
Abstract
Introduction
In a chronic disease such as diabetes, responsibility for the daily management of the illness shifts from the healthcare professional to the individual with the disease and their immediate environment. In this shift, the individual with diabetes becomes the main actor, and it is necessary for him or her to develop a diverse skillset to maintain a satisfactory quality of life. 1
Consistent with the aim of empowering people with diabetes, the Big Blue Test (BBT) is a program launched through the Internet and linked with World Diabetes Day. The objective of the BBT is to raise awareness of the importance of physical activity in managing diabetes. In fact, the importance of physical activity to the proper management of diabetes is supported by data cited in several recent studies. 2,3
A participant in the BBT voluntarily signs up for the program and follows four steps: 1. Tests his or her blood sugar 2. Performs a physical activity during a 14-min interval 3. Tests his or her blood sugar again 4. Shares his or her experience by collecting his or her own data and answering some questions through the Web (the questions are described in the Procedure section).
The BBT is run by the Diabetes Hands Foundation, a nonprofit organization that since 2008 has developed different programs aimed at people affected by diabetes.
The theoretical models that have been developed to explain how people can become active agents of their own health have used the intention (the motivation) as the main predictor of health behavior or change behavior. But, very often, intention of making a change in behavior is not the best predictor of real change. Intention needs to be supplemented by other factors that can facilitate its translation into action. 4 More recent models emphasize the importance of self-efficacy as a key variable in explaining how people can take control over their behavior. Perceived self-efficacy refers to a person's confidence in his or her abilities to perform required actions and achieve desired results. Applied to the field of health, perceived self-efficacy is confidence in oneself to change some risk behaviors for improved health and/or encourage healthy behaviors through personal action. 5 –8
It is believed that improving patient self-efficacy is a critical pathway to improved self-management. Because diabetes self-management incorporates behavioral, personal, and environmental factors into daily performance of recommended activities, the concept of self-efficacy is also relevant for improving self-management. 9 In fact, self-efficacy has been shown to be important for appropriate self-management for many chronic health conditions. 10,11
Along with self-efficacy, social support is also a very important psychological variable in promoting behavior change, as the latter is not merely the product of personal ability, but also arises from interaction between the individual and his or her environment. Thus, to identify with other people and feel part of a much wider community, sharing a set of values and beliefs, is highly relevant for promoting behavior change.
Indeed, previous research has found that self-efficacy and social support are related to patterns of physical activity in people with type 2 diabetes. 12
Accordingly, our research has aimed to advance the study of these psychological variables and to analyze their possible relationship with some data provided by participants in the BBT.
Thus, our first objective was to analyze whether the change in levels of blood sugar that occur after participation in the BBT is related to participants' perception of self-efficacy and social support. The second objective was to explore whether, after participation in the BBT, people expressed an explicit intention to practice physical activity regularly. Finally, the third objective was to determine whether insulin-dependent and non–insulin-dependent participants demonstrated differences in their perception of self-efficacy, social support, or intention to exercise.
Materials and Methods
Participants
In total, 3,916 people with diabetes completed the BBT, of whom 78.8% were insulin users. The program did not collect demographic data, so we do not have information about age, gender, or ethnicity of the participants. As the main objective of the initiative was to show the impact that small changes can have on health, we considered it more suitable not to ask for individual characteristics; this would have made the test more complex, and it would have discouraged participation.
Procedure
A specific publicity campaign for the Big Blue Test that was launched before the campaign was rooted in various online social networks. In parallel, a specific Web site for the Big Blue Test was launched (
Once a person decided to participate in the Big Blue Test, he or she was given visual and clear information on the four steps involved: “Test your blood sugar,” “Get active,” “Test your blood sugar again,” and “Share.”
The data were collected in one of two ways: (1) individuals doing the BBT entered their results on the Web site 1. If they had diabetes 2. The type of physical activity done (ranging widely from walking to martial arts to yoga) 3. Their blood glucose readings before and after 14 min of exercise 4. If they were insulin users or not.
13
Additionally, everyone taking part had to answer four questions about behavior intentions and his or her feelings about participating in the test. These questions were designed in order to evaluate the perceived self-efficacy of participants, perceived social support, and their stated intention to change their behavior in the future.
