
Abstract

Background and Introduction
The goal for Veterans Health Affairs (VHA) in the U.S. Department of Veterans Affairs (VA) is to support elements of care for 1 million veteran patients, 20% of its enrolled population, with telehealth services in fiscal year (FY) 2015. This is a 2,000-fold increase over 20 years. 1 Telehealth 2 involves the use of information and telecommunication technologies to deliver consultation and care. VHA's telehealth services currently encompass 44 clinical specialties 1 and use technology to re-engineer care delivery processes reduce or eliminate the need for travel, thereby providing the “right care in the right place at the right time.” Telehealth in VHA fits within a broader healthcare vision, one linked with complementary initiatives such as the medical home 3 and patient-centered care. 4 Collectively, these endeavors make veterans' homes and local communities into the preferred site of care, when clinically appropriate, and it is their preference. VHA's telehealth services span the continuum of care from the home (home telehealth [HT]) to intensive care units (tele-ICU). Veteran patients are highly satisfied with these services (mean satisfaction scores between 89% and 95% in FY2013). 1
Transforming the location of care for veteran patients, and growing by 22% annually, 1 VHA telehealth services are critical to VHA's health delivery mission, having come a long way since 1959, when first used 5 to provide mental health services (telemental health) between the University of Nebraska and the Omaha VA Medical Center (VAMC). From then, until 1995, prohibitively high equipment costs, rudimentary telecommunications infrastructures, absence of associated clinical decision-making tools (e.g., the electronic health record [EHR]), and a focus on hospital-based care limited telehealth's role in VHA to demonstration projects, usually linked with academic medical centers or national laboratories. Then, as now, research and training affiliations with 103 academic medical centers offer VHA an ongoing conduit for introducing new innovations, including telehealth.
After 1994, VHA's progressive uptake and dissemination of telehealth took place in three distinct temporal phases, with each phase reflective of the health needs of veterans served, its prevailing state of the art, supporting telecommunication technology platforms, associated clinical decision-making tools, and organizational structures: • Phase 1 (1994–2003) was characterized by local innovation, not coordinated at the national level. Telehealth pilots took place in many clinical areas, spurred by clinicians collaborating with their information technology (IT) counterparts in local VAMCs. Ad hoc telehealth pilots were established in 30 VAMCs. • Phase 2 (2004–2010) was driven by a “systems approach” that supported early adopters of telehealth by creating national clinical, technology, and business underpinnings for three distinct national telehealth platforms: HT, clinical video telehealth (CVT), and store-and-forward telehealth (SFT), platforms that were implemented across 150 VAMCs and over 400 community-based outpatient clinics (CBOCs). • Phase 3 (2011–2014) was determined by VHA's strategic investment in resources to further expand and consolidate telehealth programs, creating an infrastructure capable of supporting an early majority of clinical users to provide mission-critical services throughout 152 VAMCs and over 600 CBOCs and directly into patients' homes.
