
Abstract
Introduction
The term “e-health” is defined by the World Health Organization as the use of information and communication technologies in health, 1 which encompasses telehealth, defined as the delivery of health services using information and communication technologies, specifically where distance is a barrier to healthcare. 2 Since the 1990s, telehealth has been growing worldwide, drawing important attention and receiving large amounts of investment from public and private sectors. Currently, it is impossible to quantify the number of projects and related services around the world. 3
For developing countries, the most important telehealth application is tele-assistance, which includes teleconsultation and telediagnostic tools to support health professionals and to extend specialized services to remote and isolated areas. 4,5 Teleconsultation can be described as a second opinion system that allows an information exchange between health professionals in order to discuss a clinical case when a specialist is not locally available. 6 It can be real time (with simultaneous interaction) or store and forward (in a time-independent basis). Low-cost technology and low bandwidth make store-and-forward teleconsultation the most frequent form of telehealth used in developing countries. 6
With a territorial size of 586,278 km2 and a population of 19 million inhabitants living in 853 cities (60% with less than 10,000 inhabitants), Minas Gerais is a Brazilian state with large social, economic, cultural, geographical, and infrastructural contrasts. Within this context, telehealth could improve the public healthcare system, bringing better medical care to the population living in remote municipalities. Since 2005, in Brazil and in particular in the state of Minas Gerais, the government has considered telehealth as an important tool to support primary care in remote areas. 7,8 Therefore, the state government sponsored the creation of the Telehealth Network of Minas Gerais (TNMG), a partnership of six public universities with the objective to support primary healthcare of remote municipalities in the state using teleconsultation and tele-electrocardiography. However, when compared with the high utilization of tele-electrocardiography, the use of teleconsultation has always been relatively low. This situation of underutilization of the teleconsultation services has been reported in other telehealth services around the world. 4,9 –11
Therefore, a full understanding of local factors affecting the use of telehealth has an important role for a successful implementation of the technology as well as its maintenance and sustainability. There is a lack of evidence about the specific factors that affect teleconsultation utilization rates in Brazil. As such, the objective of this study is to analyze factors associated with the utilization of the teleconsultation system of the TNMG, in order to learn how to overcome the barriers and introduce new practices to improve the utilization rates and then to fully achieve the benefits of telehealth.
Materials and Methods
A cross-sectional study was carried out, including all 229 municipalities connected to the TNMG teleconsultation system, from May to September 2009, when the number of municipalities using the system was constant and without any new municipal expansions. A new implementation process started in October 2009. The municipalities were distributed throughout the state, but 63% were located in low Human Development Index (HDI) regions, which was one of the criteria for implementation. The HDI was published by the United Nations Development Program as a composite statistic of life expectancy index, education index, and income index used to rank countries or cities. Other criteria were populations smaller than 10,000 inhabitants, availability of Internet connection, an active Family Health Program, and commitment of the municipal health management.
In this study, the 229 municipalities were classified in two groups (“users” and “nonusers”) according to the number of teleconsultations performed in the defined period. Municipalities with an average number of teleconsultations of one or more per month (average in the period) were classified as “users” and those with less than one teleconsultation per month as “nonusers,” using the definition adopted by the Brazilian Ministry of Health.
This study was divided into several stages.
Analysis of the Teleconsultations Performed
We analyzed the teleconsultation requests by the municipalities during this period. In order to allow a better comparison between services with different numbers of sites, three indicators were established: • the utilization percentage, defined as the percentage of the municipalities using the system, to evaluate the use distribution among the municipalities • the average number of teleconsultations per municipality per month, defined as the number of teleconsultations divided by the total number of municipalities with the system implemented, to evaluate the global average use • the average number of teleconsultations per user municipality per month, defined as number of teleconsultations divided by the number of municipalities using the system, to evaluate the average use among the effective users.
We also analyzed the responses of a survey with three questions generated automatically by the system when users received the teleconsultation response: 1. Did the teleconsultation avoid patient's referral? 2. Did the teleconsultation answer your question? 3. What is your level of satisfaction with the teleconsultation system?
These questions continuously monitor the efficiency of the activity, the quality of specialist responses and the user's general satisfaction with the system.