Questions were rated on a 5-point Likert scale. The four questions were: Q1. “After doing The Big Blue Test, I feel more able to manage my diabetes.” Q2. “After doing The Big Blue Test, I feel more able to develop healthy habits to help manage my diabetes.” Q3. “After doing The Big Blue Test, I feel closer (more connected) to other people with diabetes.” Q4. “After doing The Big Blue Test, I intend to exercise regularly to help control my diabetes.”
The first two questions refer to participants' perception of their self-efficacy, defined as the self-confidence to change a health risk behavior through personal action. 14 The BBT aims to show the importance of physical activity in the context of diabetes and, ultimately, attempts to modify the behavior of participants toward a healthier lifestyle, through promoting physical exercise. In this context, self-efficacy can be a highly relevant variable.
The third question is linked to the perception of social support. Given that the BBT is done through the Diabetes Hands Foundation community, during the design of the test we considered it of interest to introduce this question to determine the relationship among social support, self-efficacy, and changes in blood glucose level.
The last question refers to the person's motivation for change (i.e., his or her intention to change a behavior to another that is healthier). After doing the BBT, the participant sees how just 14 min of exercise decreases the blood glucose level, which can motivate him or her to adopt this healthy practice. In doing the BBT, the participant increases his or her expectancy of the positive effects of exercise (i.e., he or she has objective proof of the positive results that the new behavior will have on his or her health).
Data Analysis
In order to study the importance of perceived self-efficacy and social support, we quantified the strength of the relationship between each question in relation to (1) the type of exercise, using Cramer's V, (2) the changes in blood sugar level, using analysis of variance and follow-up tests, and (3) being insulin-dependent or not, also using Cramer's V. We also analyzed the relationship between being insulin-dependent or not and changes in blood sugar level (Welch's test, Cohen's d, and mixed factorial analysis of variance).
The statistical software package SPSS for Windows (version 19; SPSS Inc., Chicago, IL) was used to carry out all these analyses.
Results
Perceived Self-Efficacy and Its Relationship to the Type of Exercise
For the two questions “After doing the Big Blue Test, I feel more able to manage my diabetes” and “After doing the Big Blue Test, I feel more able to develop healthy habits to help manage my diabetes,” we applied the Cramer V measure. The results were as follows: (1) V=0.062 (p=0.106) and (2) V=0.066 (p=0.034). For the two cases, the Cramer V values were very low, so we can say that the two variables were effectively not related.
Perceived Self-Efficacy and Its Relationship to the Difference between Initial Glucose Levels and Final Glucose Levels
Responses to Questions 1 and 2 were used as the main variable in order to make groups, following which we compared those who responded to each of the five options in terms of the difference between the initial glucose levels and final glucose levels using an analysis of variance.
Question 1
Figure 1 plots the 95% confidence intervals for each of the alternative responses to this question. Participants who perceived less self-efficacy with respect to Question 1 were those who reduced their blood glucose levels to a lesser extent: strongly disagree (−21.30 to 20.25), disagree (−46.00 to −16.51), neither agree nor disagree (−33.81 to −28.13), agree (−36.96 to −32.15), and strongly agree (−34.73 to −31.59).
