
Abstract
Introduction
Because of the emerging needs of point-of-care testing (POCT) in medicine, various POCTs have been developed that assess glucose levels, pregnancy, uric acid, human immunodeficiency virus (HIV), and other biomarkers. POCTs are a convenient and fast way to diagnose disease. 1,2 There may be a smaller need for POCTs in the general hospital because of established hospital labs, but, in some cases, POCTs are used to immediately confirm the test results of patients, especially after working hours. POCTs are frequently performed in the emergency room (ER) owing to their ease of use and rapid results, making POCTs useful in crowded and busy ERs. 3 –5 POCTs can also help medical staff properly treat patients.
Most POCT kits are disposable and visually indicate the results by changing colors or making lines at specific locations. Operators have to wait a desired time period, generally between 1 and 30 min, after loading the sample to see the results. 1,6,7 There may be no problem waiting for the results when using personal kits, but in the ER simultaneously testing multiple POCT kits is very confusing because checking the remaining time on each kit and noting the results are redundant. In addition, errors may occur when checking or writing down the results, and these errors cannot be confirmed after the kit is discarded. These issues hinder the use of POCT kits in the ER despite their merits.
To address these problems, taking a picture of the test results after the reaction time and storing the image in the electronic medical record (EMR) could be the ideal solution. This requires a computerized system, timer, camera, and network adapter. A good example of such a system is a smartphone, which generally contains a built-in camera and wireless adapter. Custom smartphone applications can resolve user interface, timing, and EMR connection issues. Research on using smartphones in medicine is emerging because of powerful tools, such as wireless interfaces, touch-based user interfaces, programmability, and computing power. 8 –11
However, only a few articles have been published on using smartphone-based systems with POCT kits. Dell et al. 12 developed a smartphone-based diagnostic system for immunoassay kits that records and analyzes colorimetric changes in the sensor. A similar study on quantifying colorimetric diagnostic kits using a smartphone was reported by Shen et al. 13 Other studies have reported using a smartphone and custom-developed sensors to assess enzyme-linked immunosorbent assays 14 and measure thyroid-stimulating hormone. 15 However, these studies mainly quantify the results of test kits and do not consider the transmission of test results to a remote server or other hospital requirements. In other words, previous studies on smartphone-based system for POCT kits are mostly only suitable for personal use.
This article describes a smartphone-based system for POCT kits that takes a picture of the results and wirelessly transfers the image to the EMR for review by medical staff. This system is convenient, saves time, reduces the workload, and automatically saves the results of disposable kits. In addition, securing the safety of the medical staff is possible because of the fast recognition of HIV infection status. To achieve these goals, we designed a platform for a smartphone and POCT kit and programmed an application that allows the user to control the entire process: waiting for results, taking the picture, and sending the captured image to the EMR. We tested POCT kits for detecting HIV, but the platform was designed to receive any POCT kit by separating the kit stand from the platform. The developed application reads barcodes to identify the patient identification number (ID) or prescription number and can be easily modified to adjust for waiting time and the address of the EMR server.
Materials and Methods
System Design
The system was designed after taking into account suggestions from the clinicians in the ER about the needed features. Clinicians need a simple user interface that operates with minimal touching, built-in magnets on the side of the body for the easy attachment of multiple devices and multiple kits at the same time, a removable tray that provides a simple way to place and remove test kits, and the ability to read barcodes in order to conveniently identify patient ID and prescription numbers and that is portable and light-weight. The final design was confirmed after several modifications and discussions with clinicians.
Smartphone
We identified several key smartphone features required for our proposed system: image quality, autofocus, camera positioning, cost, and weight. After these features were considered, the Galaxy S3® mini (Samsung Electronics Co., Suwon, Republic of Korea) was considered the best fit.
