
Abstract
Introduction
Telemedicine is designed to increase access to specialist care, especially in settings distant from tertiary-care centers. One of the more established telemedicine applications in hospitals is the tele-intensive care unit (tele-ICU). 1 Typically, tele-ICU systems provide comprehensive monitoring of critical care patients on a continuous basis by an off-site team of clinical specialists. 2 Through audio, video, and electronic links, the off-site “hub” clinicians have access to patient data to detect clinical instability or abnormalities in real time and coordinate with local clinicians to make patient care recommendations. 2 Systematic literature reviews examining the impact of tele-ICU on patient outcomes and cost have reported mixed results. 2 –6 In contrast, a systematic literature review focused on staff acceptance of tele-ICU suggested that its reception is generally positive. 7 However, the majority of the studies in that review were from unpublished abstracts. The few published research articles in the review reported ratings on a handful of items by small samples of clinicians.
Thus, with tele-ICU, a commonly used telemedicine application, we undertook a study focused on assessing staff acceptance. In doing so, we used a survey instrument that gathered perceptions on multiple facets of tele-ICU use. Furthermore, we administered it to clinical and administrative staff at multiple hospitals that had implemented a tele-ICU system connected to a single hub control site operated by Avera eCARE in Sioux Falls, SD. Doing so yielded a large number of respondents, which permitted us to examine multiple factors related to varying user perceptions. In addition, we conducted interviews at many of these hospitals to gain a deeper understanding of factors affecting staff perceptions of tele-ICU services.
Materials and Methods
Following a review of the literature, we designed a 24-item survey to collect perceptions on each of the six domains in a framework for assessing telemedicine 8 : clinical outcomes, technical acceptability, health system interface, costs and benefits, access, and patient/provider acceptability.
The Avera eCARE telemedicine hub site provided us with a list of primary contact e-mails at all hospitals that had implemented tele-ICU, and a survey link was sent electronically to that single contact person. These representatives were asked to share the survey with both clinical and administrative staff in their hospital and to encourage those staff members to complete the survey. In all, 145 respondents indicated they were familiar with the tele-ICU service in use at their hospital and completed the survey. The sample included respondents from 28 of the 33 hospitals that had implemented the tele-ICU service. Ten were prospective payment system (PPS) hospitals, and 18 were critical access hospitals (CAHs).
Statistical differences between groups of respondents were tested using a generalized linear model procedure to control for multiple responses from individual hospitals, run on SAS version 9.3 software (SAS Institute, Cary, NC).
Phone interviews and site visits were conducted with a sample of 24 clinicians and 16 administrators at 13 rural hospitals that used this tele-ICU service. All interviews were recorded and subsequently transcribed. De-identified transcripts were coded for themes by three of the co-authors who discussed differences until agreement was met.
Protocols for the survey and interviews were approved by the University of Iowa Institutional Review Board (approval numbers 201111717, 201203722, and 201302760).
Results
Survey Respondents
An initial question asked the 145 survey respondents to identify their primary role according to seven response options. Respondents self-identified as “nurses” (n=66, 45.5%), “administrators/management” (n=49, 33.8%), providers (n=17, 11.7%), including 15 “physicians” and 2 “nurse practitioners or physician assistants,” “pharmacists” (n=8, 5.5%), “other roles with regular patient contact” (n=4, 2.8%), or “other roles with infrequent patient contact” (n=1, 0.1%). The answers to this question were then used for skip logic in portions of the survey, and a subset of questions was only asked of respondents who had a specific clinical role (i.e., nurse, nurse practitioner or physician assistant, or physician).
Survey Responses
The majority of survey items, shown in Table 1, used a six-level agree/disagree response scale with a “don't know/not applicable” option. The 17 items at the top of Table 1 were asked of all respondents. The five items at the bottom of Table 1 were asked of nurses, nurse practitioners or physician assistants, and physicians—respondents who are most likely to have direct experience interacting with the tele-ICU system. To facilitate comparisons, the rows in each section are ordered by percentage of respondents who indicated “strongly agree.”
Distribution of Responses to Agree/Disagree Items on the Tele-intensive Care Unit Survey
Data are number (%).