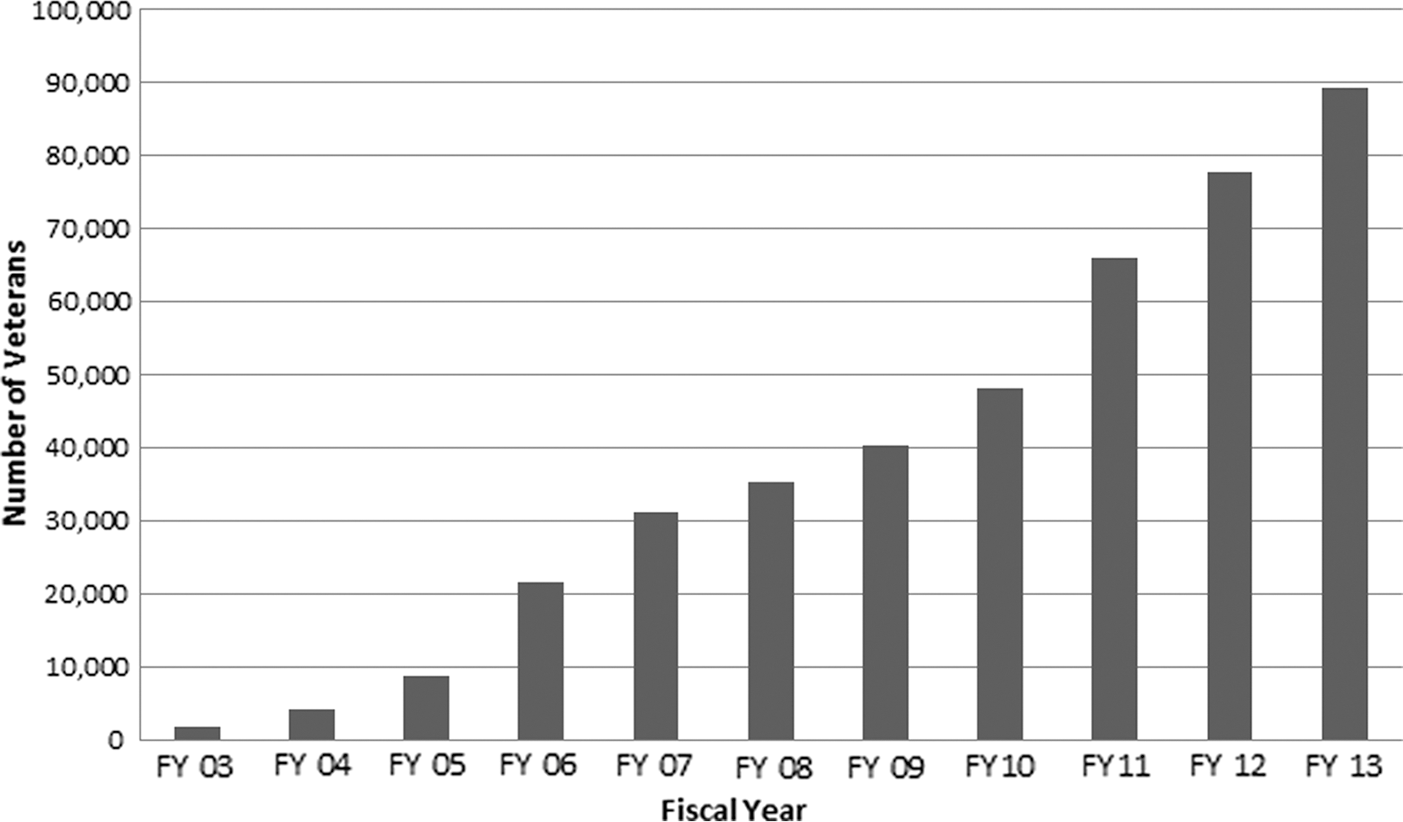
VHA's challenges in creating large telehealth networks mirror the experience of other organizations (nationally and internationally) in implementing and sustaining their programs with associated challenges, which include clinical buy-in, 6 credentialing and privileging, 7 staff training, 8 technology standardization and interoperability, 9 securing revenue streams, 10 clinical risk management, 11 relationships with IT/biomedical engineering, 12 and ensuring the quality of care. 13 Figure 1 shows the rise in numbers of veterans treated via telehealth in VHA between fiscal year (FY) 2003 and 2013. Growth of this size and scope necessitated VHA systematically addressing the above issues, as will be described.

Veterans Health Affairs total veterans served by telehealth, fiscal years (FY) 2002–2013.
This article examines telehealth development in VHA over three time phases during the period 1994–2014. It focuses on the clinical, technology, and business/management processes developed, and organizational support structures created, in order to implement, grow, and sustain these services as their size and complexity increased.