Android Application
The application was built for Android™ version 4.1 (Google, Mountain View, CA) because the Galaxy S3 mini uses Android version 4.1.2. The standard Android software development kit was used to develop our application. The key functions of the application include a barcode reader, timer, ability to take pictures, and the wireless transmission of pictures. We obtained open source codes from a Web site used by the open source community to facilitate barcode recognition. 16 Other functions and user interfaces were custom programmed. To transmit the pictures to a server via the wireless network, transmission control protocol/Internet protocol (TCP/IP)-based network communication was used. The smartphone was connected to the internal wireless network of Asan Medical Center (AMC), Seoul, Republic of Korea, and pictures were transferred to the server, which was also connected to the internal AMC network. Application settings can be easily modified using a simple touch-based interface. The user can change the IP address of the server, time required to wait for results, and other settings.
Intermediate Server
When the smartphone takes a picture of the results, the picture is transferred to an intermediate server because AMC policy prevents direct data transmission to the EMR server from unapproved devices. Therefore, we sent all pictures to an intermediate server managed by AMC's system operator. We programmed JAVA software (Oracle Corp., Redwood City, CA) to receive and transfer the pictures to the EMR server, and the software always runs on the intermediate server. The software receives the pictures from the smartphone and transfers them to the EMR server using Health Level 7 (HL7) protocol (version 2.x, OBR message).
Poct Kit for HIV Detection
Among several POCT kits approved for HIV detection, we selected OraQuick Advance® (OraSure Technology, Bethlehem, PA). Results become available in 20 min, and both blood and oral fluids can be used. Reading the test results is as simple as general pregnancy tests. The patient is infected with HIV when there is a line at “T” (the test position), and a line at “C” (the control position) confirms that the test is working.
Performance Validation
The performance of the system was verified from a survey of users after test periods. Ten medical staff members at the ER completed the survey, which consisted of six questions. The questions were modified from general customer satisfaction survey questions. Three of the questions used the Likert 5-point scale, and the remaining questions requested short answers.
Results
Developed System
Figure 1 shows a photograph of the developed system. The system measures 7×18×15 cm (width×length×height). The smartphone is placed at the front of the system, and the POCT kit is positioned at the other end. Both the barcode and the test kit are included in one image. We designed detachable holders for the easy placement and discard of the POCT kits. Users did not need to pick up the entire system to replace the POCT kit. In addition, the position where the barcode sticker needs to be placed is indicated by a rough surface. This not only helps find the correct location for the sticker, but also helps in removing the sticker when testing is finished. Furthermore, magnets were included on the sides of the system. The magnets can support two or more developed systems in parallel for testing multiple samples at the same time. The total cost of the system is about $400 ($300 for the smartphone and $100 for the body of the system), and this cost could be lowered with mass production.

Photograph of the developed system.
Smartphone Application
Figure 2 shows a screenshot of the developed application, which requires six steps. When the application is executed, a screen with a start button appears (Fig. 2a), and the application waits until the start button is touched by the user. The application recognizes the barcodes when the test starts, displays the recognized patient ID or prescription number, and then waits for confirmation (Fig. 2b). The user needs to confirm that the number is the same as the number on the printed sticker and then press “yes.” A 20-min digital countdown is displayed after barcode confirmation (Fig. 2c). When the countdown finishes, the application takes a picture of the POCT kit (Fig. 2d) and transfers the picture to the intermediate server. The six steps are as follows: 1. Click start button (Fig. 2a). 2. The application reads the barcode (prescription number or patient ID) and waits for user confirmation (if the number is correct, the user presses “Correct”; if not, the user presses “Incorrect,” and the application must recognize a new barcode) (Fig. 2b). 3. The countdown starts when the barcode is confirmed (Fig. 2c). 4. The smartphone focuses on the POCT kit and takes a picture of the results (Fig. 2d). 5. The smartphone transmits the picture to the intermediate server (Fig. 2e). 6. The application automatically returns to the first screen (Step 1) after successful transmission (Fig. 2a).