The Questionnaire
Structure of the questionnaire
We designed a questionnaire with questions divided in four groups: (1) characteristics of the municipality (related to work environment), (2) characteristics of the health professional (related to individuals), (3) factors related to the use of the teleconsultation system (related to the study object), and (4) satisfaction with the system (complementary information). Information was collected in October and November 2009. The questions in each group were as follows: • Characteristics of the municipality: population,
12
HDI,
13
geographical location, presence and number of primary care physicians, personal evaluation about difficulties to refer patients, referral distance (primary data), and using time of the teleconsultation system (database of the system). • Characteristics of the health professional: sex, age, marital status, profession, amount of time since graduation, specialty, primary care experience (years), and time interval that he or she had worked at the municipality. • Factors related to use of the teleconsultation system: Although these factors can be related to the telehealth center, to the operational system, or to the remote sites, in this study the questionnaire was applied only to professionals in remote sites, even though it included questions about their evaluation of factors related to the center and system. The questionnaire consisted of 27 questions about factors grouped into seven categories: institutional,
14
organizational,
15
–17
infrastructure,
6,14,18
technical,
6,19,20
socioeconomic,
19
–22
human,
17,23,24
and educational.
25
Answers were given in a 4- or 5-point scale. Details relative to the factors researched in the study, such as categories, description, reference site, and questions presented in the questionnaire, are shown in Table 1. Although the questionnaire consisted of 51 factors, eight factors could not be analyzed because they depended on prior use of the system, and 21 municipalities with no use were included in the study population. The alternative to this particular situation was to use two methods to analyze all the municipalities and factors: decision tree chi-squared automatic interaction detector (CHAID) and logistic regression. • Satisfaction with the system: The questionnaire included six questions: (1) What is your satisfaction degree relative to the telehealth service? (2) Do you consider the telehealth service specialists to have enough knowledge to attend your needs or questions? (3) Do you believe that the teleconsultation service has helped you solve your daily problems? (4) How do you evaluate your relationship with the telehealth service specialist? (5) Would you recommend the telehealth service to a friend or colleague? (6) Would you use this telehealth service again for other needs? Answers were possible in a 3- or 5-point scale.
Structure of the Questionnaire, Including Factors, Categories, and Reference Sites
Application of the questionnaire
A first version of the questionnaire was applied to three municipalities just to verify the feasibility of its application. After that, minor semantic mistakes were corrected without any modifications to the questionnaire's structure. The questionnaire was then applied to the 229 municipalities, classified into two groups: “users” and “nonusers.” Fifteen municipalities out of the 229 initially selected for the study were excluded because of the following reasons: refused to participate (n=5); absence of user professional in a municipality classified as user due to professional rotation (n=7); population much higher than the average in the study (n=2); and lack of secondary data (n=1). Consequently, of the remaining 214 municipalities, 137 were classified as users (64%) versus 77 as nonusers (36%), as shown in Figure 1.

Classification of the study population.
Questionnaires were conducted via telephone interviews with one health professional in each municipality. Special attention was given to apply the questionnaire to those professionals who had used or had not used the system according to the municipality grouping of users/nonusers. The questionnaire had to be applied to physicians as the system had been conceived to be used mainly by physicians; nurses were chosen only when physicians were not available. Considering that the median number of physicians in primary care was two, one was defined as the criterion for the number of professionals to be interviewed. For situations when there were two or more professionals, one was randomly chosen among those registered in the system, which had all the contact details.
First, a telephone call was made to the municipal health authority to ask for authorization to conduct the research. Five professionals refused to participate without further explanation, but almost all others answered the full questionnaire: only five missing answers were observed in the study. All participants signed the statement of informed consent.
Statistical Analysis
The normality of selected variables was evaluated using the Shapiro–Wilk test. The variables were described by mean and standard deviation, median and 25th–75th quartiles, or counts and percentages, as appropriate. The chi-squared test and Fisher's exact test were used to compare the proportions between the groups. In addition, the Mann–Whitney test was used to provide comparison between the means of the variables analyzed in the groups. A value of p<0.05 was considered significant.
