
Abstract
Introduction
Two decades after a report by Tepetes et al. 1 of a successful liver transplant for highly symptomatic hepatic neoplasms that were unresectable, there is still debate over the risks of this procedure and, indeed, over whether it should be performed at all.
Some recent reports have focused on analyses of outcomes after operative management of benign hepatic lesions and have shown that surgery for benign liver lesions is associated with high patient satisfaction and improved the postoperative patient-reported quality of life. 2
Patients with growing and nonresectable liver hemangiomas should be followed up by a transplant center with extensive experience in complex liver disease. They could be treated on an emergency basis with total hepatectomy and orthotopic liver transplantation, with an expectation of good long-term results. 3
Materials and Methods
A 37-year-old woman was referred to our institute in January 2005, following an incidental liver ultrasonography finding of multiple liver lesions of unknown origin. She underwent full laboratory and radiologic work-up in an attempt to establish the etiology. All chronic liver diseases were excluded, and all tumor markers were within normal limits (alpha-fetoprotein, 1.05 IU/mL; carcinoembryonic antigen, 0.76 ng/mL; cancer antigen 19.9, 9 U/L; cancer antigen 125, 8.3 U/mL). Soon after, she underwent upper abdominal magnetic resonance imaging with hepatospecific contrast that showed at least nine lesions, from 1 cm to 4 cm. All lesions were hypointense on the T1-weighted phase and hyperintense on the T2-weighted phase, with mild enhancement in the late acquisitions and intralesional diffusion of the contrast dye 2 h after. Because these characteristics were not specific, it was decided to proceed with an ultrasound-guided biopsy of one of the lesions. A first biopsy was done in February 2005 and showed a small area with ectatic vessels but with no evidence of malignancy.
She was put on radiologic follow-up, with magnetic resonance every 6 months. During follow-up, the lesions began to grow, some significantly. With these signs, and because of the fear of malignant transformation, we decided to do a new biopsy in one of the large lesions, which was done in August 2009. A biopsy-proven diagnosis of multiple benign hemangiomatosis of the liver was made.
Because her clinical condition was good and she was not complaining of any symptoms, she was again put on regular radiologic follow-up, with upper abdominal magnetic resonance undertaken every 6 months. During that period we observed that the liver lesions continued to grow, even if the patient remained asymptomatic.
In December 2013, the patient began complaining of abdominal discomfort, diffuse abdominal pain, and intense asthenia. She was admitted to the emergency department of her local hospital, where she had a complete blood count showing severe anemia, with a hemoglobin level of 6 g/dL and a hematocrit of 20%. Abdominal pain was treated with oral analgesics, and she was transferred to our hospital in order to study the origin of the severe anemia.
A computed tomography scan showed a further increase in size of the hemangiomas (with the largest having grown to 22 cm), hemoperitoneum, and severe dilatation of the biliary tree, which was compressed by the hemangiomas. All hepatic vessels (portal vein, hepatic veins, and hepatic artery) were patent. A diagnosis of intraabdominal bleeding secondary to rupture of the liver hemangiomas was established. She underwent several transfusions of packed red blood cells, with a daily blood requirement of 300 mL, and developed hemodynamic instability after admission to our department.
No attempt was made to localize the bleeding with angiographic or surgical control, either as definitive therapy or as bridge therapy. Considering her young age, the need for multiple blood transfusions, and the absence of other valid therapeutic options, it was decided to put her on the waiting list for urgent liver transplantation. While on the waiting list, her sister was worked-up as a potential living liver donor. Before her sister's living-donor work-up could be completed, a liver from the deceased donor became available at a small local hospital with no experience in organ donation. The donor was a 19-year-old woman affected with Down's syndrome and chronic renal failure on peritoneal dialysis. She died of a spontaneous cerebral hemorrhage, and her parents volunteered to donate her organs.