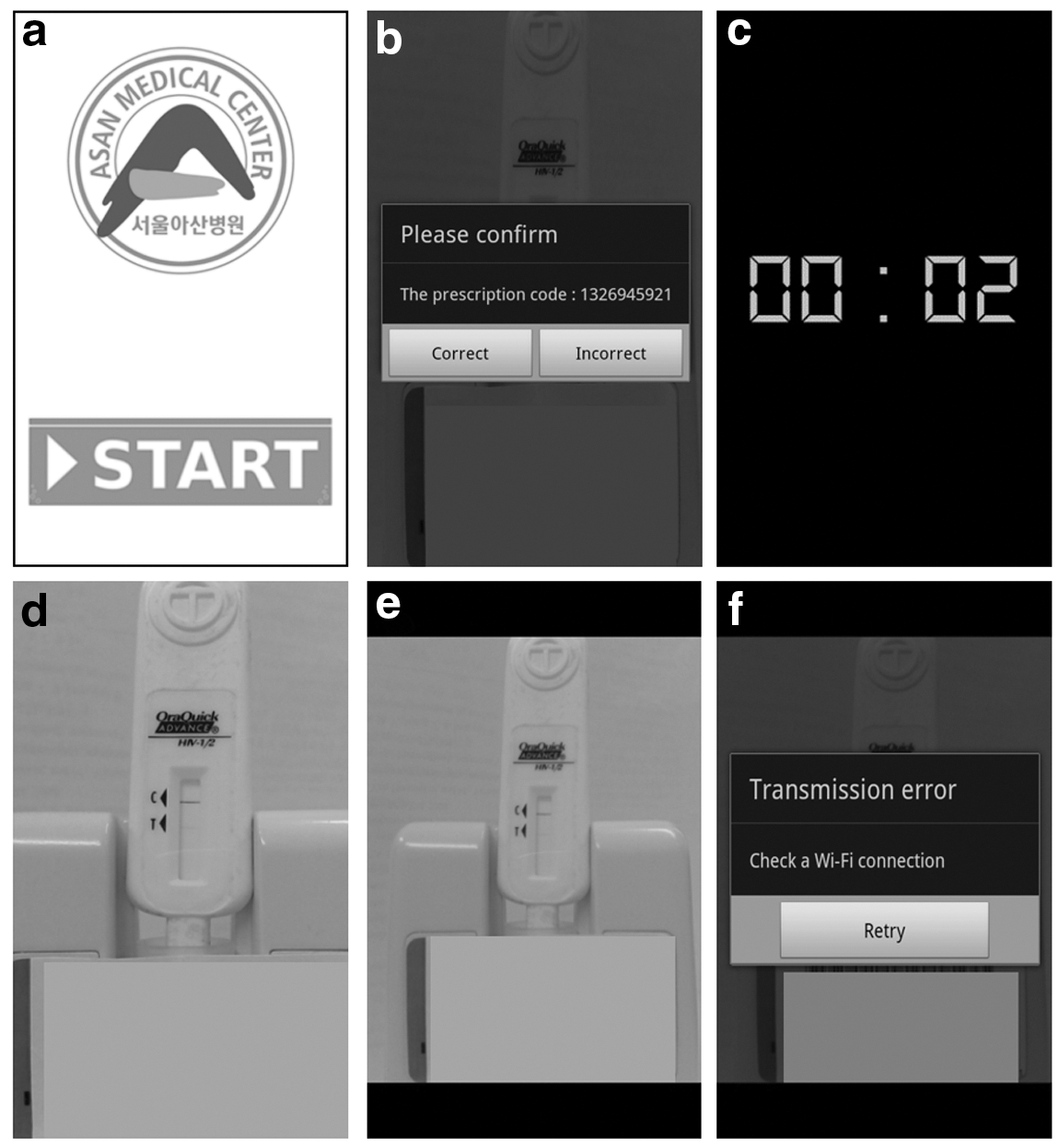
Screenshots of the smartphone application:
To minimize the operation time for the user, only two touches are required if no problems develop. When there is a problem transmitting the picture, the application shows an alarm and prompts the user to check the wireless connection. The user can retry transmission after addressing any network problems by touching the retry button (Fig. 2f). In addition, the application shows a warning when the user tries to run the test without changing the previously used POCT kit by automatically checking the barcode history.