Statistical analysis of the factors
Logistic regression was used to predict use of the teleconsultation system. Because logistic regression did not provide a stable and well-fitted model to study the factors associated with use of the teleconsultation system, a multivariable analysis using the Classification and Regression Tree algorithm with CHAID was used to analyze 214 municipalities and 43 factors. The variables to enter the tree were selected from univariate logistic regression models built with each of the variables of the study (p value ≤0.25). Another group was selected by its clinical importance: “period of time working in primary care,” “usefulness of the system,” “connection to Internet,” and “negative interference in the professional role toward patients.” 14,16,19 –21,23,24,26 The criterion adopted to stop the decision tree was a p value of <0.05 (chi-squared analysis), and the predictive accuracy was evaluated by risk summary. The risk estimative gives the proportion of cases classified incorrectly (AnswerTree version 3.0 User's Guide; SPSS Inc., Chicago, IL).
In order to perform the logistic regression for 193 municipalities and 51 factors, we created a new classification of the municipalities according to the number of teleconsultations performed in the defined period: “nonusers” were the excluded municipalities with no use of the system (21 municipalities with zero teleconsultation); the new “user” group included “minor users” (56 municipalities with one to four teleconsultations in the period) and “major users” (137 municipalities with five or more teleconsultations in the period). The whole classification of municipalities in the study is shown in Figure 1.
The same criteria described above were used to choose the variables to test in the model: p value of ≤0.25 and clinical importance (“period of time working in primary care,” “usefulness of the system,” “connection to Internet,” and “municipal administrative orientation”). 27 The model fit was checked by the Hosmer Lemeshow test.
We also used a descriptive analysis of the excluded 21 nonuser municipalities and a comparative analysis of these 21 municipalities and the remaining 193 municipalities.
SPSS version 17 (SPSS Inc., IBM, Armonk, NY), Answer Tree version 3.0 (STATCON, Witzenhausen, Germany), R version 2.10.1 (R Foundation for Statistical Computing, Vienna, Austria), and Excel™ (Microsoft, Redmond, WA) software were used for data analyses.
The project was approved by the Institutional Review Board of the Universidade Federal de Minas Gerais.
Results
Analysis of Teleconsultations Performed
From May to September 2009, 1,954 teleconsultations were performed by healthcare practitioners of the 229 municipalities. The utilization percentage was 51%; the mean number of teleconsultations per municipality per month and the mean number of teleconsultation per user municipality per month were, respectively, 1.71±1.5 and 3.32±2.2. In the same period, the analysis of the distribution of the municipalities according to the total number of teleconsultations performed showed that 93% of the municipalities had performed less than 20 teleconsultations (or less than four teleconsultations per municipality per month), as can be seen in Table 2.
Distribution of the Number of Municipalities According to the Number of Teleconsultations Performed from May to September 2009
The analysis of the survey showed that 78% of patient referral to specialists in other cities was avoided by the use of the system and that 74% of the users considered the questions totally answered by the TNMG professional. Fifty-six percent of the users reported being very satisfied and 39% reported being satisfied with the system (Table 3).
Questions, Answers, and Results of the Survey Performed from December 2008 to September 2009
Questionnaire Analysis
Characteristics of the municipality
The features of the 214 municipalities are described using the median, showing a population of 6,521 inhabitants, HDI of 0.680, time of system implementation of 18 months, presence of two physicians at primary care, and a referral distance of 80 km (Table 4). Most of the professionals interviewed (68%) said it was difficult to refer patients to specialized centers. Six municipalities (2.8%) did not have any physicians at primary care at the time of the interview.
Analysis of Features of Professionals and Municipalities by Median and Interquartile Range
Q25–Q75, interquartile range.
The study of the municipalities' location in the state regions showed that the majority of the “users” were located in the north (37.9%) and northeast (25.6%) of the state, regions with low HDI. There was no correlation between “number of teleconsultations” versus “population of the municipality” and between “number of teleconsultations” versus “how long the teleconsultation system was in operation.”
