
Abstract
Introduction
The prevalence of asthma is consistently increasing, and it is now estimated that 300 million people worldwide are affected by the disease. 1 Long-term control of asthma requires appropriate medication, patient education, and adherence with the prescribed therapy. It has been shown that patient adherence with asthma therapy can be as low as 50%, and nonadherence can lead to poor asthma control and increased symptoms. 1 One of the primary reasons for poor adherence is forgetfulness of medications and treatments. 2,3 Delayed reporting of asthma symptoms and exacerbations is associated with morbidity and the need for emergency care. 4,5
Telemedicine is typically described as “personalized healthcare over a distance.” 6 Broadly, there are two forms of telemedicine: one that occurs in real time, such as videoconferencing, and one that occurs asynchronously, such as reporting of glucose monitoring results or text messaging reminders to patients. Although telemedicine has been used for over 20 years in the management of chronic diseases, evidence that it is effective in altering outcomes is weak. 7 With respect to asthma, it is believed that telemedicine can address specific challenges such as self-monitoring, adherence to medications, avoidance of triggers, and facilitating timely access to healthcare advice. 8,9 Although many individual studies have suggested that telemedicine interventions can improve the outcomes of patients with asthma, 10 –12 a recent Cochrane review of the literature concluded that there is no evidence that telemedicine results in a clinically important impact. 13
The purpose of this systematic review of the literature and meta-analysis was to determine the effectiveness of telemedicine in relieving symptoms in patients with asthma.
Materials and Methods
Literature Search Strategy
This systematic view and meta-analysis was conducted in accordance with PRISMA guidelines. 14 A search was conducted of the Medline, Cochrane, EMBASE, and Google Scholar databases until December 31, 2013 using combinations of the following key words: “asthma,” “telemedicine,” “telehealth,” “e-health,” “mobile health,” “Internet,” “telecommunication,” “telemanagement,” “remote,” and “short message service.” Reference lists of relevant studies were hand-searched.
Selection Criteria
Inclusion criteria were as follows: (1) randomized controlled trial; (2) participants had a diagnosis of asthma; (3) the majority of the patients were ≥18 years of age; (4) male and/or female gender; and (5) the intervention involved any format of telemedicine such as text messaging, telephone, Internet, or mobile phone. Exclusion criteria were as follows: (1) participants had a diagnosis of a lung disease other than asthma; (2) the study did not evaluate changes of asthma symptoms; (3) non-English publication; and (4) the publication was a letter, comment, editorial, or case report.
Study Selection, Data Extraction, and Quality Assessment
Studies were identified using the search strategy by two independent reviewers. A third reviewer was consulted when there was uncertainty regarding eligibility, and the decision for inclusion was made by consensus. Data extraction was also performed by two independent reviewers, and a third reviewer was consulted for any uncertainties. The following information was extracted from studies that met the inclusion criteria: name of the first author (reference), year of publication, study design, demographic data of subjects, description of telemedicine intervention, and changes of asthma symptoms.
The Delphi list was used to assess the quality of the included studies. 15 The quality assessment was performed by the independent reviewers, and a third reviewer was consulted for any uncertainties.
Outcome Measures and Statistical Analysis
The primary outcome studied was change of asthma symptoms, which was investigated as asthma symptom score change. The standardized mean difference with 95% confidence interval was calculated for the outcome in the intervention group compared with the control group. Heterogeneity among the studies was assessed by the Cochran Q and the I 2 statistic, respectively. For the Q statistic, p<0.10 was considered to indicate statistically significant heterogeneity. The I 2 statistic indicates the percentage of the observed between-study variability due to heterogeneity rather than chance, with the following suggested ranges: no heterogeneity, I 2=0–25%; moderate heterogeneity, I 2=25–50%; large heterogeneity, I 2=50–75%; and extreme heterogeneity, I 2=75–100%. If either the Q statistics (p<0.1) or I 2 statistic (>50%) indicated heterogeneity exists between studies, a random effects model of analysis was used (DerSimonian–Laird method). Otherwise, a fixed effects model (Mantel–Haenszel method) was used. The pooled Hedges's g of the outcome was calculated, and a two-sided p value <0.05 was considered statistically significant. All statistical analyses were performed using the statistical software Comprehensive Meta-Analysis, version 2.0 (Biostat, Englewood, NJ).