Connecting to EMRS
When the picture is successfully transferred to the intermediate server, the server sends a message to the EMR server (according to the HL7 standard protocol), and the picture is linked to the patient's EMR. Physicians can then check the results in the EMR and confirm the infection status of the patient (Fig. 3). By connecting the results of the POCT kits and the EMR system, the medical staff can easily check the results without losing the results after the kit is discarded.
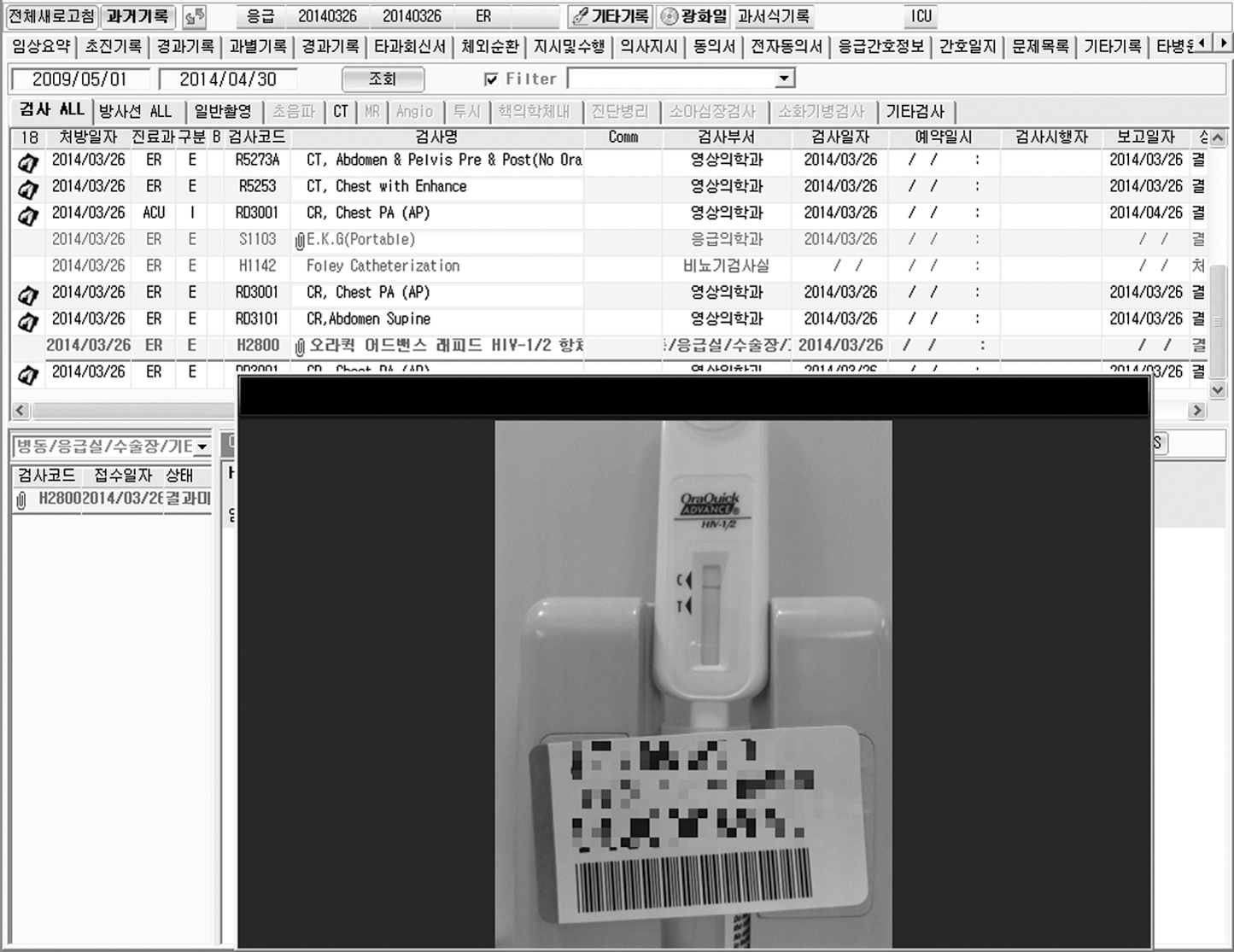
Electronic medical record showing the picture of the results obtained using our system.