Characteristics of the health professionals
Of the 214 interviewed health professionals, 55.6% were female, 55.1% were single, and 48.1% were physicians, 50.0% were nurses, and 1.9% were dentists; 51.4% reported previous specializations in specific health specialties. They were generally young professionals (median age, 30 years old), at a median of 4 years after graduation, 54.2% with less than 3 years of work experience at primary care (10.3% with more than 10 years), and 66.3% with less than 3 years of working in the municipality (only 6.1% with more than 10 years) (Table 5). The majority of respondents (99%) reported being aware of the system, demonstrating that lack of knowledge was not a cause of nonuse.
Descriptive Analysis of the Characteristics of Healthcare Professional Participants in the Study
Analysis of the factors related to use of the teleconsultation system
• Analysis of the factors associated with the use of the system by decision tree CHAID. The multivariable analysis using the decision tree algorithm (CHAID) showed that the variable that best separated the first group (“users” and “nonusers”) was “sufficient training” (p=0.0015). The group of municipalities that had received enough training had the highest proportion of “users” (74.5%). This second group was separated by the variable “possibility of discussing clinical cases with other professionals out of teleconsultation system” (p=0.0192). The group of municipalities that did not have (or rarely had) the possibility to discuss clinical cases had the highest proportion of “users.” The model had a probability of 64% of correct classification (risk statistic=0.36). With this method there was a 64% chance of correct classification; therefore the users of the teleconsultation system should be those who received sufficient training and who rarely (if at all) had the possibility of discussing clinical cases out of the teleconsultation system (Fig. 2).
• Analysis of the factors associated with major use of the system by logistic regression. The multivariable logistic regression showed in the final model that “complexity of the system” (p=0.002) and “teleconsultation service helps to solve better the daily problems” (p=0.031) were associated with major use of the system. A municipality that evaluated the system as “simple/very simple” had higher odds of being a “user” (odds ratio [OR]=3.35; 95% confidence interval [CI], 1.59–7.09) than a municipality that evaluated the system as “complex/very complex.” As well, a municipality that evaluated that the teleconsultation service had helped a little/a lot to solve daily problems had higher odds (OR=4.37; 95% CI, 1.14–16.69) than a municipality that evaluated that the service had worsened/had not helped to solve daily problems.
• Descriptive analysis of the 21 municipalities with no use of the system. As we excluded 21 municipalities that had never used the system in order to accomplish the study by logistic regression, a descriptive analysis of these municipalities was performed. Regarding the professionals, they were mainly men (71.4%), married (61.9%), and physicians (95.2%). The analysis by median showed an age of 33 years (with 38.1% being older than 40 years of age), at 4 years after graduation, 33.4% with less than 3 years of work experience at primary care (23.8% with more than 10 years), and 61.9% with less than 3 years of working in the municipality. The features of the municipalities were also described using the median, showing a population of 5,361 inhabitants, HDI of 0.713, time of system implementation of 3 months, presence of two physicians at primary care, and a referral distance of 70 km.
• Comparative analysis between these 21 and the remaining 193 municipalities. This comparative analysis is shown in Tables 6 and 7. Tests for median comparison were not precise owing to the groups' great difference in size. The comparative analysis showed “sex” (p=0.009), “work experience at primary care” (p=0.010), and “training performed” (p=0.011) as significant variables.
• Analysis of user satisfaction with the system. The user satisfaction questionnaire analysis showed excellent results (Table 8). The descriptive analysis showed more than 90% satisfaction in both groups (major and minor users), and 100% of the people interviewed affirmed that they would use again the service.
