
Abstract
Introduction
Owing to medical resources often being unequally distributed, people in rural areas may be unable to acquire sufficient healthcare services for their needs. Furthermore, with an increasingly aging population, healthcare demands are also on the rise. Many countries have been confronted with such above-mentioned situations and thus have vigorously formulated a variety of solutions to attack such problems. Among these various propositions, telemedicine in particular seems to provide a promising means for the resolution of these problems. In this article, telemedicine refers to “the use of information technology (IT) to support healthcare services and activities via an electronic transmission of information or expertise among geographically dispersed parties, including physicians and patients, in order to improve health service effectiveness and resource allocation/utilization efficiency.” 1 Although other terms such as telecare/telehealth are sometimes used to refer to a broader definition of distant healthcare, we use telemedicine in this article to refer to medicine or healthcare in the same vein.
The development of telemedicine in Taiwan began under the National Information Infrastructure project started in 1994. Experimental projects such as teleconsultation and distance education were launched at that time, but telemedicine has still not become widely adopted by hospitals despite the fact that Taiwan is covered with mountainous areas and dotted with isolated outer islands. 2 Until recently, the Ministry of Health and Welfare 3 has continued initiating a Pilot Telecare Project along with a Telecare Services Modification Project and a Quality Modification Project. The “Telecare Service Development Project” was undertaken in 2009 to foster additional telehealthcare services, to improve the supported policies and related mechanisms, and to inspire the involvement of related industries in the process. Despite the initiation of these pilot telemedicine programs, the utilization rate of telemedicine in Taiwan remains dissatisfying. More in-depth investigations are thus required to obtain an improved understanding of this phenomenon in order to ameliorate the situation.
The Theory of Planned Behavior (TPB), derived from a theory of reasoned action, has been widely adopted to predict a person's given intention toward a particular behavior. 4 TPB postulates that target behavior can be predicted by intentions (behavioral intention [BI]), which, in turn, are jointly affected by three main components: attitude (AT), subjective norm (SN), and perceived behavioral control (PBC). Previous studies 1,5 have used TPB to explore physicians' intention to adopt telemedicine and have also advanced our knowledge of physicians' adoption decision making. However, these previous studies did not take into consideration the influence of physicians' experience on the adoption of telemedicine as Venkatesh et al. 6 asserted. Their research contention is that experience was not explicitly included in the TPB model as a moderator to verify its influence on the relationships among AT, SN, PBC, and BI. Omission of important moderating variables might erroneously specify the IT adoption model and influence a physician's adoption of telemedicine negatively. Differing strategies according to differing moderating variables may thus be formulated to foster the adoption of new IT. In our study, any physicians who have ever used telemedicine-related services such as tele-education, teleconsultation, telemonitoring, or teleradiology are considered as experienced users.
There have been a few previous studies looking at the influence of experience on the adoption of new technologies within the healthcare industry but with mixed results. For example, Carayon et al. 7 examined nurses' experience with the use of a smart intravenous pump. The results show that nurses' positive acceptance of the smart intravenous pump significantly increased after 1 year of implementation as users' general experiences associated with the pump improved over time. Kijsanayotin et al. 8 found that previous IT experiences can predict health IT use in Thailand's community health centers. In exploring Singapore women's acceptance of health information seeking via mobile devices, Lim et al. 9 found that prior experiences of health information seeking contribute to positive usage intentions. However, Pynoo et al. 10 found no main effect of experience on physicians' acceptance of Picture Archiving and Communication Systems. Schectman et al. 11 found that the use of an expert system for ambulatory prescription by physicians was not associated with prior computer experience.
For IT to enhance organizational performance, it must be used by employees in organizations. 6 Physicians do play an important role in adopting usage of telemedicine among medical facilities. Consequently, how to further impel the use of telemedicine technologies by physicians is thus an imperative issue that remains yet to be addressed. Hence, our study not only aimed to investigate the influencing factors that drive physicians to adopt telemedicine technologies, but also aimed to scrutinize the moderating effect of relative experience using telemedicine on the adoption intentions of those physicians.