User Survey Results
After the primary 10-month testing period (from July 2013 to April 2014), a simple user survey was conducted to receive feedback from the users. The survey questions are listed in Table 1.
Survey Questionnaire for the Evaluation of the Developed System
The first question asked if the system helped reduce the time required to report the results: 80% positively answered that the system shortened the time, 20% answered “neutral” (i.e., did not notice significant differences), and there were no “negative” answers.
The second question is related to the first question and asked how much time the developed system was able to save. People who answered positively to the first question replied that 10–60 min could be saved using the system (average, 32 min).
The third question asked about reducing workload: 60% answered that the system reduced workload, 40% answered “neutral,” and there were no “negative” responses.
The fourth question asked about willingness to use a commercially available developed system: 100% “strongly agreed” that they would use such as system. The answers to questions 1, 3, and 4 are shown in Figure 4. There were no answers to the fifth question, which asked why they would be unwilling to use a developed system.
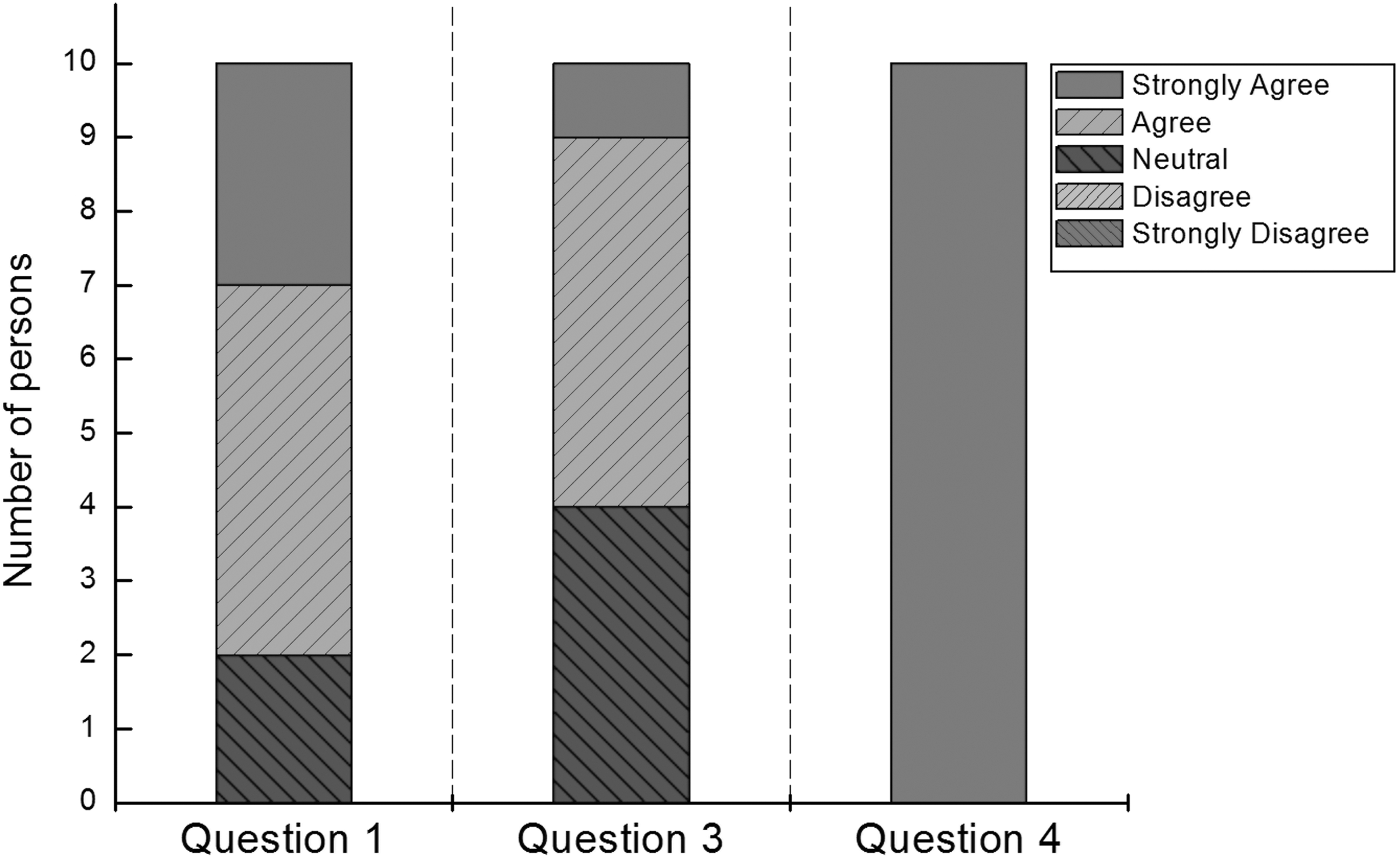
Answers to survey questions 1, 3, and 4 (see Table 1) according to the Likert 5-point scale (n=10).
Question 6 asked for additional applications of the developed system. Seven persons suggested that the system could be used to detect human chorionic gonadotropin for pregnancy testing, which is a routine test for any fertile woman who presents at the ER. Four users suggested hepatitis C virus testing as a possible application of the developed system.
Discussion
We have successfully developed a smartphone-based automatic system for managing the results of POCT kits in the ER, which takes a picture of the test results after the required time has passed and transfers the image to the EMR server. The users (i.e., medical staff) only need to put the test kit on the developed device and confirm the patient ID or prescription number. Medical staff can check the results whenever they look at the patient EMRs. From the beginning, the system was designed to consider the needs of medical staff. Therefore, the system contains several user-friendly aspects, such as a simple user interface, built-in magnets for the easy placement of several devices, a removable tray, and a barcode reader. The inclusion of