Results
Literature Search
The results of the literature search are summarized in Figure 1. In total, 813 articles were identified in the initial search after duplicates were removed, and 759 were subsequently excluded, leaving 54 for inclusion in the full text review. After full text review of the 54 studies, 43 were excluded (Fig. 1), and thus 11 were included in the qualitative synthesis. Subsequently, five studies were found not to be suitable for inclusion in the meta-analysis.
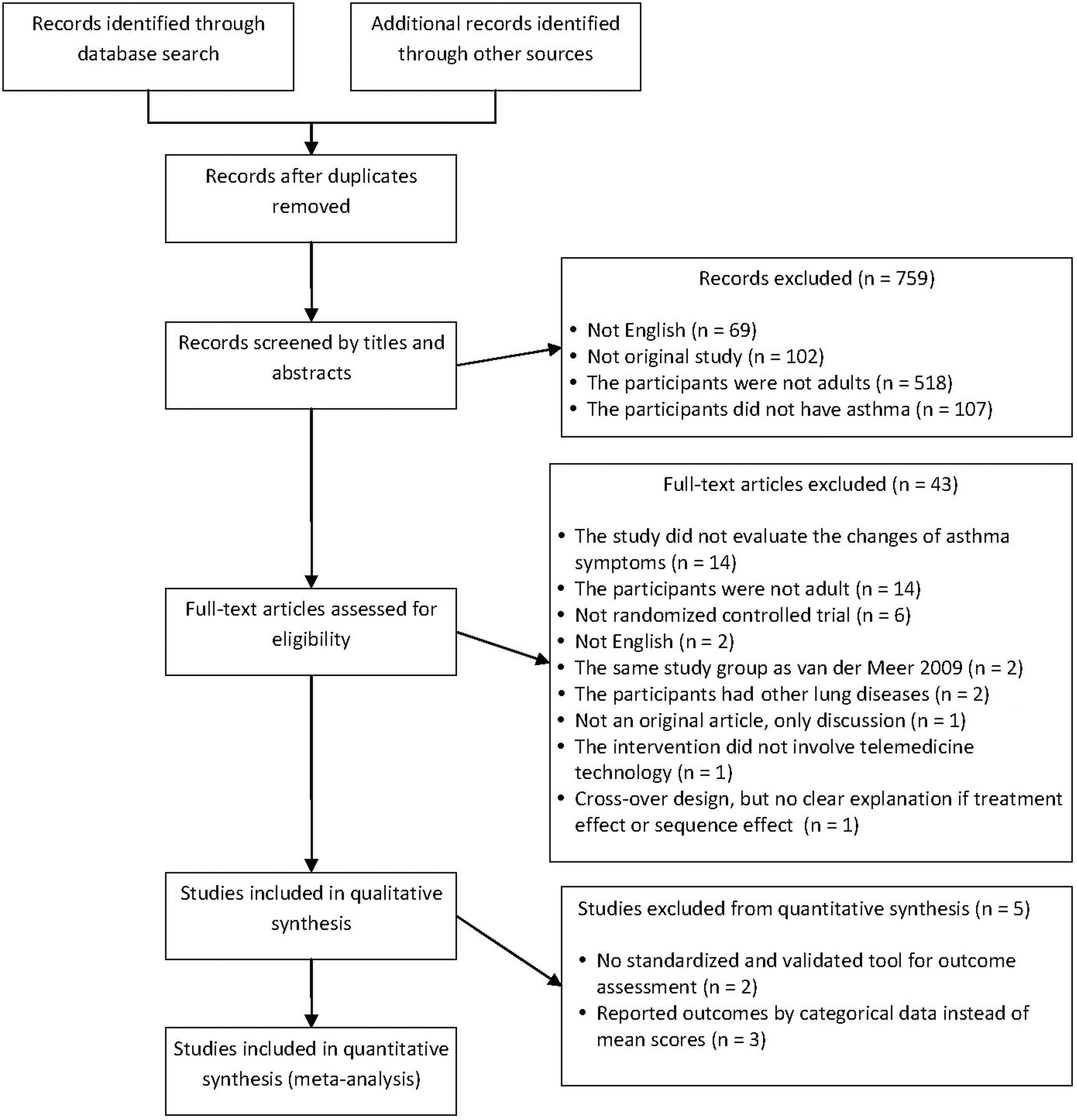
Flowchart of study selection.