Materials and Methods
This retrospective analysis of telehealth development in VHA is based on discussions with key stakeholders, VHA telehealth documentation (from the VHA Telemedicine Strategic Healthcare Group [SHG], VHA Office of Care Coordination, and VHA Telehealth Services), review of VHA telehealth satellite broadcasts that took place between FY2000 and FY2014, and the author's personal recollections.
Details of the chronology of telehealth development in VHA, and related analyses of the three phases of telehealth development in VHA (FY1994–FY2003, FY2004–FY2010, and FY2011–FY2014), are provided under the following subsections: (1) social system; (2) innovation; (3) communication channels; and (4) time.
These subsections are adapted from definitions in Diffusion of Innovations by Everett Rodgers
14
: • Social system relates to internal/external factors impacting on the VHA mission to deliver healthcare services to veterans eligible for this care and the associated organizational issues affecting uptake of telehealth in an integrated healthcare system providing care to 6.3 million patients annually. • Innovation covers more than technology hardware, software, and telecommunications connectivity associated with telehealth. It includes the clinical, business, and “people” factors necessary for a telehealth program's viability. • Communication channels are mechanisms that encourage telehealth diffusion and institutionalize organizational support structures supporting its widespread uptake. • Time refers to the progression of telehealth critical success factors across each developmental phase and how they have resulted in differential growth levels for the various programs.
Phase 1 Implementation of Telehealth in VHA, 1994–2003
Social System
VHA's initial phase of telehealth implementation coincided with the organization's transformation 15 from a widely disparaged healthcare system 16 to one lauded as providing the “best care anywhere.” 17 This transformation took a centralized hospital-focused organization and changed it into one that was decentralized and primary care oriented. It was accompanied by adoption of new clinical innovations (e.g., EHR 18 and telehealth 13 ) that were driven by meeting the needs of a veteran population older, 19 sicker, 20 and poorer 21 than the general U.S. population. Initial VHA telehealth pilots were grant-funded local innovations, often research studies, conceived and designed to meet locally identified needs in VAMCs and Veterans Integrated Service Networks (VISNs). Limited national seed funding established demonstration projects for spinal cord injury, specialty care services, and collaborations with other federal government partners 22 –24 were important catalysts for ongoing telehealth development.
Innovation
In this first phase of development, VHA's use of health information and telecommunication systems to provide healthcare at a distance was known as telemedicine (reflecting its predominant use by physicians). The technologies typically used were usually commercial off-the-shelf videoconferencing systems, ones that had been developed for administrative, not clinical purposes. VHA piloted a range of telehealth services, including telemental health, 25 digital radiology, 26 teledermatology, 27 telepathology, 28,29 and HT. 30 VHA's EHR (VistA), and its associated digital imaging platform (VistA Imaging), gave VHA a robust IT infrastructure to complement its fledgling telehealth expansion. Close collaboration between clinicians and the VHA IT community 31 created a vision of telemedicine as a “multimedia health record.” 32 Organizational sharing of the EHR across 152 hospitals, and growing numbers of CBOCs, required telecommunication connectivity, and so wide area networks were created in each of VHA's 21 VHA administrative units, VISNs. Collectively, these 21 VISN wide area networks created a fragmented national telecommunications network that supported ad hoc telemedicine consultations between VAMCs and CBOCs, usually via integrated services digital network (ISDN) circuits. Inter-VISN and national consultations were scheduled with an operator and needed a video-bridge. VHA clinicians were permitted to provide telehealth services to veterans in VA facilities in any state, providing they held a full-unrestricted license in any one of the 50 U.S. states 33 (a distinctive difference between VHA and the private healthcare sector). However, the logistics of credentialing and privileging for telehealth were labor intensive in VHA, as in private sector programs. In this early phase of development, VHA's IT community was the prime mover of telehealth. Early pilots typically lasted as long as the funding and/or clinical/IT champions remained involved.