Research Framework and Hypothesis Development
Our study adopted the TPB 4 as the theoretical foundation necessary to explore a physician's BI to adopt telemedicine. As Figure 1 shows, the three primary determinants (i.e., AT, SN, and PBC) collectively determine a physician's intention to use telemedicine. AT refers to a physician's positive or negative feelings about using telemedicine. 6 SN is defined as the physician's perceptions that people who are important to him or her hold on whether he or she should or should not use telemedicine. 6 PBC refers to the perceptions of the availability of skills, opportunities, and resources required for using telemedicine. 5 In line with TPB, we postulate the following hypotheses:
H1: There is a positive relationship between physicians' AT toward telemedicine and their intention (BI) to use telemedicine.
H2: There is a positive relationship between physicians' perceived SN and their intention (BI) to use telemedicine.
H3: There is a positive relationship between physicians' PBC and their intention (BI) to use telemedicine.
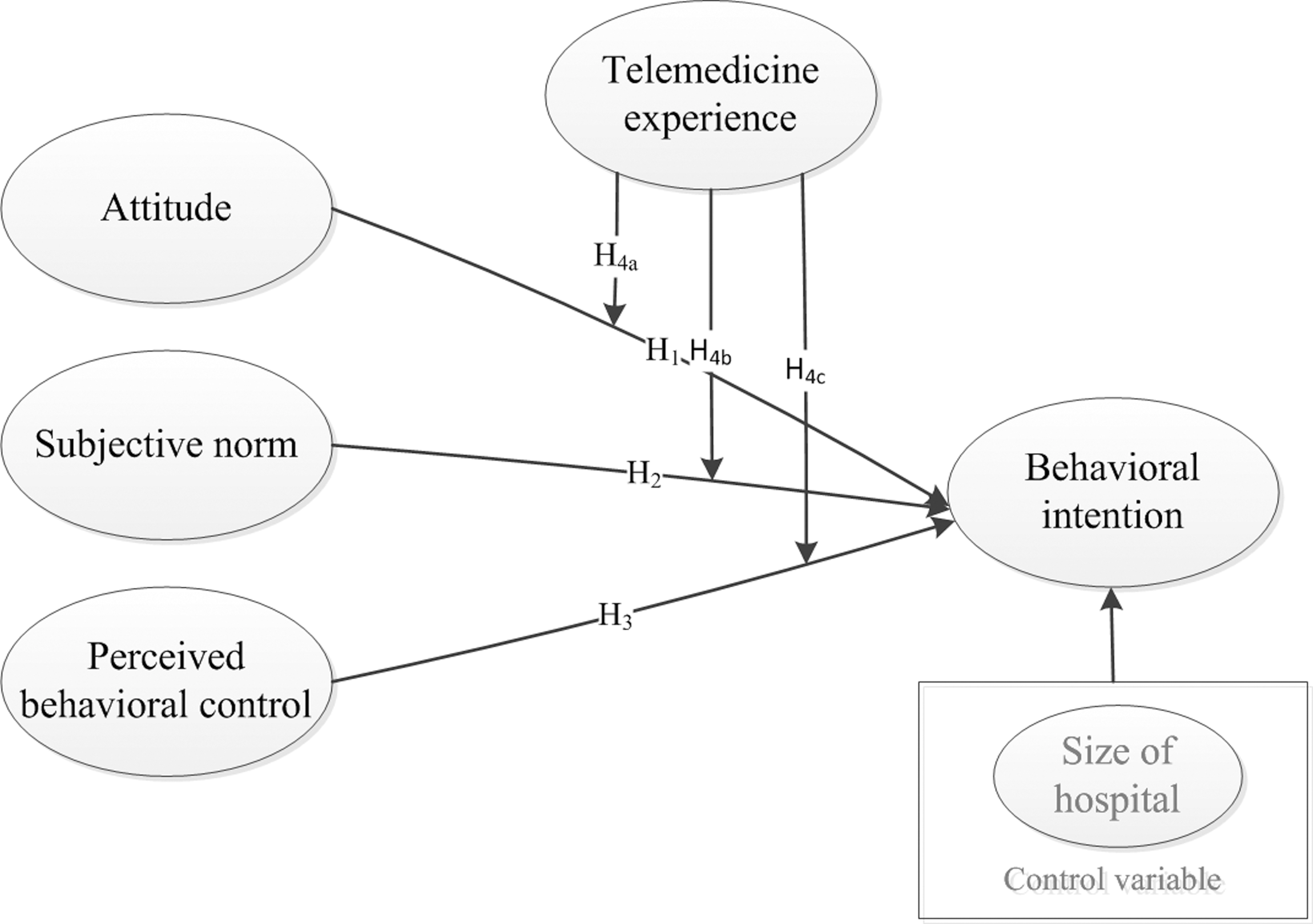
Research framework. H designates a hypothesis being tested.