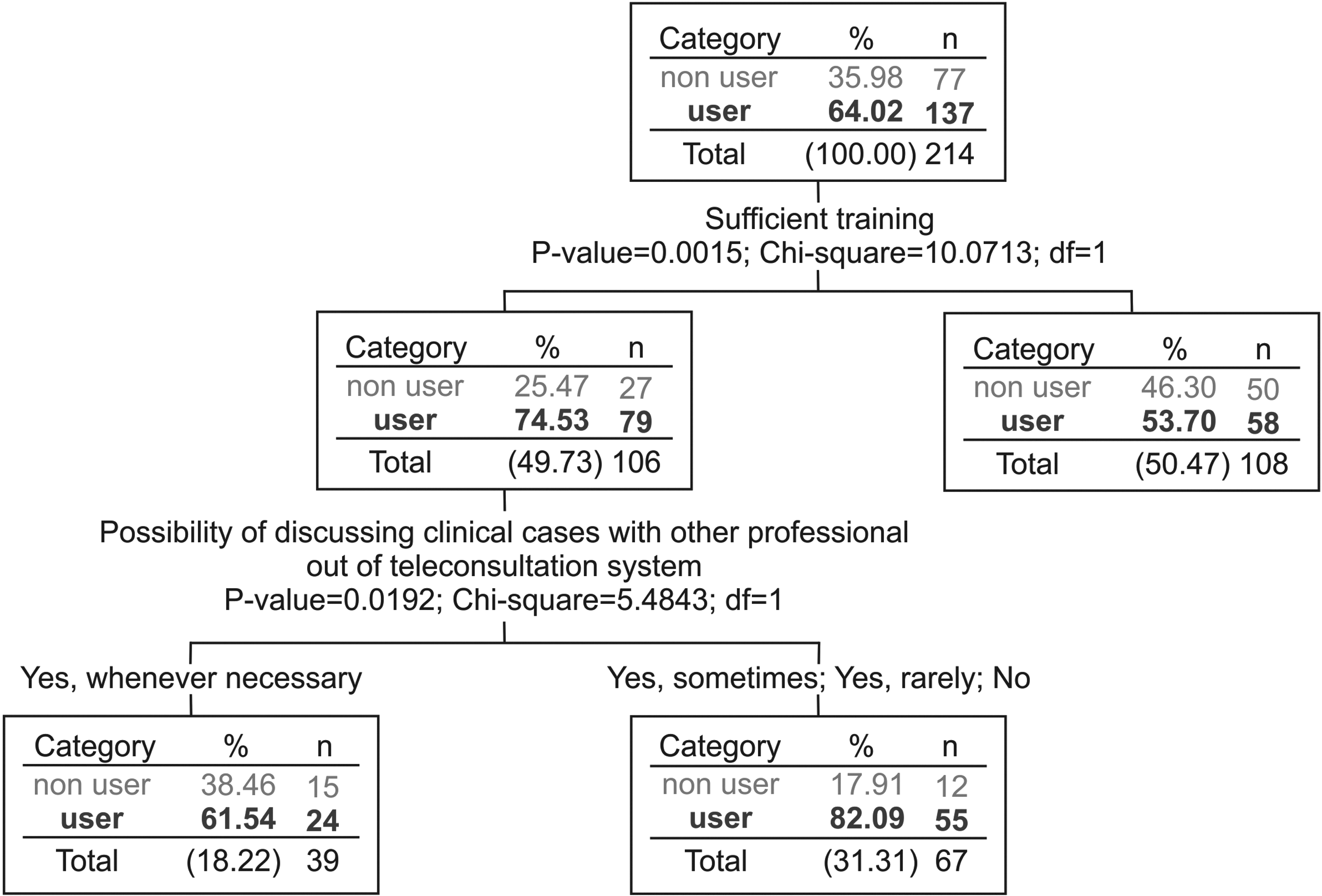
Multivariable analysis using the decision tree algorithm.
Comparative Analysis of the Features of the 21 Municipalities with No Utilization of the Teleconsultation System and the 193 Municipalities with Some Utilization in the Period of May–September 2009
Data are median values (interquartile range).
HDI, Human Development Index.
Comparative Analysis of the Features of Professionals Interviewed in the 21 Municipalities with No Utilization of the Teleconsultation System and in the 193 Municipalities with Some Utilization in the Period of May–September 2009
Data are percentages.
Descriptive Analysis of User Satisfaction with the Service
By chi-squared test, p=0.133.
The variable “Do you consider that the teleconsultation service helped you to better solve your daily problems?” was the only one in six variables analyzed with a significant value by Fisher's test (p=0.036, OR=3.99).
The questionnaire had five missing responses. From the group “major users,” two were related to the question “Do you consider the telehealth service specialists to have enough knowledge to attend your needs or questions?,” and two were related to the question “Would you use this telehealth service again for other needs?” From the group “minor user,” one missing response was related to the question “How do you evaluate your relationship with the telehealth service specialist?”