Communication Channels
In 1997 VHA established a telemedicine strategic healthcare group (SHG) with two staff members within VHA's Office of Patient Care Services in Washington, DC. The Telemedicine SHG's role was to support the development, continuity, and sustainability of telehealth programs in order to substantially increase access to care. To do this, the tools at its disposal were formulating strategic plans, developing policies and practices that promoted telehealth growth, facilitating VHA telehealth communities of interest, networking with other stakeholders (e.g., IT and biomedical engineering), and offering ad hoc consultancy support to programs. Five of VHA's 21 VISNs and several of the VAMCs used telemedicine coordinators. Clinical staff involved in telehealth did so as collateral duties, and their initial policy requirement was to formalize credentialing and privileging arrangements. Clinicians had no prior experience of telehealth from previous clinical training programs, and VHA had no formal structures to provide this training; therefore the Telemedicine SHG collaborated with VHA's Employee Education System (EES): reviewing models of telehealth training in other organizations and implementing ad hoc telehealth training resources (derived from telehealth toolkits) from 2002 onward. In FY2000, VHA published its first telehealth newsletter, which has been published quarterly thereafter.
Time
Clinical care, 1994–2003
By FY2003, VHA had experience in using telehealth to deliver care in 30 different clinical areas, with the major ones being mental health, rehabilitation, screening for diabetic eye disease, and management of chronic diseases (e.g., diabetes, heart failure, pulmonary disease, and cardiac failure). To systematize and sustain development in these areas of high clinical need, VHA created telehealth toolkits, beginning with telemental health. These toolkits systematized the clinical, technology, and business processes necessary to successfully develop telehealth services. In FY2003, VHA extended its portfolio of telehealth toolkits to include HT, telerehabilitation, and telesurgery.
VHA's telehealth community
In September 1999 VHA held its first telehealth meeting in Park City, UT. The task for the eight participants was to decide how best to build communities of interest to support telemedicine/telehealth in VHA. They decided to hold VHA telehealth meetings alongside VHA's annual Information Technology Conference and the annual American Telemedicine Association meeting. These meetings both took place in FY2000, and a nascent VHA telehealth community of 70 people (clinical, technology, and managerial) was able to network. To target the growth of clinical communities that could support growth of telemental health, teledermatology, and telerehabilitation, VHA developed lead positions to champion each specialty area, to develop telehealth toolkits, and to build nationwide clinical communities of interest. The Telemedicine SHG's partnership with EES was a critical component in developing these communities of interest and supported telehealth in VHA with regular satellite broadcasts from FY2000 onward, as a means of generating interest in telehealth and sharing best practice throughout all 152 VAMCs.
Evolution of VHA IT architecture for telehealth
Before FY2003 there was no systematic IT support for telehealth in VHA. There were 152 VAMCs, of which fewer than 30 were actively engaged in telehealth and with no unified IT infrastructure or associated support for telehealth. Often telehealth projects were developed using bespoke interfaces at an individual medical center, ones that were not replicable across the system. Both VHA IT and biomedical engineering supported telehealth but without consistent standards for equipment purchase, installation, service, warranty, and help-desk arrangements.
Evolution of business processes and funding for telehealth
Between FY1994 and FY2002 there was no means to systematically code telemedicine activity in VHA. From 2002 a coding system for CVT was introduced. Understanding what telemedicine activity occurred, and where and when this happened, required ad hoc surveys. There was no workload credit for clinicians undertaking telehealth and therefore no direct financial incentive for VHA sites to undertake routine telehealth-based care, and there were no datasets to systematically collect outcomes data.
Creation of the evidence base to support telehealth
Between 1994 and 2004 VHA staff published over 79 peer-reviewed journal articles, contributing to the evidence base for telehealth. The positive findings of a Kaiser Permanente HT study 34 corroborated VHA's strategy of piloting HT and develop an associated care coordination model. 35 A 2001 study of teleretinal imaging to screen for diabetic eye disease 36 supported existing VHA initiatives and encouraged developing further programs.