Because the influence of telemedicine experience on the relationships among AT, SN, PBC, and BI remains an unsolved issue,
6
we proposed the following hypotheses to better understand its moderating influence: H4a: Physicians' telemedicine experience moderates the relationship between their AT and BI to use telemedicine. H4b: Physicians' telemedicine experience moderates the relationship between their perceived SN and BI to use telemedicine. H4c: Physicians' telemedicine experience moderates the relationship between their PBC and BI to use telemedicine.
Furthermore, to eliminate the potential influence of the size of hospitals where physicians are located, we have also included a control variable of “size of hospital” in the research framework.
Materials and Methods
To validate the proposed model, we undertook a cross-sectional survey and used questionnaires to collect physicians' perceptions concerning their use of telemedicine.
Measurement Development
According to the guideline for questionnaire development of Churchill, 12 our study included items from prior literature to generate an initial pool of scales for each construct. Next, an expert panel consisting of three Taiwanese physicians with prior telemedicine experiences inspected these items. A few ambiguous words were modified, along recommendations made by the experts. The survey items were measured on a 7-point Likert scale (from 1 for “strongly disagree” to 7 for “strongly agree”). The instruments for AT, SN, and BI were adapted from those of Venkatesh et al. 6 and were measured using three, two, and three items, respectively. PBC was measured using a four-item scale developed by Venkatesh et al. 6 and Taylor and Todd. 13 The original source questionnaire was provided in English and was therefore inappropriate for our target subjects. Hence, we used a back-translation approach to assure that the meaning of original scales would not be changed when translating survey items from the English version into traditional Chinese. One of our authors first translated the English version of the instrument into traditional Chinese, and then an independent translator back-translated the Chinese version into English. Original and back-translated instruments were then compared, and divergences were revised and remedied between these two versions questionnaires by our expert panel. The Appendix shows the final survey items.
Sampling and Ethics Approval
Permission from the Institutional Review Board of a large hospital in Taiwan was obtained prior to investigation. To validate the proposed model, we conducted a field survey of convenience sampling for the collection of data. In Taiwan, hospitals can roughly be classified into three separate levels: medical centers, regional hospitals, and district hospitals. Prior to the sending out of the questionnaires, we successfully contacted 15 hospitals, including 5 medical centers, 7 regional hospitals, and 3 district hospitals, to secure their collaboration. We assigned a coordinator for each hospital to help with the distribution and collection of the questionnaires. Physicians in the 15 hospitals were invited to participate in a paper-and-pencil survey. In total, 300 questionnaires were distributed to these coordinators, and 125 questionnaires were returned to the researchers. After 19 incomplete questionnaires were excluded, 106 questionnaires were left for subsequent analysis.
Results
Respondent Characteristics
Most respondents were attending physicians (56.6%) and were between 41 and 50 years of age (36.8%). Only 31 physicians had had any experience in using telemedicine (29.2%), with tele-education being the most widely experienced telemedicine service. The detailed distribution of respondents and hospitals is shown in Table 1.
Demographics of Respondents
However, because the usage experience of various telemedicine applications is different, we conducted a chi-squared test to assess if there is a difference among those experienced physicians. The results revealed that the chi-squared value is not significant (χ 2 =0.295, df=3, p=0.295), indicating there is no difference among these physicians regarding their telemedicine usage experience. Among the 15 hospitals surveyed, 10 hospitals have implemented tele-education service to date. Telemonitoring and teleconsultation services were also adopted by two and five medical centers, respectively. Only one regional hospital has adopted a teleradiology service, which was initiated as a pilot telemedicine programs by the Ministry of Health and Welfare, Executive Yuan, Taiwan.