Discussion
The indicators defined in this study to analyze the teleconsultations performed demonstrated that the use of the teleconsultation system was lower than its potential, in agreement with findings from other authors. 3,4,9,11,28 Mars and Scott 11 found an average of 1.8±3.5 (median, 0.7) consultations per site per week (C/S/W) in a review of 77 telehealth services, which included the TNMG service with an average of 3.4 C/S/W (where consultation includes all telehealth activities [teleconsultation+tele-electrocardiography]). The result from the teleconsultation service of TNMG in this studied period shows an average of 0.38 C/S/W. The systematic use of the indicators of utilization, mean number of teleconsultations per municipality per month, and mean number of teleconsultation per user municipality per month could allow the comparison among different services.
The analysis of the characteristics of municipalities according to number of teleconsultations performed shows an important similarity, with almost all of them with low use of the system. According to Ohinmaa et al., 14 a teleconsultation system has to be incorporated into daily practice of health professionals to cause an impact on the local health system. In order to reach this difficult target, it is important to initially demonstrate the potential benefits of teleconsultations. In this sense, the analysis of the survey has yielded important conclusions: its use has an important potential to reduce patients' referral (78%); the telehealth clinical staff seemed to be adequate to the user's need, as only 8% of users related that the teleconsultation did not answer their question; and 95% of users were satisfied or very satisfied with the system. Therefore, the factors associated with the use of the system must be known in order to break the barriers, to improve its utilization, and to help incorporate it in the routine practice of primary care.
Teleconsultation, like other forms of e-health, has several problems related to its adoption by users and incorporation in daily practice of health practitioners. Several published studies have described the barriers and factors associated with e-health acceptance and adoption. The main factors can be summarized as follows: (1) lack of evidence of the impact of e-health in health indicators, 15,19,29 (2) need for changes in health management and work process, 15 –17,26,30,31 (3) users' perception of usefulness, benefits, and limitations, 19 –21,26 (4) lack of evidence of cost-effectiveness and sustainability, 14,15,22,29,32 (5) low acceptance of technology, 19 –21,26,31,33,34 (6) deficiency in local infrastructure, 6,14,18 (7) ethical and legal aspects, 3,19,26,28,35 (8) human factors, related to users' perceptions about e-health, 17,23,24,26 (9) lack of adequate specialist clinical staff, 4,6,36 and (10) lack of large-scale studies to evaluate the adoption of e-health. 4,17,35 Some models, theories, and concepts from different areas have been used to study the adoption of telemedicine by users, such as the Technology Acceptance Model, 19,21 Theory of Planned Behavior, 21,24 Theory of Interpersonal Behavior, 24 Unified Theory of Acceptance and Use of Technology, 18,26,33,37 Readiness, 16,20 and Diffusion of Innovations Theory. 38,39
In this study, the characteristics of healthcare professionals (physicians and nurses) demonstrate the high turnover of these categories in Minas Gerais, as 66.3% had been working in the municipality for less than 3 years and only 6.1% for more than 10 years. In addition, they suggest the usefulness of a teleconsultation system in their routine practice, considering that the potential users were not able to solve all the clinical problems of the patients because of their youth, short interval after graduation, and working time experience at primary care. These features and the result of the comparative analysis between the 21 municipalities with no use of the system and the 193 municipalities with some utilization, which showed in the descriptive analysis more experienced professionals as nonusers and the variable “work experience at primary care” as significant (p=0.010), suggest that use of the teleconsultation system is associated with a health professional's necessity. 16,19,20,26,40 –42 These studies suggest that the social factor “utility of the system” will have a strong association with the use of telehealth systems. This correlation between use and utility is supported by the fact that the majority of users are located in remote regions with low HDI, where the public health system is deficient owing to the difficulties in retaining experienced specialists. Furthermore, it is almost the only alternative for medical assistance.