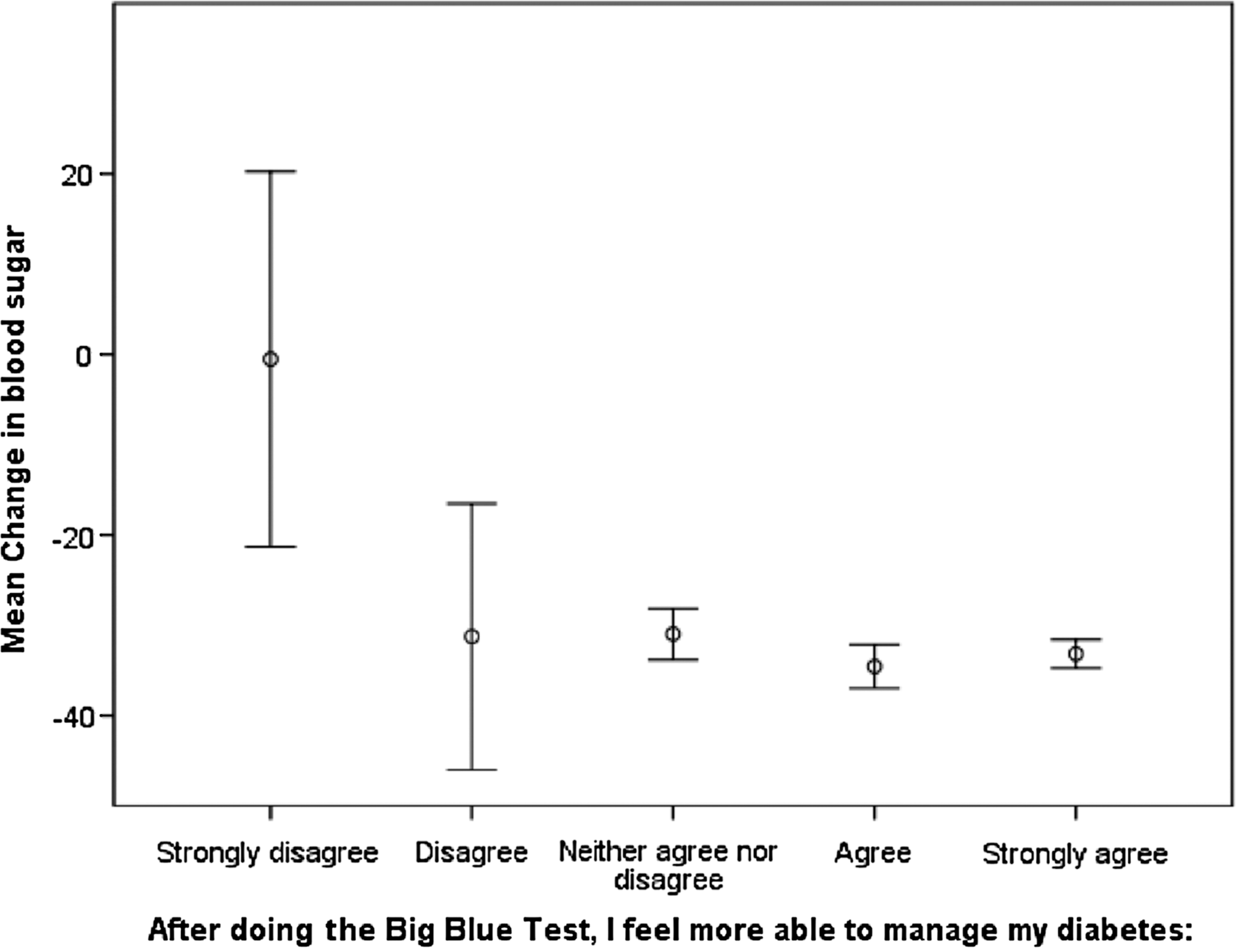
Responses to the statement “After doing the Big Blue Test, I feel more able to manage my diabetes.” Error bars are the 95% confidence interval.
Using Dunnett's T3 test, we compared pairwise those who responded “Strongly disagree” with the rest, and we found differences only with those responding “Agree” (p=0.021) and “Strongly agree” (p=0.029).
Question 2
As in Question 1, with confidence intervals of 95% for each of the alternative responses to this question (Fig. 2), the participants who perceived lower self-efficacy regarding this item reduced their blood glucose levels to a lesser extent: strongly disagree (−25.00 to 12.64), disagree (−40.29 to −15.05), neither agree nor disagree (−33.46 to −27.10), agree (−38.03 to −32.60), and strongly agree (−34.43 to −31.44).