Model Evaluation
The proposed model and hypotheses were empirically validated using partial least squares, a component-based modeling technique, 14 supported by SmartPLS® version 2.0 M3 software. 15 To validate the proposed model, we tested the measurement model and the structural model separately. 14 We verified the measurement model by assessing its reliability and validity including item loadings, construct reliability (composite reliability and Cronbach's α), average variance extracted, discriminant validity, and convergent validity. 14
The item loadings of our study were higher than the 0.7 threshold, 14 indicating sufficient item reliability. Cronbach's α and the composite reliability of the constructs investigated all exceeded the 0.7 criterion, 14 demonstrating sufficient construct reliability. Furthermore, the average variance extracted of all constructs was also higher than the 0.5 criterion, 14 demonstrating reasonable convergent validity. Finally, discriminant validity is gauged by comparing the square root of average variance extracted and the correlation between two constructs. Our results revealed that the former should be higher than the latter, demonstrating sufficient discriminant validity.
Regarding the structural model, we also used partial least squares for analyzing the responses of telemedicine-experienced and -inexperienced physicians, respectively. Of the three hypotheses, only hypothesis H2, which postulates that SN will influence BI for experienced users, was not supported (Tables 2 and 3). All the other hypotheses for both groups of physicians were supported. Overall, the proposed model accounted for about 58.8% of the variance of BI for combined data (Fig. 2). Moreover, the proposed model accounted for 37.9% of the variance in BI for experienced physicians and for 68.1% of the variance in BI for inexperienced ones. Regarding the control variable, the size of the hospital was not found to be significant. The relationships among AT, SN, PBC, and BI for combined data are still significant, regardless whether the size of the hospital is included. That is, the size of the hospital has been controlled in our study.
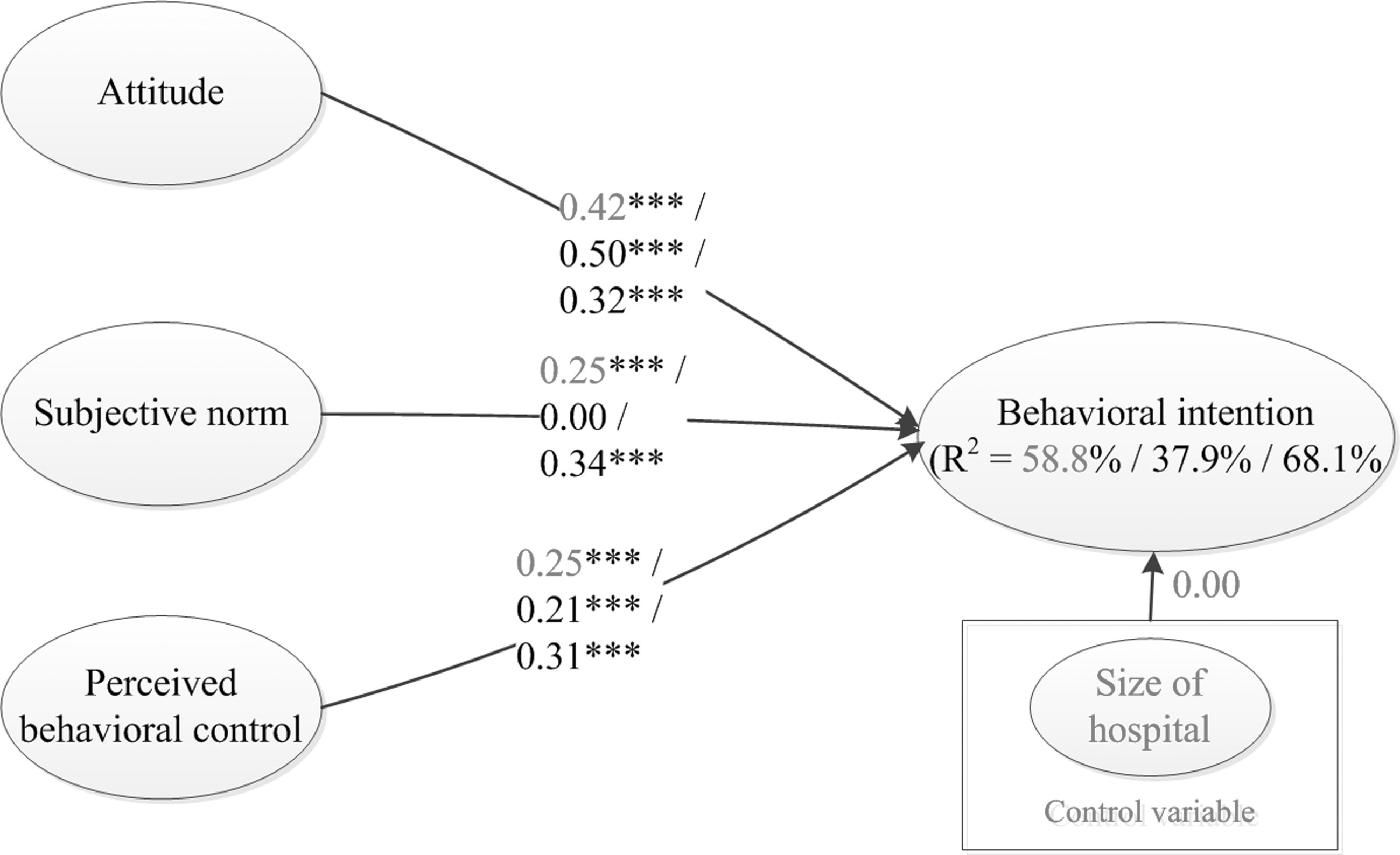
Structural model results (combined data for telemedicine-experienced and -inexperienced physicians, ***p<0.001).
Results of Structural Model for Combined Data
p<0.001.
AT, attitude; BI, behavioral intention; SN, subjective norm; PBC, perceived behavioral control.
Results of Structural Model for Experienced and Inexperienced Physicians
p<0.001.
AT, attitude; BI, behavioral intention; SN, subjective norm; PBC, perceived behavioral control.
Table 4 gives the results of group comparison tests 16 for hypotheses H4a, H4b, and H4c. For experienced physicians, there is a stronger positive influence of AT on BI relative to inexperienced ones. For inexperienced physicians, there is a stronger positive impact of SN on BI compared with experienced ones. Finally, for inexperienced physicians, there is a stronger positive influence of PBC on BI relative to experienced ones.
Group Comparison of Experienced Versus Inexperienced Physicians
p<0.001.