Phase 2 Implementation of Telehealth in VHA, 2004–2010
Social System
In addition to the Phase 1 drivers, VHA's telehealth development was now driven by four external strategic imperatives, supporting (1) returning veterans and active-duty military from Operations Iraqi Freedom/Enduring Freedom, (2) VHA's mandate from the 1999 Millennium Bill 37 requiring VHA to provide noninstitutional care for aging veterans wanting to live independently in their own place of residence, (3) mandated rural health initiatives 38 to promote access to care, and, finally, (4) the effect of the 2008 global economic downturn on increase the demand for veterans to access VA healthcare.
Innovation
Three major innovations characterized this phase: (1) national implementation of care coordination/HT (CCHT), an HT program providing noninstitutional care; (2) a VHA national model using teleretinal imaging to screen for diabetic retinopathy; and (3) a clinical videoconferencing network to connect 25 major sites in VHA to manage severe traumatic injuries with polytrauma. 39 VHA's platform for CCHT was based on the purchase of commercial off-the-shelf HT technologies that used HT technologies to support patient self-management and coordinate care using data acquired from the homes of veterans with complex chronic conditions that VHA care coordinators monitored. Preventing avoidable blindness for the 20% of enrolled veterans with diabetes provided the rationale for teleretinal imaging in VHA. VHA's Polytrauma Telehealth Network (PTN) created a core clinical videoconferencing capability on VHA's telecommunications backbone linking 25 major polytrauma sites at major nodes on the VHA backbone. 40 PTN provided VHA with the capacity to leverage specialist expertise in polytrauma across the system. The unifying principle underlying use of telehealth across the various HT, SFT, and PTN programs was care coordination; telehealth provided the capacity to connect services across the continuum of care. With the creation of national telehealth programs, VHA developed associated quality management programs for internal accreditation and outcomes assessment.
Communication Channels
With implementation of VHA's national HT program in 2003/2004, VHA designated leads for HT in each of its 21 VISNs. This “braintrust” of VISN leads was an implementation group that connected CCHT with VISN strategic plans for service development. To reflect a wider vision of telehealth to coordinate services across the continuum of care, the Telemedicine SHG was renamed, and repurposed, to become the Office of Care Coordination Services (OCC). Its expanded role was developing, disseminating, and sustaining models of telehealth that incorporated disease management and health informatics to support care and case management. OCC partnered with other clinical services in VHA Patient Care Services that provided peer review and national endorsement for their respective telehealth toolkits. OCC expanded its collaboration with EES and developed HT, SFT, and CVT training centers that used the standardized VHA telehealth toolkits to create virtual training tools. EES provided national communication channels to distribute this content with a focus on using Web services, satellite broadcasts, and streaming video. This training strategy was to train 90% of staff virtually, thereby reducing the need for face-to-face training and conferences. OCC linked biannually with the Joint Commission to discuss its current telehealth operations and future telehealth expansion plans, focusing on quality management.
Time
Clinical care, 2004–2010
By FY2010, VHA had experience in using IT and telecommunication technologies to deliver care in 44 different clinical areas. Telemedicine gave way to telehealth to describe these services, reflecting the multidisciplinary role it was playing. VHA HT programs used disease management protocols to coordinate the care and implemented these clinically for chronic heart disease, diabetes, hypertension, chronic obstructive pulmonary disease, and spinal cord injury (Fig. 2). VHA supported a major rollout of teleretinal imaging from FY2005 (Fig. 3).
Veterans Health Affairs home telehealth end of year patient census, fiscal years (FY) 2003–2013.

