
Abstract
Introduction
The application of radioactive iodine 131I in patients with differentiated thyroid cancers was approved more than 60 years ago, 1 both for ablation and for the treatment of remnants/recurrences and/or local and distant metastases of differentiated thyroid cancers. It is considered essential in the differentiated thyroid cancer treatment algorithm for the majority of patients. 2,3
Hospitalization in special premises with restricted access (“restricted area” [RA]) is mandatory for patients who receive radioiodine 131I until their body radiation drops below the allowed value, 4,5 as it minimizes environmental hazards. Legal requirements for maximum patient radiation levels upon discharge differ among countries, so the hospitalization can last between 2 and 5 days.
Keeping in mind the overall costs of radioiodine treatment, the limited capacity of the hospital premises for radionuclide therapy, and the slight inconvenience of being confined in the RA, it is of great importance that patients be discharged as soon as possible. The standard procedure for checking the whole-body burden after receiving high doses of radioiodine is to measure the exposure rate by a manual Geiger–Müller counter or a similar device at a distance of approximately 1 m from the patient's body. The procedure has serious shortcomings and limitations: it is subjective and imprecise due to variable geometry of the measurement; it usually involves the overexposure of the staff to significant levels of radiation, especially after repeated measurements, which require them to be in the vicinity of the patient at least several times per day; and, finally, it is time consuming, as it requires the presence of the personnel even during weekends or holidays.
In order to overcome the disadvantages of the usual measuring procedure for patients receiving radioiodine 131I, our team has devised a detection system for online, real-time telemonitoring (THYRPAN-TM), which can provide remote measurement of the radiation exposure rate.
Materials and Methods
Technical Characteristics of the Real-Time Online Telemonitoring Device Thyrpan-Tm
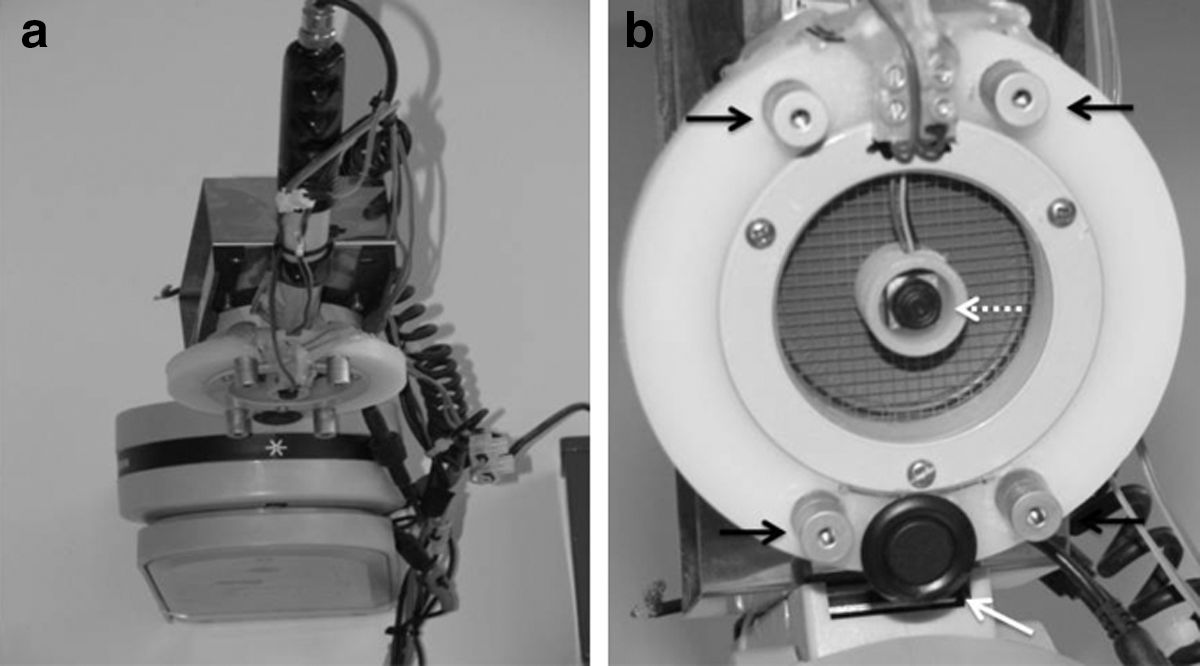
The THYRPAN-TM was constructed using a 2-inch-diameter pancake probe (model T-1190; Technical Associates, Canoga Park, CA) as a substruction, which was placed on a pan-tilt-zoom device used to direct the detector toward the desired region of the patient's body. The positioning of the detector via the pan-tilt-zoom device is controlled by a digital video recorder and the appropriate software. The control can be local, in which case the digital video recorder's software (iVMS-4000; Hikvision, Hangzhou, China) is used, or remote, via the Internet, using any browser, such as Microsoft (Redmond, WA) Internet Explorer, Google (Mountain View, CA) Chrome, Mozilla (Mountain View) Firefox, Opera, etc.