ICU, intensive care unit.
In addition to the items shown in Table 1, the survey included an item that asked how frequently the tele-ICU technology works well, and the responses were 28.0% “always,” 42.7% “usually,” 9.8% “frequently,” 8.4% “sometimes,” 2.8% “rarely,” 0% “never,” and 8.4% “not applicable/don't know.”
Respondents who indicated that they were a nurse, nurse practitioner or physician assistant, or physician were asked to indicate how often they interact with tele-ICU, and the responses were 14.5% “frequently,” 53.0% “sometimes,” 32.5% “rarely,” and 0% “never.”
Survey Comparisons
A series of analyses were conducted to compare subgroups of respondents. The first three subgroup analyses split respondents into categories based on individual characteristics: (1) respondents who had clinical roles versus those who had administrative/managerial roles; (2) nurses versus providers (i.e., physicians, nurse practitioners or physician assistants); and (3) nurses and providers who indicated they interacted with tele-ICU “frequently” compared with those who interacted with it “sometimes” or “rarely.” The remaining subgroup analyses split respondents into categories based on characteristics of their hospital: (4) respondents who worked in a CAH versus PPS hospital; (5) respondents at hospitals that had more tele-ICU patient-days per month versus those with less; and (6) respondents at hospitals that had implemented tele-ICU earlier versus those that had implemented it more recently.
Providers and nurses differed statistically significantly on three survey items. As shown in Figure 1, providers were significantly (p<0.05) more positive than nurses about several facets of the tele-ICU service, including that it makes caring for patients in the ICU less burdensome, that tele-ICU utilization is encouraged and supported by their hospital administration, and that it helps with recruitment and retention of healthcare professionals in their hospital.
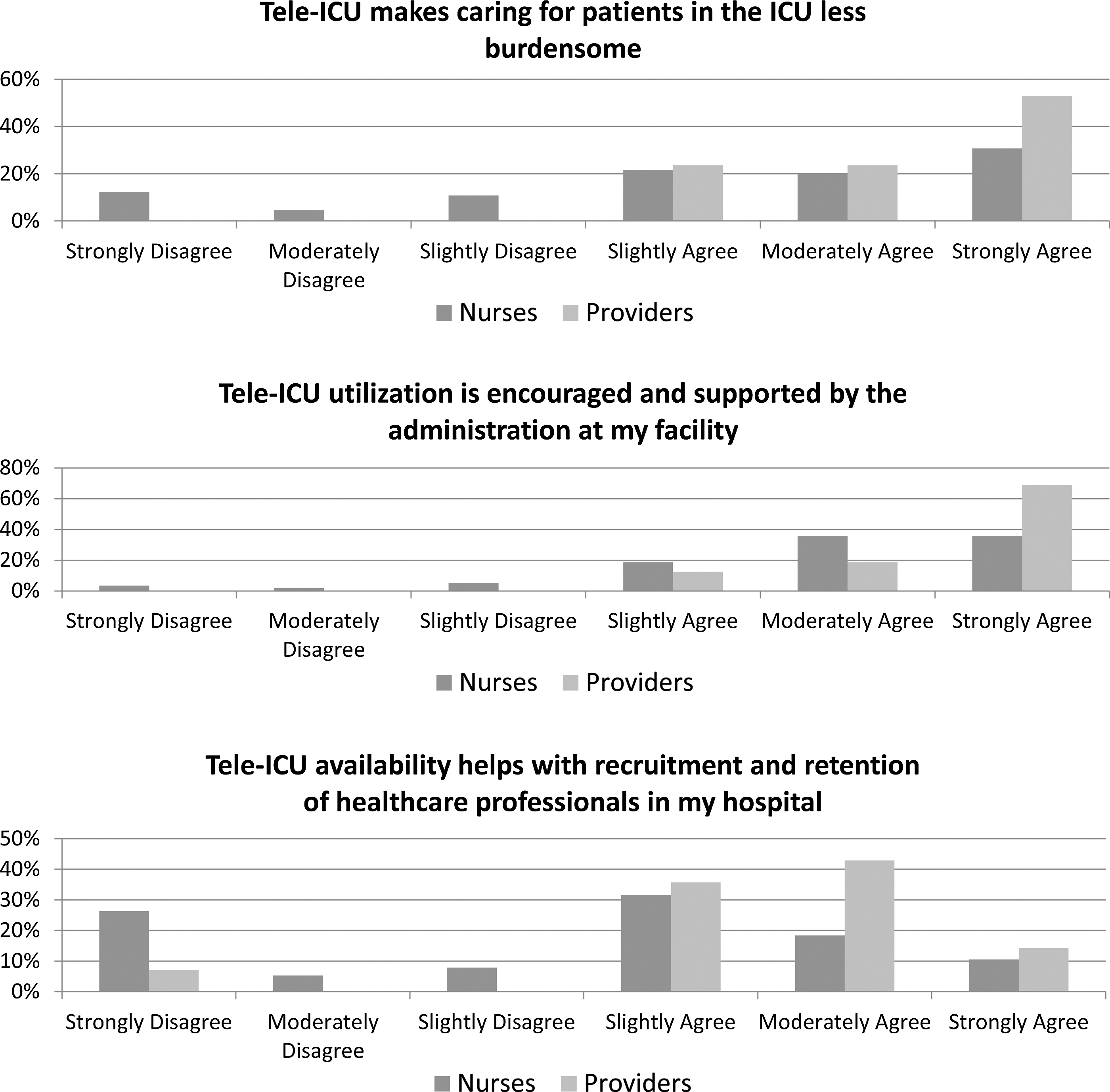
Tele-intensive care unit (tele-ICU) survey responses for items with significant differences between nurses and providers.
Analyses found no significant differences in comparisons between CAHs and PPS hospitals or between clinical and administrative/managerial respondents. However, analyses for the other three comparisons yielded significant differences, as summarized in Table 2.
Percentage of “Strongly and Moderately Agree” Responses and Comparisons Between Groups on the Tele-intensive Care Unit Survey
ICU, intensive care unit; pt-day, patient-day.
As shown in Table 2, analyses indicated that clinicians who said they used tele-ICU frequently were statistically significantly (p<0.05) more positive in their responses on 14 survey items than were clinicians who used it sometimes or rarely.