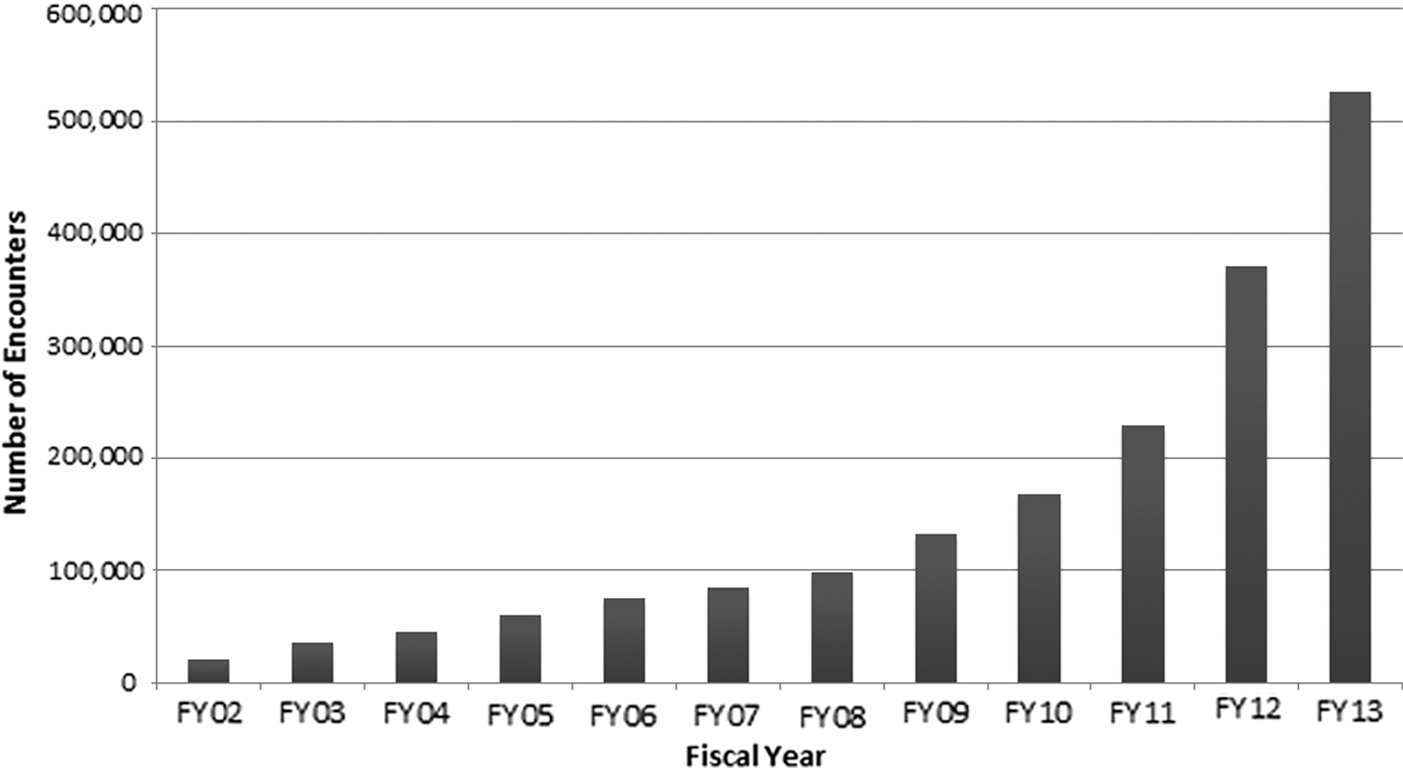
Veterans Health Affairs store-and-forward telehealth encounters, fiscal years (FY) 2006–2013.
VHA's telehealth community
OCC supported VISN leads for HT and developed leads for SFT and CVT also. As part of VHA's expansion of teleretinal imaging, VHA created a national cadre of teleretinal imagers whose role was to acquire teleretinal images in primary care.
Evolution of VHA IT architecture for telehealth
Between FY2004 and 2010, VHA developed a national contract for HT technologies that enabled a standardized platform and data systems. VHA standardized requirements for teleretinal cameras and clinical videoconferencing systems for CVT. VHA's development of the PTN led to the establishment of quality of service standards for wider implementation of VHA's clinical enterprise videoconferencing network that fulfilled a vision of linking all clinical sites with each other to create national consultation networks.