AT, attitude; BI, behavioral intention; SE, standard error; SN, subjective norm; PBC, perceived behavioral control.
Discussion
The Effects of at on BI
Whether or not physicians are experienced with telemedicine technology, we found AT to be an important predictor of physicians' intention to use telemedicine. That is, the more favorable the perception in a physician's AT toward telemedicine technology, the greater the likelihood that the physician will use such telemedicine in his or her practice. In the case of experienced physicians, the effect of AT on BI was stronger than that of inexperienced physicians. This finding indicates that if experienced physicians hold a more positive AT toward telemedicine technology, they will surely use more telemedicine than inexperienced physicians do. Consequently, to boost the usage of telemedicine, hospitals can encourage experienced physicians to share their facilitative telemedicine experiences with inexperienced physicians to foster a more positive AT toward telemedicine technology usage. Because experienced physicians comprehend what benefits they can acquire by using telemedicine technology, they should be very persuasive to others.
The Effects of SN on BI
SN was found to exert no significant influence on experienced physicians' intention. The finding was in line with that of Chau and Hu 5 but not with those of Hung et al. 17 and Taylor and Todd. 13 Previous literature 5,13 argued that the mixed results of the effects of SN on BI might result from the differing natures of study subjects. Chau and Hu 5 asserted that subjects possessing characteristics such as specialized training, autonomous practice, or independent thinking might place less weight on the opinions of others on a given topic. Therefore, physicians tend to be such typical professionals possessed of the above-mentioned traits, and this may well explain why the insignificant effects of SN on BI have come to exist.
However, our analysis concerning inexperienced physicians showed that SN was significantly influencing their BI toward telemedicine technology. In other words, inexperienced physicians could be influenced by their friends, colleagues, or superiors regarding telemedicine usage. This is an interesting finding and in line with the study of Taylor and Todd. 13 Prior literature 18,19 also demonstrated that SN is important in the early stage of information systems development/adoption but will be lessened over time as experiences increased. Transferring this rationale to our study, telemedicine is a new concept for those physicians who have no usage experiences, and thus SN may play an important role in the promotion of telemedicine technology. Furthermore, our multigroup analysis showed that the strength of the relationship between SN and BI for inexperienced physicians is significantly stronger than that for experienced ones. Based on the finding, it might imply that hospitals can make good use of superiors or experienced physicians to convince inexperienced physicians regarding the advantage that telemedicine technology can convey in order to arouse their interests or even usage intention regarding telemedicine technology.