In addition to respondents' estimation of how frequently they use tele-ICU, data on monthly patient-days of tele-ICU service for each hospital, obtained from the hub control site, were analyzed. Because of highly skewed data for PPS hospitals, only CAHs are reported here. Average monthly tele-ICU patient-days for CAHs ranged from 0 to 45 patient-days, with the median around 1 patient-day per month. As shown in Table 2, analyses indicated that respondents at hospitals averaging more than 1 patient-day per month of tele-ICU use were statistically significantly (p<0.05) more positive in their responses on 12 survey items than were respondents at hospitals that had used the tele-ICU services less.
Analysis also examined the relationship between survey responses and time since tele-ICU implementation. Implementation of tele-ICU services had been phased in over the past 7 years. As shown in Table 2, respondents at hospitals that had implemented tele-ICU more than 3 years previously were significantly more positive in their responses on nine items than were those at hospitals that had implemented it more recently.
Interview Themes
Interviews with hospital administrators and clinical personnel at half of the hospitals that implemented tele-ICU yielded four commonly expressed themes.
Differing views as a factor of utilization
Utilization was fairly low in most CAHs. Consistent with the survey findings, interviewees at hospitals with higher tele-ICU utilization were likely to express more positive views of the service. In contrast, low CAH utilizers were more likely to have a negative view of the service overall and to suggest that tele-ICU was a burden on nurses. For example, the amount of work related to connecting tele-ICU equipment was a source of frustration for some nurses who used the service infrequently.
Perceived value of monitoring function
Many interviewees highly valued the monitoring function of tele-ICU. When this function worked well, it was intensely appreciated by rural clinicians. Some interviewees reported that tele-ICU reduced the on-call burden for local physicians by using the hub's monitoring service, especially overnight. Some interviewees expressed that tele-ICU provides a physician satisfaction that might enhance recruitment and retention. Similarly, many noted the unique challenges facing nurses in smaller hospitals. Unlike nurses in hospitals with dedicated ICUs, nurses in rural hospitals are often simultaneously responsible for the emergency department, outpatient clinics, and/or inpatient beds, making it impossible to fully dedicate themselves to the few critically ill inpatients. In these situations, the tele-ICU service was especially valued.