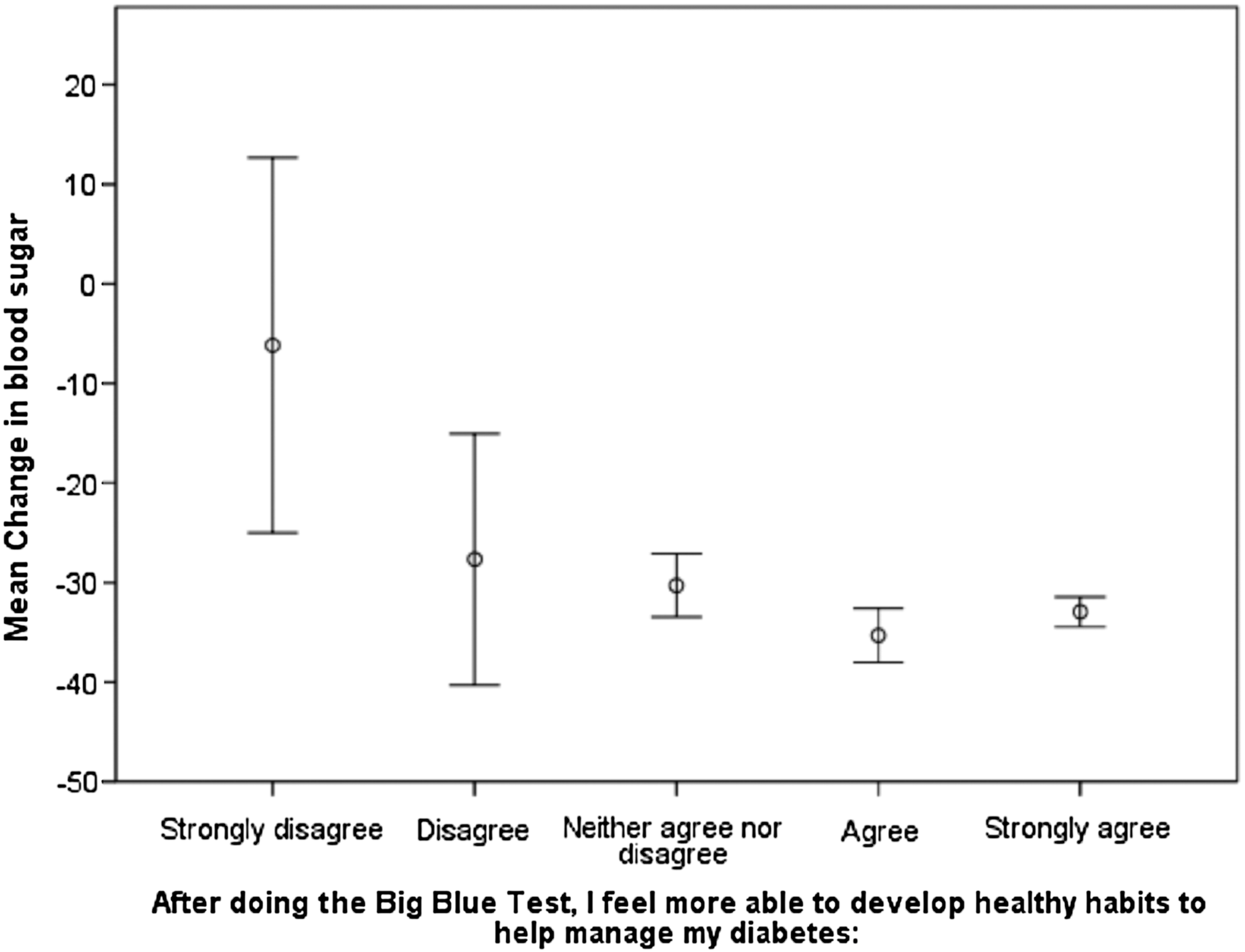
Responses to the statement “After doing the Big Blue Test, I feel more able to develop healthy habits to help manage my diabetes.” Error bars are the 95% confidence interval.
Using Dunnett's T3 test, we made a pairwise comparison of those who responded “strongly disagree” with the rest, and we found differences only with those responding “agree” (p=0.036).
Perceived Social Support and Its Relationship to the Difference between Initial Glucose Levels and Final Glucose Levels
Results for Question 3 (means, with 95% confidence intervals for each of the alternative responses) suggest that people who perceived less social support had a smaller decrease in glucose levels. As the values were quite close and the confidence intervals overlapped significantly, we decided to carry out the Brown–Forsythe test (p=0.157), which proved them not to be significant.
Being Insulin-Dependent or Not and Its Relationship to the Difference Between Initial and Final Glucose Levels
As the assumption of homogeneity of variances was not satisfied, we applied Welch's test, and the result was statistically significant: t(1748.402)=9.507; p<0.001. It is therefore highly unlikely that the two populations (insulin-dependent and non–insulin-dependent) have the same mean difference between initial and final glucose levels. Based on the descriptive results (123.26 mg/dL after exercise versus 158.4 mg/dL before exercise for insulin users and 116 mg/dL versus 139.01 mg/dL, respectively, for non-insulin users), we know that there is a greater decrease in glucose in insulin-dependent participants (−35.14 mg/dL versus −23.01 mg/dL).