The position of the detector is visually controlled by a microcamera placed in the center of the detector's plane. We used an ultra-small high-definition complementary metal-oxide semiconductor closed-circuit TV microcamera, which provides a real-time video control of the probe's positioning through a live video signal.
Four laser pointers were placed around the detector for the purpose of marking the area of the patient's body to which it is pointed. They can be switched on/off by means of the digital video recorder. In addition, an ultrasound sensor placed on the edge of the detector holder was used to estimate the exact distance between the probe and the patient's body. The detector is connected to a personal computer (PC) by means of the customized hardware/software open source system Theremino® (
The ultrasound sensor and the microcamera attached to the pancake probe are connected by an appropriate electronic device in order to obtain the mixed live video signal and the data about the measured distance between the pancake probe and the patient's body at the same time. For this purpose, we have used control unit PS-LC3-R of car parking system model PM9805 (Parkmatic®, Aurolite Industrial Limited, Hong Kong). The prototype THYRPAN-TM is shown in Figure 1.
The laser pointers and ultrasound sensor are turned on automatically by the software when we want to check the position and the distance of the probe. This command is performed through the free “focus out” control line of the pan-tilt-zoom controller, which enables the lasers and the ultrasound sensor to be turned on at our command.
Using a remote connection by means of any of the following (virtual private network, remote desktop connection, or virtual network computing or by TeamViewer® software [TeamViewer US LLC, Tampa, FL]), a physician can access the data acquisition computer (connected to the Theremino system) and have an online control of the probe position during the measurement, as well as the exposure rate values at any time and from any distance (Fig. 2). The remote connection to the data acquisition computer can be made via another computer from the Department of Nuclear Medicine, by any of the physician's home computers, or via smartphones (Fig. 3).
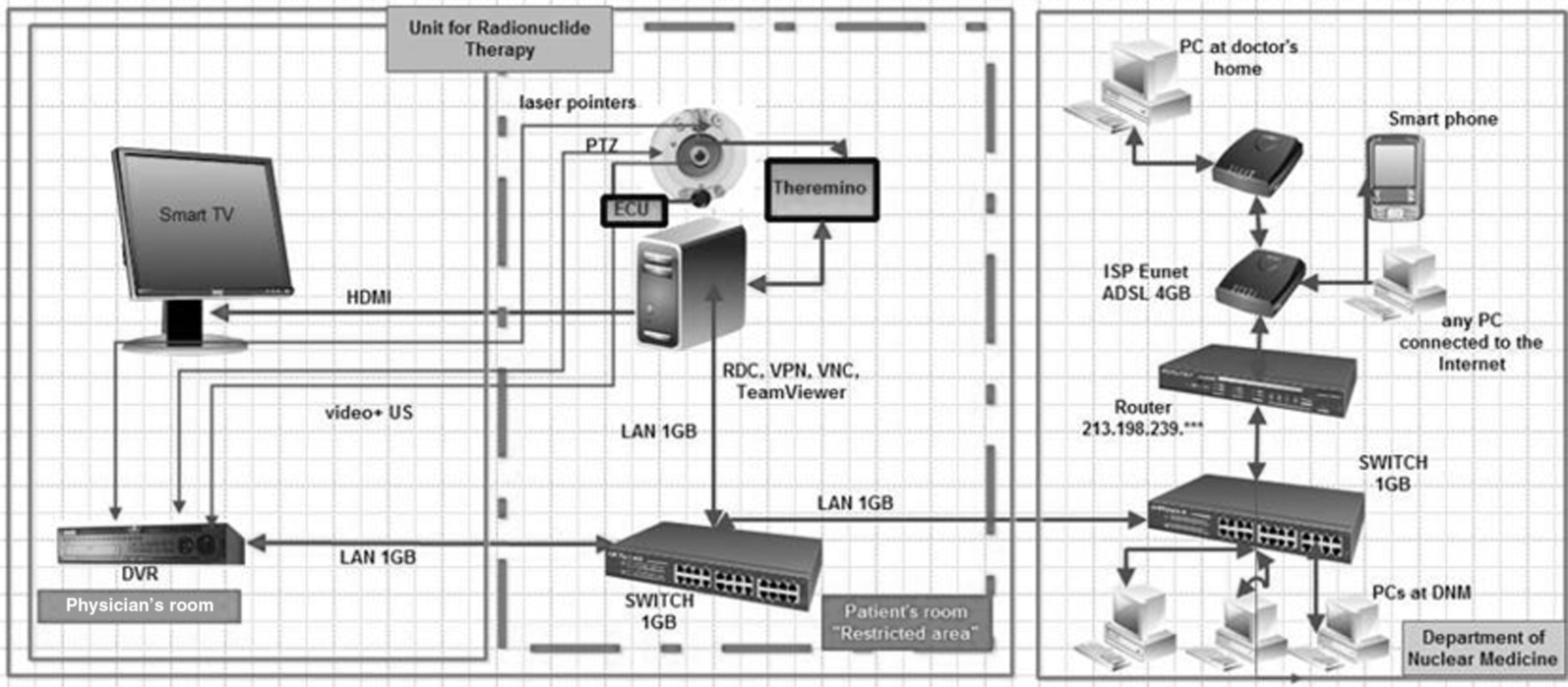
Scheme of our system (thick dashed lines indicate premises with a high radiation exposure rate [i.e., “restricted area”]). DNM, Department of Nuclear Medicine; DVR, digital video recorder; ECU, electronic control unit; HDMI, high-definition multimedia interface; LAN, local area network; PC, personal computer; PTZ, pan-tilt-zoom; RDC, remote desktop computing; US, ultrasound; VNC, virtual network connection; VPN, virtual private network.

Remote connection to the acquisition computer established with a notebook computer and a smartphone at the physician's home.
Testing System Characteristics