Study Characteristics
In total, 11 studies were included in the qualitative synthesis, 16 –26 and the study characteristics are summarized in Table 1. Among the 11 studies, there were 1,460 patients in the intervention groups and 1,349 patients in the control groups, and the total numbers of participants ranged from 12 to 481 in the intervention groups and from 12 to 487 in the control groups. The mean age of patients ranged in the intervention groups from 34.4 to 54.6 years and in the control groups ranged from 30.7 to 56.4 years. The treatment duration ranged from 0.5 to 12 months.
Summary of the Studies Included in the Systematic Review
Data are amean±standard deviation, bmean (range), or cmedian (range) as noted.
Responses based on 208 intervention and 222 usual-care participants at baseline and 481 intervention and 487 usual-care participants at final visit.
NA, no data available, SMS, short message service.
Internet-based and telephone-based were the most commonly used interventions (Table 2). Four studies used the Asthma Control Questionnaire (ACQ) to measure outcomes, and other studies used the Asthma Therapy Assessment Questionnaire, North of England Asthma Symptoms Scale, and Short Questionnaire (Table 2).
Summary of Study Outcomes
Data are amean±standard deviation, bchange (standard error), cmedian, dchange (95% confidence interval), or emean as noted.
Responses based on 208 intervention and 222 usual-care participants at baseline and 481 intervention and 487 usual-care participants at final visit.
ACQ, Asthma Control Questionnaire; ATAQ, Asthma Therapy Assessment Questionnaire; NA, no data available; NEASS, North of England Asthma Symptoms Scale; Short Q, short questionnaire; SMS, short message service.
Outcome Evaluation: Change of Asthma Symptom Scores
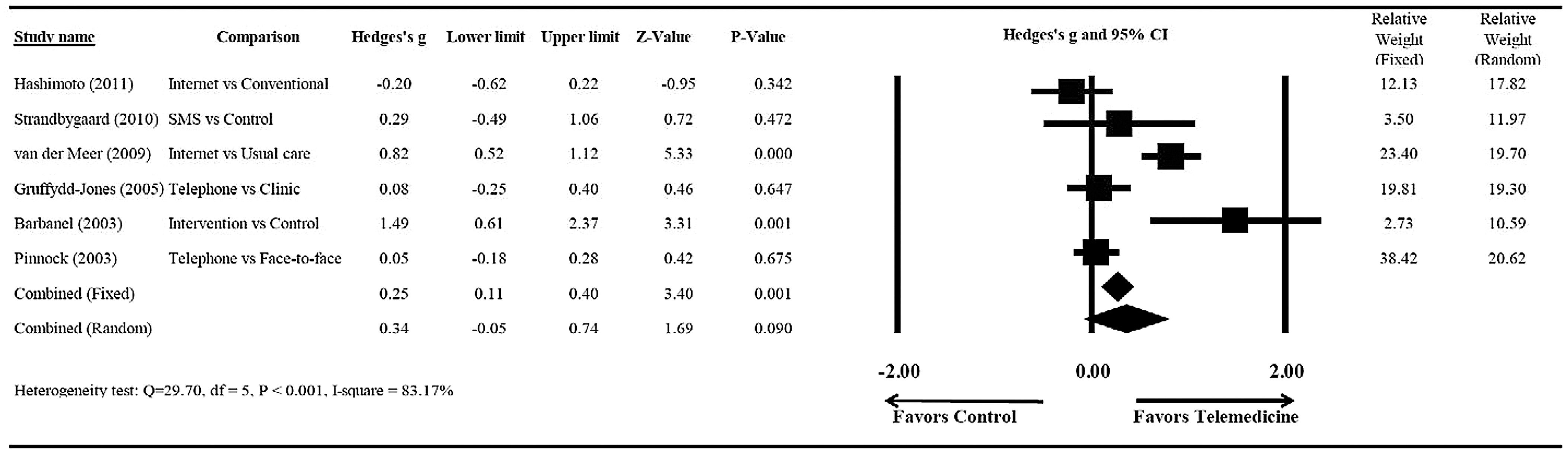
For studies that used the ACQ, the asthma symptom score change for the intervention groups ranged from −0.87 to 0.26, and the asthma symptom score change of the control groups ranged from −0.62 to 0.12. Five studies were not included in the meta-analysis, 18,19,21,22,24 and the reasons for their exclusion are shown in Figure 1.