At the population level, the 95% confidence interval shows that these differences should be between 9.63 and 14.64.
To obtain indicators of effect size, we calculated the standardized mean difference (Cohen's d). The value of d=0.33 shows that the insulin-dependent group had a reduction in glucose level 0.33 standard deviations higher than the non–insulin-dependent group.
A mixed factorial analysis of variance was carried out to compare the two groups (insulin-dependent and not) at both times of glucose measurement (before and after exercise). In this case, the significant interaction (F of the Greenhouse–Geisser correction=63.409, p<0.001) indicates that the change in glucose level for the insulin-dependent participants was not the same as for the non–insulin-dependent participants. The reduction is more pronounced for the insulin-dependent individuals (Fig. 3). Moreover, although non–insulin-dependent individuals had a lower initial blood glucose level, the difference between their level after exercise and that of the insulin-dependent subjects was reduced.

Responses to the question “Do you use insulin?”
Perceived Self-Efficacy and Its Relationship to being Insulin Dependent or Not
Question 1
The chi-squared test of independence indicates that the two variables are significantly related (χ2=47.193; p<0.001; Cramer V=0.110).
Specifically, and according to the contingency table (Table 1), more insulin-dependent participants disagreed (strongly or otherwise) with the statement than could be explained by chance. Additionally, more non–insulin-dependent participants agreed (strongly or otherwise) with the statement, and fewer disagreed (strongly or otherwise), than would have been expected if the variables had not been related.
Contingency Table for Responses to “After Doing the Big Blue Test, I Feel More Able to Manage My Diabetes”
Question 2
The independent chi-squared test of independence indicates that the two variables are significantly related (χ2=51.633; p<0.001; Cramer V=0.115).
When we look at the contingency table (Table 2), we see that this relationship is expressed by more insulin-dependent participants disagreeing with the statement than would be expected by chance. Additionally, more non–insulin-dependent participants were in complete agreement with the statement than what would be expected if the variables were related.
Contingency Table for Responses to “After Doing the Big Blue Test, I Feel More Able to Develop Healthy Habits to Help Manage My Diabetes”
Perceived Social Support and Its Relationship to being Insulin Dependent or Not
The independent chi-squared test of independence indicates that the two variables are significantly related (χ2=10.396; p=0.034; Cramer V=0.052).
As in the previous cases, this relationship is expressed through more insulin-dependent participants disagreeing (strongly or otherwise) with the wording of the statement than would be expected by chance. Additionally, more non–insulin-dependent people were in full agreement with the statement than were in disagreement (strongly or otherwise) than would be expected if the variables were not related (Table 3).
Contingency Table for Responses to “After Doing the Big Blue Test, I Feel Closer (More Connected) to Other People with Diabetes”
Intention to Exercise and Its Relationship to being Insulin Dependent or Not
Question 4
The independent chi-squared test of independence indicates that the two variables are significantly related (χ2=54.581; p<0.001; Cramer V=0.118).
According to Table 4, this relationship is expressed by more insulin-dependent participants in disagreement (strongly or otherwise) with the wording of item than can be expected by chance. Additionally, more non–insulin-dependent participants were in strong agreement and fewer in disagreement (strongly or otherwise) than would be expected if the variables were not related.
Contingency Table for Responses to “After Doing the Big Blue Test, I Intend to Exercise Regularly to Help Control My Diabetes”
Intention to Exercise and Its Relationship to the Difference Between Initial and Final Glucose Levels
Figure 4 plots the 95% confidence intervals for each of the alternative responses to this question. It suggests that people who express no intention to exercise are those with a smaller reduction in their levels of glucose. However, the difference is not very clear because the difference between initial and final glucose levels for people who answer “disagree” is greater than for those who agreed with the assertion: strongly disagree (−44.19 to 18.92), disagree (−63.15 to −21.89), neither agree nor disagree (−32.23 to −24.57), agree (−35.82 to −30.18), and strongly agree (−34.80 to −31.91).

Responses to the statement “After doing the Big Blue Test, I intend to exercise regularly to help control my diabetes.” Error bars are the 95% confidence interval.
In this case, it is even more important to test statistically whether there are differences between the groups.