The system was tested for stability, efficacy, and linearity by performing at 1-min intervals measurements of the 110 MBq 131I source exposure rate at a distance of 10 cm over 32 days. During that period, the system recorded 46,000 values of exposure rate. The system efficacy, linearity of the exposure rate response, and stability were based on the extent of divergence between theoretical and measured exposure rate values.
Patients And Data Acquisition
Prior to the first measurements on patients, the staff was instructed in a separate educational session on positioning the patients and appropriate use of the system; a brief step-by-step procedure was developed to provide for consistency in the measurements. THYRPAN-TM was then used to measure the exposure rate following the administration of radioiodine in 15 patients (10 females and 5 males) following total thyroidectomy due to papillary thyroid carcinoma. None of them had distant metastases. Nine patients received 5.55G-Bq radioiodine doses, and 6 patients received 3.70-GBq doses. Before application of radioiodine therapy, all patients were briefly educated on how to assume the proper position during the measurement process, in order to preserve the same geometry for each measurement. The patient education was performed always by the same staff member, using a predeveloped checklist.
The system acquired data minute by minute during the patients' entire hospitalization period, collecting about 4,000 datasets, which showed changes in the radiation exposure rate during the individual patient's free activities in the RA (sleeping, rest, movement, using the shower and toilet, etc.).
In addition, the patients were instructed to stay in a particular position for 3 min every hour, during the first 10 h, as well as 20, 23, 26, 29, 32, 44, 47, 50, 53, and 56 h after the radioiodine administration. Using THYRPAN-TM we were able to remotely control patients' positions and correct them if necessary. The data were acquired from the heart region, keeping the same distance during all measurements. Prior to the measurement, the patients were instructed to close their eyes in order to avoid any potential damage from laser beams. The datasets obtained from patients in the prescribed position were considered reference points for exposure rate measurement.
Written informed consent was obtained from patients before the measurements were initiated.
Results
Stability and Efficacy of the Thyrpan-Tm Detector
The radiation values of the 131I source measured by the THYRPAN-TM showed minor deviation from the theoretical values. The greatest deviation (7.20%) was measured during the first 131I half-life, and it was located in the highest exposure rate area (Fig. 4a). Starting from the second half-life of 131I and further out, the recorded deviations have waned. During the whole 32-day testing period the exposure rates did not fluctuate significantly, which demonstrated the stability of the system.