There was significant heterogeneity when data from the six remaining studies 16,17,20,23,25,26 were pooled (Q=29.70, df=5, p<0.001, I 2=83.17%); therefore a random effects model of analysis was used (Fig. 2). The meta-analysis including these six studies revealed no significant difference in asthma symptom score change between the telemedicine and control groups (pooled Hedges's g=0.34, 95% confidence interval=−0.05 to 0.74, Z=1.69, p=0.090).
Sensitivity Analysis
The results of the meta-analysis using the leave-one-out approach to assess the sensitivity of the fixed effects model and random effects model are summarized in Figure 3. The direction and magnitude of the pooled estimates did not vary considerably, indicating that the meta-analysis had good reliability. However, in the fixed effects model removal of the study by van der Meer et al. 20 caused the pooled Hedges's g to become nonsignificant (p=0.352) (Fig. 3A). In the random effects model removal of the study by Hashimoto et al. 16 caused the pooled Hedges's g to became significant (p=0.040) (Fig. 3B).

Publication Bias and Quality Assessment
There was no significant evidence of publication bias for the asthma symptom score change by Egger's test (t=0.660, df=4, p=0.273) (Fig. 4). Quality assessment findings are summarized in Table 3. None of the included patients was blinded to care, and only two studies had blinded care providers and outcome assessors. 19,21

Funnel plot evaluating publication bias of asthma symptoms score change for all studies. Open circles represent observed studies. The open rhombus represents the observed combined effect size.
Summary of Quality Assessment
Discussion
The results of this meta-analysis indicated no difference in outcomes as measured by asthma symptoms score change between patients managed with a telemedicine intervention and control groups. Although the results revealed no significant different between the telemedicine intervention and control groups, there are some points that should be considered. None of the included studies applied a double-blind design. As some authors have pointed out, it is impossible to blind patients and their caregivers, which introduces the potential for bias. 23,26 The longest length of intervention among the included studies was 12 months, and the shortest was only 0.5 months, which can affect the results of individual studies and comparisons of them. Although patients who received telemedicine interventions had no significant improvement compared with the control groups, their knowledge and attitude may have been changed by the intervention. This point is illustrated by the study of Zurovac et al., 27 in which the investigators assessed immediate postintervention effects and effects at 6 months after the intervention. The analysis showed that the performance of the participants continued to improve after 6 months postintervention. In addition, some components were not significantly different from baseline at the immediate postintervention follow-up but were significantly different at 6 months postintervention.
Advantages of telemedicine include home care of patients with video- or Internet-based conferencing and education, reminders for compliance with therapies, monitoring to allow earlier detection of disease, continuity of care, and reduced costs. 28 These advantages have been seen with ambulatory care 29 and in the management of chronic diseases such as asthma. 9,30 Telemedicine interventions have been shown to increase adherence with antiretroviral therapy and smoking cessation, 28 reduce the risk of emergency department visits and hospitalizations in patients with chronic obstructive pulmonary disease, 31 and even improve healthcare workers' adherence with malaria treatment guidelines. 27
Several studies have shown that telemedicine interventions can improve outcomes in patients with asthma. For example, van Gaalen et al. 10 found that Internet-based self-management support that included weekly asthma control monitoring and treatment advice, online group education, and communication with a respiratory nurse resulted in improved asthma-related quality of life and asthma control, and the improvements persisted after the support ended. Van Sickle et al. 11 reported that weekly e-mail reports and access to online data that summarized remote monitoring of inhaled bronchodilator frequency were associated with improved asthma control and decreased daily symptoms. Araújo et al. 12 found that Web-based asthma management was preferred by patients over standard paper-based self-management and that although asthma outcomes were similar, the quality of the data were improved.