Telemedicine Technology
The tele-intensive care unit (tele-ICU) connection was made with a system of Internet protocol videoconferencing-on-wheels equipped with local area wireless technology that complied with the standards for the safety and effectiveness of medical electrical equipment published by the International Electro-technical Commission (series IEC 60601). The whole system of videoconferencing (including video codec, videoconferencing microphones, and laptop speakers) was less than 0.55 m2 and was simple to transport into an intensive care unit (ICU). The system was equipped with ethernet connectivity with traditional transport control protocol (TCP) in which a connection-oriented protocol is established to the hospital network and maintained until the application programs at each end have finished exchanging messages with wireless connectivity to be able to allow at least 2.5 h of continuous videoconferencing without the need for a main power connection.
The cart was equipped with a monitor with a liquid crystal display that allowed good definition of displayed images. The codec-supported protocol for sharing content also allowed optimization of the bandwidth used by allowing high-definition videoconferencing.
The cart was equipped with a silent pan–tilt–zoom camera with a 12× optical zoom, designed for clinical use, and was compliant with regulations for use in hospital environments.
The tele-ICU system allowed remote management of all camera functions, including pan, tilt, and zoom so that the user could remotely control the camera, and had high-quality audio. A directional microphone with high sensitivity allowed audio transmission of voices, even when away from the videoconferencing system.
Results
A tele-ICU technology was networked with the bedside ICU team via audiovisual communication and computer systems. It was used to provide clinical data to intensivists, critical care nurses, and regional transplant coordinators, modify the deceased-donor management with medication orders, and enhance donor hemodynamic stabilization (Fig. 1). Despite the marked hemodynamic instability and the difficult realization of a proper fluid balance in the deceased donor with these comorbidities, thanks to a telemedicine system our anesthesiologists were able to stabilize the donor, allowing the procurement to be carried uneventfully. After admission to the ICU, the donor presented hemodynamic risk factors, including prolonged hypotension (systolic blood pressure of <60 mm Hg for more than 2 h), and required dopamine (10 μg/kg/min) for more than 6 h to sustain blood pressure associated with hyperkalemia. Before the systemic infusion of two inotropic drugs to sustain donor blood pressure, the tele-ICU connection with the Mediterranean Institute for Transplantation and Advanced Specialized Therapies was started. As suggested, a continuous renal replacement therapy was initiated, and a progressive electrolyte balance was recorded. Hemodynamic instability was avoided, and the procurement procedures were performed after 48 h, without administration of amines.

Flowchart showing every phase of the tele-intensive care unit (tele-ICU) and the decision-making steps for scheduling the donor surgery. Once the organ is accepted for a potential recipient, transportation arrangements are made for the surgical teams to come to the donor hospital, and surgery is scheduled. It is mandatory to emphasize the role of telemedicine in aiding the single parts of deceased-donor management to merge into the main goal of deceased donor hemodynamic stability. ICU, intensive care unit.
Our recipient was transplanted with a whole liver with less than 8 h of total ischemia time. At laparotomy, hemoperitoneum was present, although the patient was hemodynamically stable. We usually perform liver transplantation in massive hepatomegaly patients without venovenous bypass, 4 as we did in this case. Despite the active bleeding, the patient remained hemodynamically stable throughout the procedure. The native liver was huge (Fig. 2), weighing 9 kg.