Organizational factors are also cited as relevant to the adoption and incorporation of telehealth. 14 –17,19,20,30,31,35 Considered as a new manner of working, telehealth requires detailed planning, new protocols, and monitoring. “Sufficient training,” an organizational factor, was the most relevant factor in this study. Telehealth training must include motivation, discussion about its benefits, barriers, risks, ethical and legal aspects, and necessity of changes in daily practice, according to the Readiness model. 16,20 Adequate training was also a relevant factor in other studies. 21,27,31,42,43 According to the Technology Acceptance Model theory studied by Hu and Chau, 42 user training is important to solidify users' perception of usefulness of the system. As the main objective of a teleconsultation system is to offer the possibility of clinical case discussion, it could be expected that when it naturally occurs, the system would not be useful.
The perceived ease of use has been studied by several authors with different results, 21,27,31,33,34 but the simplicity and adequacy of the system with local Internet conditions should be considered as success factors. In this study, 93% of the interviewed professionals affirmed using computers and the Internet in their private life and work. This fact likely facilitates the adoption of the system. The perceived usefulness is the strongest factor described in the literature as associated with the use of telehealth. 16,19 –21,33,40,41 In this study, the questionnaire had two questions related to this factor: “How would you assess the usefulness of the system in your work daily practice?” applied to all the 214 municipalities, and “Do you consider that the teleconsultation service has helped you to better solve your daily problems?” applied to 193 municipalities. The descriptive analysis showed that, on average, 90% of the interviewers, independent of being users or nonusers, considered the system useful or very useful, demonstrating a lack of association of this factor with system utilization. Additionally, the second question (“Do you consider that the teleconsultation service has helped you to better solve your daily problems?”) remained in the logistic regression final model (p=0.038, OR=3.99). The perception of the utility of the system is related with the users' necessities fulfillment, 14,44 showing the importance of planning a telehealth service according to users' expectations. These results are according to the Technology Acceptance Model and other theories, where perceived usefulness and perceived ease of use are the most important variables.
In this study, human factors, considered as a negative interference of using a second opinion system in the professional role facing patients, community, and colleagues, were not associated with use of the system, as were also infrastructure factors (connection to Internet, equipment availability). The great majority of the interviewers declared they knew of and agreed with the benefits of telehealth. The lack of defined features of both groups (“users” and “nonusers”) suggests that the system would not still be incorporated in daily practice.
Limitations of the Study
The main limitation was the similarity of the majority municipalities studied regarding the system's usage pattern, causing difficulties for their classification into groups. This situation was due to two factors: a change in the usage pattern of the system during the study period, with an increased number of monthly teleconsultations requested, and the short period of time defined for the analysis.
In 2009 the Telehealth Network implemented several corrective actions to improve the use of the system. Several municipalities changed their status from real nonusers (with no utilization of the system) to users with irregular use, without defined characteristics of a condition or other. It was also not possible to amplify the period of the study to some months before May 2009, as it was an implementation period of the system and owing to the high turnover of the remote professionals that occurred by the end of 2008 after municipal elections.
Conclusions
Teleconsultation systems are constantly described with enormous benefits, but the numbers are usually lower than expected. The present study intended to demonstrate the factors associated with the low use of the teleconsultation system of the TNMG to collaborate in achieving the success of telehealth. As a conclusion, the main factors in the state of Minas Gerais needed to improve the use of a teleconsultation service are to attend remote municipalities, to support young professionals, to offer efficient training, to use a simple system, and to meet the real needs of the users. The results also showed the potential of teleconsultation to reduce referrals and to help solving routine problems of health professionals in primary care. Considering this potential, solutions to increase the utilization must be sought from scientific observations to collaborate in the adoption and diffusion of this new work practice.
Footnotes
Acknowledgments
This study has no specific funding. The Telehealth Network of Minas Gerais is mainly funded by the State Government of Minas Gerais, by its Health Department (the Secretaria de Estado da Saúde de Minas Gerais), but also by the Ministry of Health and the Ministry of Science and Technology, and the Brazilian research agencies Conselho Nacional de Desenvolvimento Científico e Tecnológico, Financiadora de Estudos e Projetos (Projeto SIGTEL, Convênio 01.10.0717.00), and Fundação de Amparo à Pesquisa de Minas Gerais (PROJETO REDE 61/11). A.L.R., M.B.A., and L.S. received grant from Conselho Nacional de Desenvolvimento Científico e Tecnológico.
Disclosure Statement
No competing financial interests exist.