these features resulted in positive feedback after 10 months of testing: 80% of users reported positive responses, and they reported that the developed system reduces processing time by approximately 32 min (from ordering the test to reporting results). Furthermore, 60% of users reported that the developed system reduced workload, and 100% of users would use the system if it was commercially available.
The ER is one of the busiest parts of any hospital, and the ER medical staff suffers from a heavy workload and high risk of infection. Our developed system is suitable for use in this environment. During the 10-month test period, the HIV tests of >100 patients were processed, and 2 HIV-positive patients were identified. We believe our system could help protect medical staff from infection.
The proposed system does not offer the automatic identification of the test results because it was not designed for HIV tests. Users can test any POCT test that requires the visual inspection of the test results by modifying the removable tray. Furthermore, legal issues can be avoided when the physician confirms the results. Kit-specific applications that perform image analyses could be developed to automatically identify POCT results. Our system was only tested in the ER, but it could be applied anywhere POCT tests are required. In addition, owing to the convenience and portable size of the system, it could be used in local clinics and dental clinics because the system stores the images on either the internal or external memory of the smartphone.
Conclusions
Here, we describe a system for the automatic management of POCT results in the ER. This system recognizes the patient ID or prescription number, provides a countdown to when the test results will be ready, takes a picture of the test results, and transfers the results to the EMR server. These features received positive feedback from the users after the 10-month testing period. We used POCT HIV detection kits in this study, but the system could also be used with any POCT tests that require visual inspection (e.g., human chorionic gonadotropin or hepatitis C virus kits). The further application of kit-specific clinical support functions requires further development.
Footnotes
Acknowledgments
This research was supported by the Bio & Medical Technology Development Program of the National Research Foundation funded by the Ministry of Science, ICT & Future Planning (2014-034366).
Disclosure Statement
No competing financial interests exist.