Evolution of business processes and funding for telehealth
VHA introduced systematic coding systems for HT and SFT that mirrored that previously introduced for CVT. Review of these data provided the basis for recognition of workload credit for all three areas of telehealth. Analysis of the costs and cost avoidance of using HT for noninstitutional care and chronic disease management led to recognition of these areas for differential funding allocation under VHA's capitated funding system, the Veterans Equitable Resource Allocation system. 41
Creation of the evidence base to support telehealth
VHA continued to add to the evidence base for telehealth across a wide scope of telehealth. Studies of SFT, 42 HT, 43 and CVT (telemental health 44,45 ) supported their ongoing implementation.
Phase 3 Implementation of Telehealth in VHA, 2011–2014
Social System
This phase of VHA's telehealth development coincided with VHA Transformation Initiatives. These initiatives were designed to make VHA into a 21st century organization in being forward looking, results oriented, and veteran focused. Telehealth was identified, together with initiatives for mental health, specialty care, patient-centered care, homelessness, health promotion/disease prevention, primary care, and women's health, as a new model of care to underpin this transformation. With troop withdrawal from Iraq and Afghanistan and the need to provide services for returning veterans, telehealth played an important part in promoting access. For tech-savvy younger veterans, used to accessing services on electronic devices, telehealth is a natural way to access care.
Innovation
In this third phase of telehealth growth, major innovations included expanding the scope and size of VHA telehealth programs and an emphasis on teledermatology, tele-audiology, tele-amputation, tele-ICU, and the use of mobile devices to support chronic disease conditions. Having expanded HT and SFT through national initiatives in Phase 2, the main thrust of innovation in this phase was the national expansion of CVT to provider specialty care services into primary care (Fig. 4). In FY2010/2011, as part of this national expansion VHA developed a National Telemental Health Center in West Haven, CT, that implemented innovative services for telepain management, telebipolar care, teleschizophrenia, and telecompensation and pension exams. In FY2012, VHA piloted CVT into the home, a program that enabled 2,248 veterans to receive secure encrypted video consultations in their homes on their own personal computers, laptops, and tablet computers in FY2013.
Veterans Health Affairs growth in clinical video telehealth encounters, fiscal years (FY) 2002–2013.
Communication Channels
To expand access to care through CVT, VHA established VISN telehealth leads in all 21 VISNs, Facility Telehealth Coordinators in all 152 VAMCs, and Telehealth Clinical Technicians to support clinicians using telehealth in all facilities and over 600 CBOCs. VHA established a National Telehealth Help Desk to help implement telehealth technologies for CVT and SFT and rapidly troubleshoot any problems. To coordinate these various activities, to determine the strategic direction for telehealth, to develop appropriate policies, and to create training materials, OCC was renamed VHA Telehealth Services. Also renamed were the VHA telehealth toolkits, becoming operations manuals.
Time
Clinical care, 2011–2014
VHA's predominant focus in this phase of development was to grow the three basic models of telehealth (HT, SFT, and CVT) and to expand them in size and scope. To promote clinician buy-in, a monthly clinical champion meeting was established to share and promote telehealth innovation. In FY2011 VHA established pilot programs for tele-ICU to provide remote intensivist support to VAMCs with challenges in recruiting and retaining these clinicians and developed a clinical lead for tele-ICU. VHA consolidated its “conditions of participation,” an internal accreditation processes for HT, CVT, and SFT, into a combined assessment as part of a comprehensive quality management approach to telehealth 46 and incorporated tele-ICU and teledermatology into this process. Of the veteran patients whose care was supported by telehealth in VHA, 47% lived in rural areas in FY2013.
VHA's telehealth community
Having developed strong and cohesive communities for HT, CVT, and HT and master preceptors to support training and development in these three areas, VHA Telehealth Services combined its HT, SFT, and CVT training centers into a single telehealth training center. This change was in recognition of how these areas were converging clinically and technologically. The emergence of other areas of virtual care (e.g., Connected Health) placed telehealth within a wider framework of a continuum of virtual care services, with VHA's patient portal MyHealtheVet as the likely future contender for a consolidated point of access for patient facing services related to telehealth. VHA Telehealth Services moved its traditional communities to embrace a wider vision of virtual care.