The homogeneity of variances was not met, so we again applied the Brown–Forsythe test (asymptotically distributed F=2.065, p=0.093). The result was not statistically significant.
Discussion
These results show that those participants who reduced their blood glucose levels the least after exercise were those who expressed a lower perception of self-efficacy in managing their diabetes and in developing healthy habits to help manage their condition. Similarly, the participants who reduced their blood glucose the least after exercise were those who perceived less social support. The results also suggest that the type of exercise performed by participants was not related to their perceived self-efficacy.
However, if we consider if participants are insulin-dependent or not, the picture becomes more complex because the relationship among perceived self-efficacy, social support, intention to exercise, and being or not being insulin-dependent is statistically significant. Although insulin-dependent participants reduced more their glucose levels after 14 min of exercise compared with non–insulin-dependent participants, the former felt less able to manage their diabetes, less able to develop healthy habits, less intent on exercising regularly, and perceived less social support. In other words, for those who were insulin-dependent, it is their condition (being insulin dependent) and not the change in blood sugar level that was the most determining variable in perceived self-efficacy and social support, as well as in intention to exercise regularly. In this sense, Brazeau et al. 15 have studied the main barriers that patients with type 1 diabetes face regarding physical exercise and have indicated that the strongest barrier is the fear of hypoglycemia, arguing that these patients need information and support in hypoglycemia management. Overall, it seems clear that insulin-dependent people should be considered a particularly important population when designing and implementing programs to promote awareness about their role as agents of their own health and their self-management, incorporating diabetes-specific actions to prevent hypoglycemia.
Another important implication of the data presented in this study is for understanding and dealing with intention. Intention has not been shown to have a relation with observable changes in glucose levels, contrary to what had been expected. These changes in glucose levels show objectively and in the short term the consequences of physical exercise on blood glucose level; therefore it was to be expected that when these changes were greater, participants would have a higher level of motivation to introduce this behavior regularly in their daily lives. However, this was not the case.
This could be due to the fact that for the introduction of a new health behavior, it is not enough that there is merely a high perception of self-efficacy or a clear awareness of the benefits to be gained with the new behavior. Although these are certainly necessary conditions, they are not sufficient in themselves, and it is important to consider what other variables might influence the development of an intention to further action and its later implementation and maintenance. Some of these variables could include the locus of control (i.e., if we attribute causality to internal factors related to ability and effort, or external factors relating to luck or chance), social norms (i.e., pressure to act a certain way), or control (the extent to which we believe a behavior is under our personal control). It is for this reason that, when intending to implement a program of self-management, it is essential to both make an action plan—to plan how to carry out the action—and monitor the action—to oversee and adjust the implementation and maintenance of this plan. 16,17
This study is limited as these data cannot be generalized to the entire diabetic population, due to the fact that the participants in the experiment are, first, volunteers—the volunteer effect is well known in Internet studies 18 —and, second, people who are accustomed to being online. So, rather than being a sample of patients with diabetes, they are instead a sample of e-patients with diabetes. Furthermore, we did not have data on the type of diabetes the participants had, so a comparative analysis of this variable was not possible. It is important to note that the BBT has a very limited duration in time and that its purpose is solely to promote awareness and a sense of belonging in a specific community.
In conclusion, for a health behavior such as exercise to be become a habit in people with diabetes, it is necessary to consider not only crucial physiological variables (e.g., changes in blood sugar level or being insulin-dependent or not), but also those psychological variables that have clearly affected behavior change. As we have revealed through the data in this study work, awareness of the benefits of exercise does not predict behavior change, as the physiological changes that individuals with diabetes can experience after exercise does not promote, directly, such a change. For this reason, interventions in this area should not only aim to raise awareness of the benefits of the new behavior, but also involve self-efficacy and social support in order to establish programs that allow control and maintenance of future health behaviors.
Footnotes
Acknowledgments
The authors are grateful to Rumen Manolov, University of Barcelona.
Disclosure Statement
No competing financial interests exist.
B.G-Z., M.P., M.M.H., and M.A. contributed to the conception and design of the project. B.G.-Z. took the lead in data analysis, and E.G. helped in this analysis. M.M.H. and S.C. researched data. B.G.-Z. and M.P. wrote the manuscript. M.A. contributed to the discussion and reviewed/edited the manuscript. B.G.-Z. and M.M.H. are the guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.