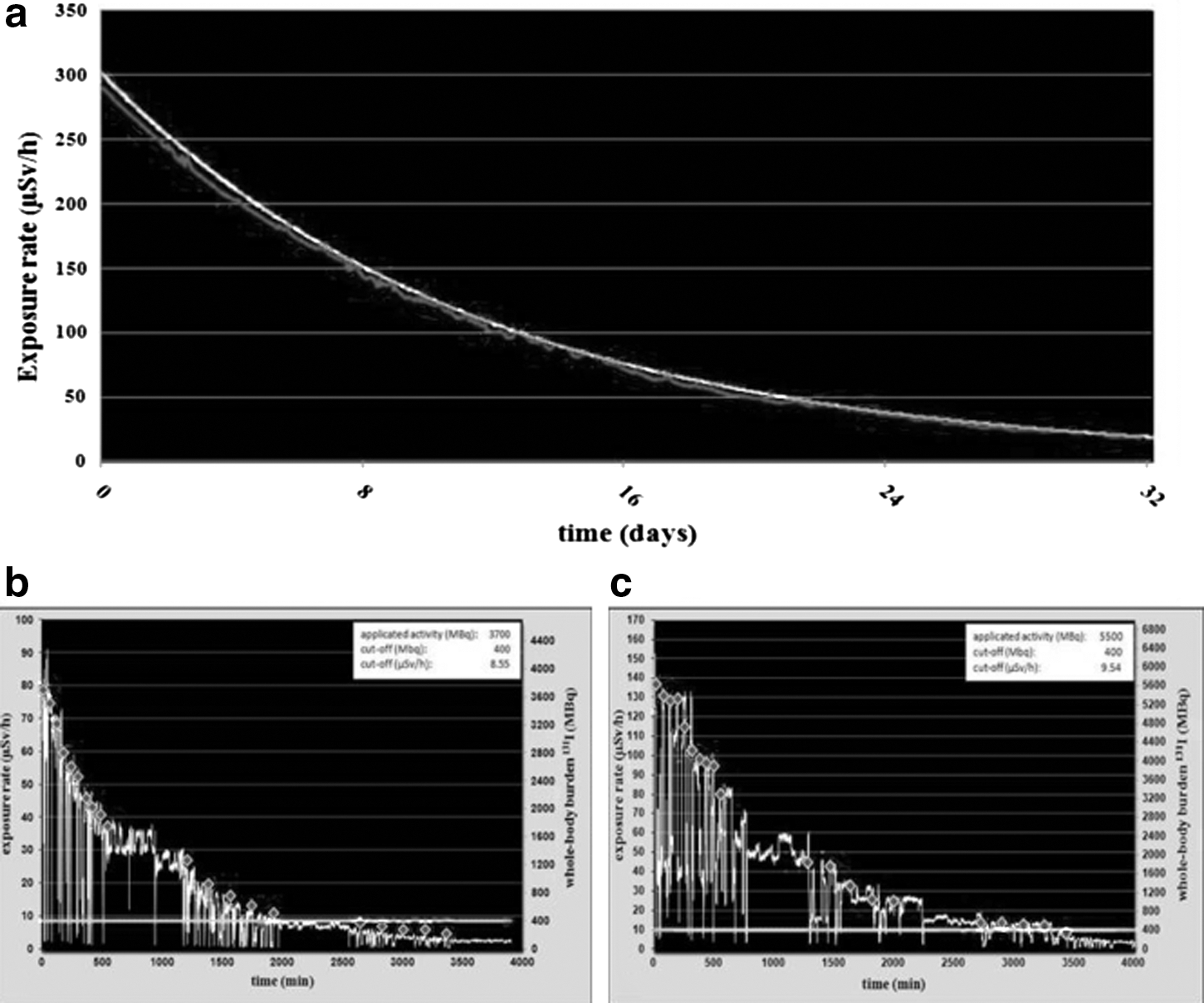
As for the highest expected values, which are equivalent to the exposure rate at a 1-m distance from a patient treated with 5.55 GBq of 131I immediately after the application, the deviation of the measured values from the theoretical ones did not exceed 4.91%, showing a near-linear exposure rate response and demonstrating the efficacy of the detection system.
Clinical Testing of the Thyrpan-Tm System
Elimination rates of radiation from patients' bodies were similar in reference points and during free activities. The amount of time in which residual body radioactivity reaches the point of 400 MBq was significantly shorter after 3.70 GBq (1.88±0.47 days; range, 1.34–2.43 days) than after the 5.55-GBq dose (2.59±0.29 days; range, 2.08–2.95 days) of 131I (p<0.05) ( Fig. 4b and c ).