Despite a large volume of literature indicating that telemedicine interventions can improve outcomes in patients with asthma, reviews of the literature have indicated little impact. A 2011 Cochrane review by McLean et al., 13 which identified 21 randomized controlled trials, concluded that there was no evidence that telemedicine had a clinically important impact on the quality of life of asthma patients, but the interventions may have the potential to reduce the risk of hospital admissions, particularly for patients with severe asthma. A more recent review of telehealthcare in general by McLean et al., 32 which included 80 systematic reviews, found large variation in the length of studies and number of participants and that many studies did not adequately describe the interventions, making it difficult to distinguish the effects of technological and human or organizational factors. The authors concluded that the greatest benefits of telemedicine will likely be for patients with the highest risk of serious outcomes. Kitsiou et al. 33 also examined systematic reviews and meta-analyses of home telemonitoring interventions for patients with chronic diseases and noted that large numbers of studies have intrinsic methodological problems, which limits interpretation of the results, and the overall quality of the studies has not improved over time.
In some cases, the individuals who investigate the effectiveness of telemedicine may be specialized in information technology but may not be familiar with methods of clinical evaluation. Five studies that were included in the current systematic review were not eligible for the quantitative analysis because they did not use a standardized and validated evaluation tool for asthma, such as the ACQ or Asthma Therapy Assessment Questionnaire, which is recommended in the guidelines for asthma management, 1 or they reported categorical data rather than mean scores. Some of the studies that were not included in our meta-analysis indicated telemedicine interventions were useful, whereas others indicated that they were not useful. Prabhakaran et al. 18 used short messaging service support and found no differences in the number of nebulizer treatments, emergency department visits, or reduction in admission rates between the intervention and control groups, although the number of patients in each group was relatively small (n=60). Vollmer et al. 22 used an automated telephone outreach system, and although the program was well received by patients and healthcare providers, it did not improve asthma outcomes. On the other hand, Rasmussen et al. 24 found that an online interactive monitoring tool managed by physicians resulted in improved asthma control, as measured by quality of life and lung function, compared with specialist monitoring or general practitioner monitoring. Clark et al. 21 found that a telephone counseling intervention improved functioning, quality of life, and healthcare utilization in women with asthma. Bender et al. 19 reported that an interactive voice response intervention increased adherence to inhaled corticosteroid treatment and improved Beliefs in Medications Questionnaire scores.
Although the results of this study did not show that telemedicine interventions improved asthma symptoms scores, to conclude that telemedicine interventions provide no value is simplistic. Nor can it be concluded that the results suggest telemedicine and in-person care are clinically equivalent. All patients in the intervention and control groups received conventional physician office visits. However, patients in the intervention groups also received some form of telemedicine intervention. Thus, no conclusions can be drawn with respect to “telemedicine only” and “conventional physician only” care. Despite the findings, we do not believe that it can be said telemedicine offers no value. There may be benefits such as reducing the number of acute asthma exacerbations, emergency department visits, and hospitalizations. These are factors not evaluated in the current study. Thus, we believe the exact benefits of telemedicine are undetermined.
Study Limitations
There are limitations of this study that need to be considered. The definition of telemedicine encompasses a wide range of technologies and interventions. This extreme heterogeneity makes a comparison of different studies and a synthesis of the results of different studies very difficult. In addition, telemedicine interventions can range from automatic interventions based on computer algorithms to personalized responses from physicians. Furthermore, results can be affected by the different outcome measures used in different studies. However, our meta-analysis only included studies that measured outcomes with standardized and validated tools.
Conclusions
Telemedicine interventions do not result in an improvement of asthma symptom scores. However, the exact benefits of telemedicine with respect to asthma remain to be determined. For example, factors such as reduction in the number of acute asthma exacerbations, emergency department visits, and hospitalizations were not evaluated in the current study. In addition to the evaluation of clinical effectiveness, an economic analysis of telemedicine on asthma management is necessary before defining health policy. Policy makers will have to consider the ethics, complexity of telemedicine devices, and the ability of the telemedicine devices to be integrated with existing systems.
Footnotes
Acknowledgment
This study is supported by the National Science & Technology Huimin Program (2013GS410101), Major Program of Science & Technology of Henan Province (121100111100), Youth Foundation of the first Affiliated Hospital, Zhengzhou University, and Innovation Scientists and Technicians Troop Construction Projects of Henan Province (144100510017).
Disclosure Statement
No competing financial interests exist.