Help when retaining patients in special circumstances
Under special circumstances when critical care patients could not be transferred, interviewees stated that support from a tele-ICU hub physician enabled rural hospitals to provide higher-quality care. Most interviewees cited at least one instance in which tele-ICU had provided substantial benefit, usually due to assistance when they retained a patient they would normally transfer if possible. Often, such decisions were related to special circumstances, including inclement weather or strong family/patient preferences to remain local, often for elderly patients or in end-of-life circumstances. In such cases, tele-ICU was seen as an invaluable resource. Many interviewees stated that tele-ICU provided a community benefit for patients and their families by allowing them to remain local.
Lack of consensus about patient needs
Interviewees at CAHs tended to attribute any underutilization to the lack of critical care patients for whom the service was an appropriate alternative to patient transfer. Interviewees at CAHs often stated that their hospital lacked the laboratory and nursing support capabilities to care for a patient whose level of need was high enough to justify ICU-level care. Staff at these hospitals were hesitant to retain such high-acuity patients, reflecting their awareness that patients could “crash” and need the intense intervention from a better-equipped and staffed institution. This viewpoint explains why the assistance provided by the tele-ICU hub “intensivist” (a physician board certified in critical care medicine) was generally less valued than the service's monitoring support. Interviewees noted occasional divergence between the remote hospital's view of a patient's needs and the tele-ICU hub physician's view of the same patient. Interviewees at rural hospitals sometimes felt that the hub physicians might not understand the needs of their patients who were placed on tele-ICU because most were not truly “ICU-level” patients. Some rural clinicians expressed concern that this might cause the hub to provide an unnecessarily high level of service, taxing the rural hospital's limited resources. For example, nurses and other support staff in rural hospitals sometimes resented the number of lab tests ordered for tele-ICU patients by the hub physicians.
Discussion
The perception survey and interviews included questions about multiple facets of tele-ICU services. The hospital personnel who interacted with tele-ICU were generally favorable about it. Most survey respondents indicated that tele-ICU facilitated care for seriously ill patients at their hospital. Respondents in both large and small hospitals viewed the service positively, as did both administrators and clinical personnel. There were significant differences between nurses and providers, but only for 3 of 21 items. The most interesting difference was that 100% of the providers responded that tele-ICU makes caring for patients in the ICU less burdensome, whereas a quarter of the nurses disagreed. Our interviews shed light on this. Some local nurses felt burdened by orders placed by hub physicians that were greater in number and more complicated than orders regularly placed by the local providers, thus increasing the nurses' workload. A small number of nurses who used the service infrequently also complained that hooking up the tele-ICU equipment increased their burden.
When interpreting these findings, several limitations of the current study must be considered. First, we do not know how many staff received notice of the survey and therefore cannot compute a response rate. Second, all respondents worked in hospitals that were clients of a single tele-ICU service, which could limit generalizability. However, these limitations are balanced by several important strengths. In particular, although only one model of tele-ICU was implemented, it is the most widely used commercial model, thus increasing its relevance. 2 More important is that large numbers of survey responses were available for analysis (n=145) from a variety of staff categories at 28 hospitals, permitting statistical analysis to examine differences in perceptions across respondent groups. Supporting this was the insight garnered from interviews conducted with personnel at half of these hospitals.
By examining multiple aspects in the 24 survey questions and by surveying a large number of respondents, this study expands considerably on previously published research. We updated the previously discussed systematic literature review 7 and located eight published journal articles focused on staff acceptance of typical tele-ICU implementations. Two reported perceptions in anticipation of tele-ICU, 9,10 and two reported on perceptions of hub facility personnel only 11,12 ; the remaining four reported on staff perceptions in hospitals receiving the service. 13 –16 One analyzed interview data, 15 and the other three provided limited information on brief surveys that were collected from a small number of staff. 13,14,16 Generally, these studies reported user satisfaction with the technology, effect on receiving care locally, quality of care, and overall tele-ICU use. 13,14,16 Our approach expands on these facets to include survey items to assess each domain in a telemedicine framework, 8 including clinical outcomes, technical acceptability, health system interface, costs and benefits, access, and patient/provider acceptability. Our survey results indicate that both administrators and clinicians view the tele-ICU implemented at large and small hospitals positively across all these domains.