Evolution of VHA IT architecture for telehealth
From FY2011, revised contracting arrangements for HT, SFT, and CVT technologies met upgraded requirements. In order to formalize IT support services within VA for these three platforms, VHA Telehealth Services collaborated with IT and biomedical engineering to create a memorandum of understanding and service-level agreements for telehealth to assure current service delivery, to negotiate future growth, and to ensure backup, redundancy, help-desk support, and future upgrades.
Evolution of business processes and funding for telehealth
With workload recognition for HT, SFT, and CVT, VHA Telehealth Services developed formal systems to inform VISN telehealth programs about the resource allocations they accrue from growing telehealth.
Creation of the evidence base to support telehealth
Telehealth is an important area of health services research in VHA, with regular research studies published across the continuum of VHA Telehealth Services, from HT to tele-ICU.
Discussion
Diffusion is the “process by which an innovation is communicated through certain channels over a period of time among the members of a social system.” 14 Telehealth in VHA has followed recognized patterns of diffusion with the social system, innovation, communication channels, and time interacting in a complex adaptive environment to bring about its adoption and uptake. In a review of Figures 1 –4, this adoption and update are following an “S”-shaped innovation curve. 47 Over the three phases of its implementation since 1994, telehealth in VA has passed from innovators through early adopters and from 2011–2014 is moving into the phase of being embraced by an early majority of clinicians in VA.
Telehealth has been introduced in VA to meet the demands on the organization to provide access to care and not as a technology implementation, per se. During this evolution, the nature of the innovations has changed from sporadic activity at local VAMCs by individuals to one where a wider consensus implements national models based on systematic pilots. Although this has frustrated some innovators, it has provided the assured models of telehealth-based care that a wider clinical community can embrace because they are nationally endorsed by an organizational peer group of clinical leaders in each specialty area, as safe and effective and compatible with outside quality reviews. The partnership with EES has been particularly important in creating the diffusion channels, building the communities of interest, and engaging the clinical champions who have been vital to growth of telehealth. The temporal dimension to growth of telehealth has not been serendipity over time. Through its metamorphosis from Telemedicine SHG to Telehealth Services, VHA's program office for telehealth has linked with the wider VHA telehealth community to develop sequential strategic plans for telehealth, the successful implementation of which have shaped the evolution of telehealth in VHA.
Conclusions
Telehealth is now a mature innovation in VHA that is transforming healthcare delivery in many areas of clinical care that focus on the management of chronic disease. Its implementation has followed a recognized course with respect to the uptake and diffusion of innovation. Telehealth services are now mission critical to VA in areas that include HT, teleretinal imaging for diabetic retinopathy, teledermatology, tele-ICU, and tele-audiology. VHA has taken a “systems approach” to its telehealth implementation and re-engineered care delivery processes to create the clinical and business rationale for implementation. VHA has strategically adapted its approach to the innovation and communication channels over time. In using telehealth to deliver increasing levels of mission-critical services to veteran patients, VHA must keep addressing the critical diffusion factors mentioned above. Keeping abreast of the ever faster pace of technology change is vital for VA if it is going to provide the usability that patients and staff will demand to sustain telehealth uptake by the early majority and move into the phase of adoption by the late majority, at which time VA will have radically transformed from a bricks and mortar-based healthcare delivery system to one that has embraced virtual care technologies.
Footnotes
Acknowledgments
The author recognizes and applauds the work of VA staff throughout the organization who have been involved in developing, implementing, and sustaining telehealth services in VHA from 1994 to 2014. Their singular devotion to serving veterans and passion for excellence has been critical to VHA's successful adoption of telehealth and over 1.7 million unique veterans receiving access to care in this way.
Disclosure Statement
No competing financial interests exist.