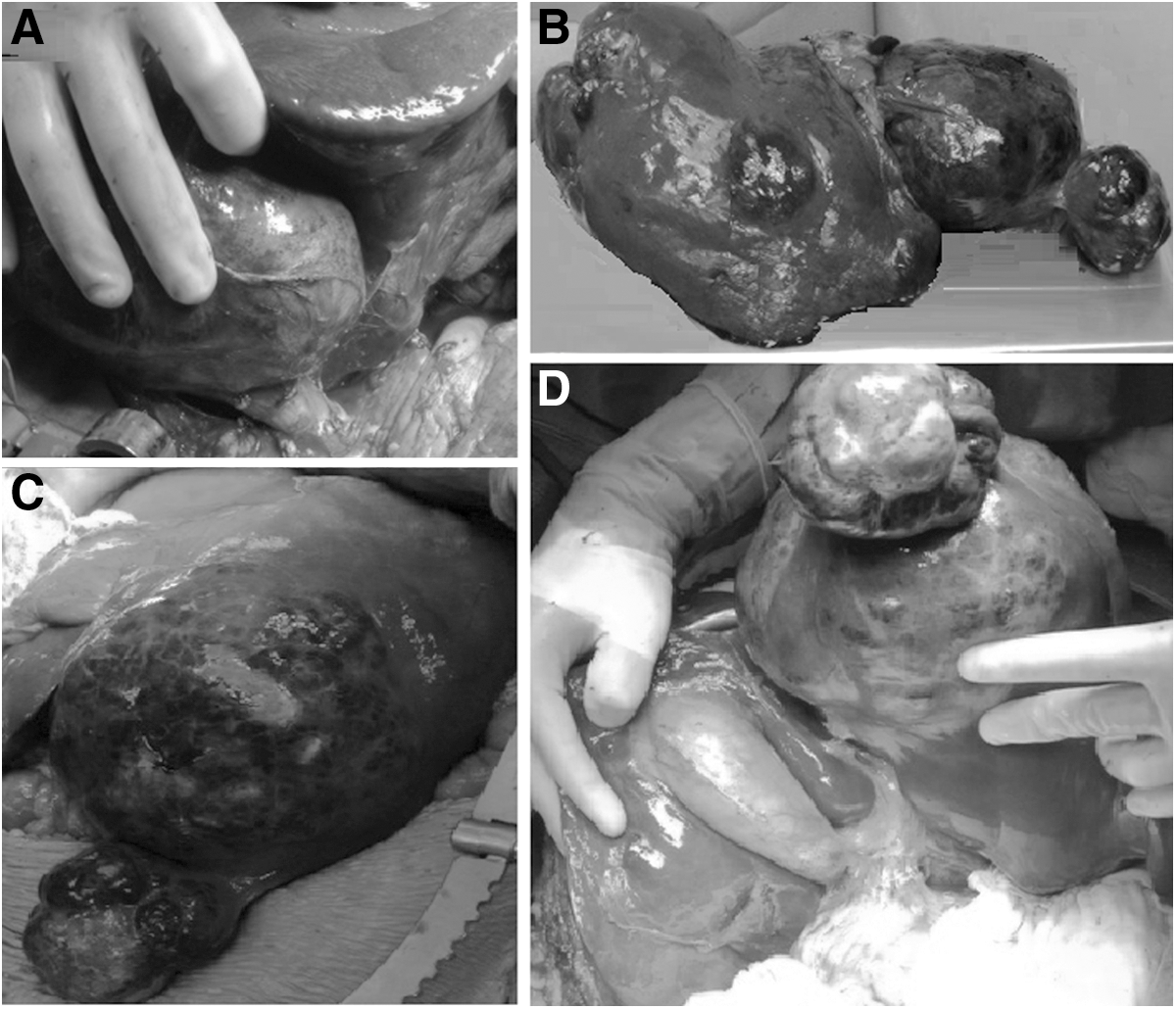
Intraoperative view of multiple giant hemangiomatosis.
The recipient's postoperative course was uneventful. Five months after transplantation she is alive and well, with a normal-functioning whole liver allograft. The tele-ICU system allowed the physicians from the donor hospital and the Mediterranean Institute for Transplantation and Advanced Specialized Therapies to work together and implement all the procedures necessary to guarantee that the organ to be procured and transplanted was not damaged.
Discussion
The tele-ICU technology applied for managing deceased donors has considerable advantages over traditional management, especially in the Mediterranean Basin, where there are limited numbers of board-certified anesthesiologists. It is well known that telemedicine has been used in several healthcare areas for improving outcomes, lowering costs, and heightening patient access to high levels of care. 5,6 Ours is a positive story of the value of tele-ICU technology in rendering critical care to a patient and validated the use of tele-ICU technology when donor organs are identified in a rural hospital that does not have a trauma unit or board-certified anesthesiologists. A remotely based critical care team can be networked with the bedside ICU team via state-of-the-art audiovisual communication and computer systems.
