training, and no structured diabetes education protocol in place for the nurses to deliver. The monthly cost per patient ($220) over 3 months was largely (78% of total cost) for the initial RHM device and hub hardware, and the remainder was for monthly data fees and BG strip and lancet supplies for the BG meter. If the program were extended to 1 year, the average monthly fee would drop to $92. Thus, this program is low cost as delivered and could be easily integrated into busy primary care settings.
We found a mean weekly medication adherence rate of 80% for all 12 weeks of the program (rising to above 90% for the 3 initial weeks). Oral agent medication adherence is reported as 61–79% for T2D diabetes populations using a single pill electronic medication pillbox device, the Medication Event Monitor Systems (MEMS®; APREX, Division of AARDEX, Union City, CA) and with prospective tracking of medications. 15 Moreover, African American T2D patients (who made up the majority in the current study population) have been reported to have a 1.8 times higher medication discontinuation rate compared with other patients. 16 Thus, the current pilot telehealth program had a substantial positive impact on medication adherence when used to augment usual care provided to a poorly controlled T2D population attending an urban safety net clinic.
The results also showed that clinic providers reported consistently high ratings for the clarity and ease of use of the CDS reports we provided in the form of summary RHM graphs at the end of the 3-month program, as well as high ratings for its clinical usefulness. The providers indicated that the report should be located in the future within the hospital electronic medical record, where they did their daily clinical work. The CDS report was delivered in this study as a hard copy pdf file into the patient's electronic medical record inbox by the telehealth nurse interventionists but was not incorporated into the active patient management areas of the electronic medical record.
A weakness of the study was that the patient sample was a highly selected group with 73% African American patient representation compared with the local clinic T2D population, which is 25% African American. This difference reflects our inclusion criteria in this study, as 40% of our clinic patients are Latino, and many do not speak English as a first language as was required to join the study. Future studies could adopt a strategy we have used in prior local studies to include bicultural, bilingual Latino research staff and diabetes team staff to provide the appropriate culturally competent staffing capacity to manage a more representative study population. 14 It is notable that there were significant provider concerns regarding the suitability of recruiting poorly controlled safety net clinic patients into a novel diabetes telehealth program, resulting in an upper patient eligibility criterion of HbA1c level being set at 11%. Future research could expand the scope and reach of the program in other ways (e.g., to include younger patients, all insulin users in the patient registry, and patients seen at non–safety net clinics that differ in patient demographic and clinical characteristics and insurance coverage mix) to provide a wider and more representative patient sample as part of a more pragmatic research approach. 17
Also, our intervention design (and research resources) allowed for only limited allocation of nurse time (i.e., two RNs working together half a day per week) to respond to the total of 72 RHM device alerts generated for all patients during the study. Only 6.4% of the 72 flagged alerts required an additional, unscheduled outbound telephone call from one of the nurse interventionists, as many were judged unremarkable by the RNs because they had been resolved by the time they were reviewed. Future research examining our diabetes telehealth intervention could provide more practical and immediate RN response to provide reassurance, education, or referral, as needed. An established nonurgent hospital diabetes telehealth program for poorly controlled, Medicaid T2D patients (“HouseCalls”; New York City Health and Hospitals Corp., New York, NY) that we evaluated in prior research uses a 2-h RN response window to RHM device alerts (for hyperglycemia and hypertension) on weekdays and during office hours based on device alert protocols for out-of-range values similar to those used in this study. 12
The clinical benefit of our telehealth program may be attributable to the improved level of patient engagement by daily use of the RHM devices and also as a result of research staff support and outreach by phone in the critical early phase of the 3-month program. Research staff members checked-in with all patients, particularly in the first week of the program, to see if they had questions regarding use of the RHM devices or concerns regarding data obtained from the devices. This support role by research staff could be formalized into a standardized clinical care protocol that could be implemented by community health workers or patient outreach staff and case managers as part of an expanded diabetes team model. 8 Although staff registered nurses (i.e., our nurse interventionists) delivered the brief telephone outreach component of the program, this was not an ideal use of these clinic staff members, and their lower satisfaction with the program compared with patients and providers was described as reflecting the simple “checking in” nature of the calls made as part of the intervention protocol. These nurses could be alternately trained in future research to deliver a brief diabetes education protocol with supervision by a certified diabetes educator who specializes in diabetes education and behavior change or by an endocrinologist or primary care provider with expertise in diabetes.
We did not examine here the clinical impact of the program on provider medication intensification behaviors or the quality of provider–patient communication achieved during clinic visits following the intervention. Future qualitative and quantitative studies should be carried out to examine these important issues as well as the impact of a longer-duration program to allow time for patients and staff to develop enduring ways of using the telehealth system and identify any long-term barriers to participation or safety issues with longer-term use. Also, newer technology versions are increasingly being made available for the RHM devices, including a lockable pillbox that was not available for this study, that would strengthen patient safety planning and patient and provider satisfaction with the program.
Conclusions
These findings provide encouraging empirical support for the usability and clinical usefulness of our 3-month diabetes telehealth program that was delivered to an urban poor clinic population and that was enriched by the integration of a user-friendly cellular pillbox and CDS tools.
Footnotes
Acknowledgments
We would like to thank the McKesson Foundation for its financial support of this project in the form of an m-Health Innovation research grant.
Disclosure Statement
G.W. is Chief Scientific Officer at Silver Fern Healthcare LLC. A.B. and S.Z. declare no competing financial interests exist.