Discussion
In our previous study we presented a telemedicine system that enables video surveillance of the RA and telemonitoring of the patients' vital functions following the administration of radioiodine. 6 This experience prompted our decision to upgrade the previous system and enable it to measure the exposure rate online, in real time, during the entire hospitalization period.
To our knowledge, only one study has been published so far that deals with radiation monitoring of patients treated with high doses of radioiodine 131I. 7 This study described an old and inefficient type of communication, using modem connection by phone. Technically, it was a pollable Geiger–Müller detector with the continuous data acquisition function, which did not happen in real time and could not be accessed online.
The THYRPAN-TM detector can measure the exposure rate online, in real time, during the entire hospitalization period, using the same geometry of measurement and the technology that can target the same body region. It makes the remote calculation of the whole-body burden of 131I possible at any moment. It has an important role in deciding when to discharge the patients. This is particularly important, due to the fact that the decrease in body activity after the application of the same dose of 131I differs markedly among patients. It depends on many factors, including the size (volume) of the target tissue (thyroid remnant, tumor remnant/recurrence, and/or tumor metastases) and other factors that can affect pharmacokinetics of radioiodine, such as kidney function, concomitant medication, and functions of various organs. 8 In favor of this is the fact that our patients reached permitted levels of radioactivity 2.08–2.95 and 1.34–2.43 days following the application of 5.55 MBq and 3.70 MBq of 131I, respectively, demonstrating that the amount of time in which residual body radioactivity reaches the point of 400 MBq was significantly shorter after receiving lower doses of iodine, but in some cases the interval of reaching the permitted radioactivity can be the same regardless of the activity applied.
Our system ensures permanent insight into the position of the detector in relation to the patient's body with the help of a microcamera placed in the center of the measuring probe's visual field. Additionally, maintaining the same position of the detector by means of laser pointers and keeping the same distance with an ultrasound sensor make the measurement geometry of the detection system constant.
Based on the testing results, our system has a near-linear exposure rate response and minimal lost counts (i.e., good efficacy) over the relevant exposure rate range. During the whole 32-day period, the measured values of the exposure rate did not fluctuate significantly (i.e., the system was stable and satisfied the requirements for the exposure rate measurement of the whole-body radioiodine burden in patients treated with high doses of this radionuclide).
During the clinical testing of our system, the exposure rate was recorded in 1-min intervals in order to get a full understanding of radioactivity elimination from the body and the changes that were recorded during various free activities of the patients. Because our patients were hypothyroid, they spent most of the time in bed, causing the geometry of the measurement to be very similar to that of the reference point geometry. This can explain why the decrease in the exposure rate was similar both during patients' free activities and in the reference points.
The THYRPAN-TM detection system is currently being upgraded, with the focus on predicting the discharge of the patients from the RA on the basis of exposure rate decrease during the first day of hospitalization. Because we believe that this system has the potential to decrease the length of stay of the patients and overall costs of radioiodine therapy, the next step will be to accurately measure these potential benefits. Because we are in possession of a detailed database of patients treated with radioiodine in the past without this system, we will compare their length of stay, resource utilization, and costs with the patients who will be treated by the new system after receiving different doses of radioiodine therapy, such as 1.85, 3.70, 5.55, and 7.40 GBq. New patients will be matched with the historical controls by age, sex, the tumor grade, and dose of radioiodine received. Based on that, we expect to obtain useful data for promotion of further routine clinical use of our system.
Conclusions
The THYRPAN-TM prototype is a safe and user-friendly system for the measurement of the exposure rate following the administration of radioiodine. It enables the telemonitoring of patients, as well as real-time and online measurements of the whole-body burden of 131I, which are essential for deciding when to discharge the patients. The implementation of this system in clinical practice should enable a more rational utilization of hospital resources and a decrease in overall treatment costs. Moreover, the system is useful in protecting the staff from overexposure to radiation.
Footnotes
Acknowledgments
This work has been supported by the Ministry of Education of the Republic of Serbia, under projects 175007 and III41007. The THYRPAN-TM prototype has been realized with support from “Prizma” Company, Kragujevac, Serbia.
Disclosure Statement
M.R. is an employee of Prizma Company. M.M., M.J., S.J., V.U., and M.V. declare no competing financial interests exist.