A tele-ICU connection might be established to allow a major teaching institution linked with the procuring organization that typically accesses the computerized organ matching system to enter information about the donor organs and run the match program. It may also become an alternative way to provide effective ICU service for managing deceased donors who lived in rural areas with small local hospitals with no experience in organ donation. When it is requested or when there is a need to guarantee a perfectly matched liver donor/recipients, physicians, nurses and other critical care specialists could receive clinical data electronically, create medication orders, and communicate with on-site caregivers to implement changes in donor care.
Cavernous hemangiomas are congenital vascular malformations that enlarge by ectasia rather than neoplastic growth and are the most common benign hepatic tumor. Recent recommendations indicate that patients with hemangiomas smaller than 4 cm and without any symptoms should be kept under observation only. 7
Although surgical treatment is the classic method for symptomatic giant hemangioma, some studies have evaluated the effects of embolization with bleomycin mixed with lipiodol for ameliorating symptoms and inducing size reduction. 8 Because surgical treatment for giant liver hemangioma has morbidity rates similar to those obtained in patients followed up without treatment, it has been argued that liver resection should be reserved for patients with severe symptoms or disease-associated complications. 9
Transcatheter arterial embolization of the hepatic arteries has been adopted for tumor shrinkage, with or without the association of sorafenib administration. 10 Transcatheter arterial embolization has also been proposed for the sequential management of ruptured, bleeding liver tumors and for nonsurgical treatment of symptomatic giant liver hemangiomas. 9,11
Conversely, very recently, a study by Kneuertz et al. 2 analyzed which factors most impacted quality of life to determine which patients derived the most benefit from surgery for benign liver lesions. They examined the response rate of 179 patients over the course of 10 years, drawn from prospectively maintained databases of two tertiary referral centers (The Johns Hopkins Hospital and the University of Pittsburgh Medical Center). They concluded that liver resection for benign liver tumors was associated with improvements in quality of life domains and that those treated laparoscopically also seemed to enjoy more benefit in terms of pain control. 2
In our department, we consider an early surgical therapy if a subcapsular hemangioma of the liver is present and there is enlargement of the lesion associated with symptom progression during follow-up.
Although multiple benign hemangiomatosis of the liver requiring emergency transplant is rare, and to the best of our knowledge this is only the second report worldwide, 3,7 we believe our case supports the indication for patients with asymptomatic, but growing, hepatic hemangiomas to be followed up in a transplant center with extensive experience in managing complex liver disease. 8,12
The uniqueness of this case is related to the coincidence of the emergency indication for a liver transplantation and the contemporary organ procurement organization because it is highly unusual for the recipient team to be managing a deceased donor.
Conclusions
The telemedicine system and tele-ICU are becoming increasingly important tools for ensuring the best care for patients and deceased donors, wherever they are. With proper application, we might offer possible solutions to the shortage of board-certified anesthesiologists, train more intensivists, and increase the use of telemedicine on a regional level, where the most critically ill patients would be sent to high-level ICUs.
The management of the donors is extremely important in guaranteeing the best transplant outcomes, especially in this very rare case of an emergency liver transplantation for a spontaneous hemoperitoneum secondary to huge multiple benign hemangiomatosis.
We are currently working with the Regional Transplant Center to plan a systematic connection with other Sicilian ICUs. We would like to use tele-ICU not only for organ donation and procurement, but also, and above all, for collaboration in the medical and surgical treatments of the most complex and seriously ill patients.
Tele-ICU technology could be a promising resource for emergency transplantation, reducing the urgent need for living donation and allowing a faster recipient recovery and return to normal life. Our first tele-ICU case offers early confirmation of the feasibility of this procedure.
Footnotes
Acknowledgments
The authors thank Warren Blumberg for his valuable critical editing of the manuscript.
Disclosure Statement
No competing financial interests exist.
S.G. drafted the article critically for important intellectual content. D.P., G.B., A.A., G.P., I.P., D.C., M.S., and G.V. made substantial contributions to conception and design, acquisition of data, and interpretation of data. S.G., D.P., and I.P. wrote the article. S.G. and G.V. gave the final approval of the version to be published.