The Effects of PBC on BI
The path analysis revealed that PBC is a significant predictor of BI for both groups of physicians. Currently in Taiwan, roughly 415 hospitals have enrolled in the National Insurance Program for reimbursement of the healthcare services they provide. Because the National Health Insurance Administrator demands access to computerized reimbursement, all hospitals are forced to use IT for accelerating the reimbursement process. Consequently, most hospitals in Taiwan already possess sophisticated IT capabilities and related resources. Among these hospitals, more than 300 hospitals have previously adopted electronic medical records systems, and thus physicians in Taiwan should have reasonable access to these resources and maintain adequate computer literacy on a daily basis. Also, physicians belong to a highly specialized profession, and, as such, they are well educated and tend to learn new things quickly. 17 This finding may imply that hospitals should provide physicians with sufficient telemedicine-related hardware, software, and training programs to improve the overall adoption/usage of telemedicine. Physicians may thus feel that telemedicine can also be used or controlled and will result in their stronger intention to subsequently use telemedicine.
Conclusions
Based on TPB, our study validated a research model designed to advance our understanding of telemedicine adoption perceptions among physicians. The results revealed that AT, SN, and PBC were significant predictors of BI to use telemedicine for combined data. We further conducted a multigroup analysis by dividing physicians into experienced and inexperienced groups. For experienced physicians, only AT and PBC were significant determinants of BI. Regarding inexperienced physicians, AT, SN, and PBC were proven to be significant predictors of BI. Several implications for research and practice can be derived from this study.
Implications for Research and Practice
TPB has been proven a superior model for predicting an individual's intention toward a specified behavior. Extant literature, however, has primarily focused on general users regardless of their experiences. Our study attempts to fill this gap by comparing those perceptions regarding telemedicine between experienced and inexperienced physicians. Meanwhile, the results revealed that SN was unable to predict BI for experienced physicians but did so for inexperienced ones. This finding may shed light on future study for a more in-depth study on the influence of SN on differing settings/subjects types.
Our research also implies several practical implications. Becasue SN does not predict experienced physicians' BI, hospitals must place more emphases on their AT and PBC approaches to inspire physicians' BI toward adopting telemedicine technology. Concerning inexperienced physicians, the significant factors influencing a physician's adoption behavior found in this study can allow hospitals to pay more due attention to it. To sum up, differing strategies for experienced and inexperienced physicians must be formulated to boost the adoption of telemedicine technology.
Limitations and Future Directions
Because we collected a sampling from only 15 hospitals in Taiwan, a generalization of results to other hospitals and countries may not be safely made. Furthermore, we conducted this study in a cross-sectional perspective, which might not be able to capture the impact of the changing AT. Hence, it may obtain more insights to the proposed model if longitudinal studies were to be conducted at a later date. Another limitation is the potential influence of physicians' differing usage experience of telemedicine applications, such as tele-education and teleradiology, which might confound the result. Future research could collect more homogeneous samples to avoid such limitation. Furthermore, we cannot affirm that all the physicians acquire telemedicine experience in current hospital settings or somewhere else. Finally, although the response rate (35.33%) of our study is higher than the average response rate in healthcare context, 20 future research could prepare more carefully in order to achieve a more satisfying sample size and response rate.
Contributions
The implementation of IT is rarely uniform across all groups within any given organization. On the contrary, IT is likely to influence diverse groups of people differently. 21 Consequently, only by understanding the important factors regarding an individual physician's telemedicine adoption decisions can hospitals effectively design appropriate supporting procedures to help physicians perform their jobs more effectively. Consequently, by further understanding the moderating influence of experience on the telemedicine adoption model, our study might shed light on how experience will influence physicians' telemedicine adoption decisions, and hospitals may thus formulate improved strategies to boost the adoption and use of telemedicine by all physicians, regardless of experience.
Footnotes
Disclosure Statement
No competing financial interests exist.