Across all domains, the greatest differences in survey responses were related to utilization of the service. Clinicians who said they used tele-ICU frequently viewed it more positively on multiple survey items than did clinicians who said they used it sometime or rarely. Similarly, personnel at hospitals that averaged more tele-ICU patient days responded more positively, as did personnel at hospitals that had used tele-ICU longer. Because these latter analyses involve hospital-level use rather than individual clinician use, they help clarify that hospitals with more and longer use of tele-ICU have personnel who view its effect more favorably. We speculate that initial resistance to this new technology might decrease over time with greater familiarity. As with other information technology such as electronic health records and computerized provider order entry, initial concerns eventually turn more positive as familiarity is gained. 17,18
Another important theme that arose in the interviews with clinicians at small CAHs was related to the perception that ICU patients at CAHs are different from ICU patients at larger hospitals. CAHs rarely admit critically ill inpatients, usually transferring critical care patients to urban ICUs. Having ICU-level patients stressed staff, especially when tele-ICU hub specialists recommended more intensive diagnostic and therapeutic procedures. However, even in CAHs that rarely care for ICU-level inpatients, the tele-ICU service was valued on those occasions when caring for a critically ill patient was necessary. In the rare situation when a seriously ill patient could not be transferred, the tele-ICU service was reported to be especially helpful for maintaining high-quality patient care.
It is important to note that in small CAHs, ICU beds are more often used for end-of-life care patients or for elderly critical care patients who refuse to transfer. In these cases, rural hospital staff did not desire tele-ICU to provide typical ICU-level services. Instead, rural hospital staff more often requested that the tele-ICU hub provide teleconsultation for specific questions or even telehospice-type services such as reassuring family during end-of-life decision making. This points to the need for the hub facility to recognize local practice patterns and balance the clinical needs of the patient with remote hospital staff workload demands. Perhaps asynchronous but rapid response strategies could be used to involve other clinical personnel in the hub for particular questions, and triage protocols could be established to be responsive to different types of patients.
Tele-ICU is often implemented to provide around-the-clock monitoring of critically ill patients in PPS hospitals that have true ICUs. The service we studied provided tele-ICU to both large and small hospitals. In rural hospitals, tele-ICU is a means of assuring high-quality care locally (in many instances because patients cannot be transferred, at least not immediately) by extending patient care services to locations unable to provide those services with resources available onsite. The value of tele-ICU services was recognized by the vast majority of survey respondents. However, the interview findings suggest that the tele-ICU model familiar to large institutions with independently staffed ICUs, serving steady volumes of high-acuity patients, does not meet all needs especially across varying hospital sizes, particularly in rural and remote communities, where telemedicine fills many service gaps. For the smallest CAHs, typical tele-ICU hub intensivist services are rarely needed but are highly valued when that need occurs.
Moving forward, tele-ICU is likely to evolve to maximize its usefulness in rural areas, for example, by improving monitoring/notification capabilities that provide call relief for rural physicians and that allow rural nurses to effectively staff multiple areas of the hospital. Therefore, as regional healthcare systems develop and restructure, various forms of telemedicine are likely to be incorporated into patient care and business models. Regional systems may well want to keep as much care as possible in close proximity to patients, both to increase patient loyalty to the system and to spread the capacity of the system. Similarly, public policies and financing models promoting appropriate local access to services across the continuum will further support adoption and use of telemedicine to enhance inpatient care. Such policies will be focused on the value of the totality of services, creating more flexibility for delivery organizations to determine how best to deliver that value.
Footnotes
Disclosure Statement
S.K. is an employee of Avera Health. M.M.W., F.U., A.J.P., A.C.M., and K.J.M. declare no competing financial interests exist.