
Abstract
Introduction
Limited access to skilled psychiatric care for children, especially access to child psychiatrists, is a major systems problem. 1,2 Although half of all lifetime mental illness begins by 14 years of age, less than a quarter of these children are identified and treated. 3,4 Specialists like child psychiatrists are poorly distributed and thus are difficult to access in rural and low-income areas. 2
Without quality service access, a child's treatment plan might over-rely on the use of psychiatric medications. State and federal agencies are investigating if this is one reason why children with Medicaid coverage are more likely than other children to receive psychotropics, as well as twice as likely to receive antipsychotics. 5,6 Increased prevalence of children receiving psychiatric medications at very high doses or at a very young age is a concern when that use is ineffective or creates unnecessary side effects. 7 –9 Concerns like these have led to all U.S. states now being required to monitor psychiatric medication use for children in foster care. 10
The demand for child psychiatric hospitalizations increases when local services are limited, when the child is living in a rural location, or when the child is receiving fewer community services. 11,12 Receiving appropriate mental health services and high-quality treatment planning may, in turn, reduce intensive and unnecessary child psychiatric inpatient care. 13
Telepsychiatry addresses regional access and care quality challenges like those described above. Outcome studies show that child telepsychiatry assessment and treatment compare favorably with in-person care. 14,15 Although telepsychiatry systems include additional technology and administrative costs, reductions in patient transportation costs and provider overhead may offset these expenses. 16 –18 Because insurers and payers may not be directly responsible for those transportation expenses, the payer appeal of telepsychiatry increases if or when cost savings for health systems are identified.
Wyoming is a large and very rural state, with the smallest total state population and only 6 residents per square mile (the U.S. state average is 87 per square mile). 19 In 2010, Wyoming state agencies identified three areas of concern: (1) child psychotropic medications prescribed at high doses, in high numbers, or for children under 5 years of age; (2) long-term psychiatric hospitalizations suspected as due to poor community child psychiatrist access; and (3) primary care providers requested additional child mental health supports. Long-term psychiatric hospitalization in psychiatric residential treatment facilities (PRTFs) was a particular concern because the state's total number of reimbursed bed days had increased by 54% between Fiscal Years 2008 and 2010. 20
Wyoming responded to these issues by engaging a team of University of Washington–based telemedicine-focused child psychiatrists to deliver rapid access consultation services in a coordinated system that would address all of these above concerns. This article reviews outcomes of that consultation service.
Materials and Methods
Wyoming Medicaid engaged a team of telemedicine child and adolescent psychiatrists at its regional affiliated medical school, the University of Washington School of Medicine. This centrally administered, three-part consultation service started January 2011.
1. Televideo consults for Multidisciplinary Teams (MDTs). Foster care caseworkers requested rapid-access televideo patient appointments when a long-term inpatient or residential stay was being arranged by the local MDT, or when a second opinion was needed for other reasons. Consultants provided a record review, an approximately 30-min telephone conference with the caseworker, a 1.5–2-hour patient appointment during business hours using dedicated videoconference equipment in local foster care offices, follow-up with the caseworker, and a detailed final report within 5 business days. MDT preconsult placement plans were recorded at the time of consult for tracking.
2. Medication reviews (second opinion). Age and dose thresholds were created in the Medicaid outpatient medication authorization system that automatically triggered requests for rationale and supporting documentation from the prescriber, as detailed at the
3. Elective telephone consultations (Partnership Access Line [PAL]). All medical providers in Wyoming were given immediate telephone access to a child psychiatrist who they could call to consult on any of their patients on weekdays 9 a.m.–6 p.m. The PAL service further provided referral assistance and televideo consult appointments upon request.
21
PAL consultants hosted free regional Category I educational conferences about best practice mental healthcare, referencing a peer-reviewed care guide that was sent to all primary care providers (the guide is also free at
Consultants recorded all service characteristics in a Microsoft® (Redmond, WA) Access® database in their usual workflow. An aggregated query of this database was performed on all three types of consults from January 1, 2011 to March 31, 2013 regarding demographics, service characteristics, and recommendations. For televideo MDT consults, placement histories for each child 6 months after his or her consult were obtained from the Wyoming Department of Family Services, as well as all outpatient claims data from Wyoming Medicaid. Overall cost calculations used the state's 2013 PRTF average daily rate and 2013 outpatient CPT code rates. Wyoming Medicaid reported its state psychiatric medication utilization rates and costs for its entire Medicaid population for state Fiscal Years 2010–2014. Pearson's chi-squared test was used for significance of change tests. This overall analysis procedure was approved for exempt review by the Seattle Children's Institutional Review Board. Community providers had no charge for receipt of any consult services as all program funding came from the Wyoming Department of Health.
Results
There were 229 televideo MDT consults, 125 second opinion reviews, and 277 elective PAL consults performed (Table 1). One hundred thirty-one community providers attended one of nine child mental health educational conferences.
Patient Demographics
Four percent of Partnership Access Line (PAL) callers did not report their patients' age and sex.
MDTs, Multidisciplinary Teams.
Televideo Consults for MDTS
Consultations were completed an average of 3.3 business days from caseworker request. Each patient had a mean of three different diagnostic issues, with disruptive behavior disorder (52%), depressive disorder (44%), attention-deficit hyperactivity disorder (39%), posttraumatic stress disorder (36%), and anxiety (28%) as the most common. Consultants recommended a mean of three different new psychotherapy or psychosocial interventions per patient. They also recommended to either start or increase a medication in 57% of cases and recommended to either stop or decrease a medication in 39% of cases.
One hundred forty-one of the referred children (62%) had been planned by their local team to enter a PRTF long-term hospitalization before their consult. Placement records found only 57 of this subgroup of 141 children (40%) were subsequently admitted to a PRTF during the next 6 months postconsultation, for a mean duration of 4.5 months. The remaining 84 children went to family homes (53%) and other group residential care settings (47%). The hospitalized children had mean inpatient and outpatient combined expenditures of $48,085.53 per child over the next 6 months postconsult. The remaining 84 children in this group who were not PRTF-admitted (redirected into other forms of care such as new outpatient services) had mean combined inpatient and outpatient expenditures of $18,538.48 per child over the next 6 months postconsult. These figures entered a return on investment calculation (Table 2).
Cost Analysis for Televideo Multidisciplinary Team Consults
Findings reflect outcomes of 141 children being processed into a psychiatric residential treatment facility admission prior to consultation.
MDT, multidisciplinary team; PAL, Partnership Access Line.
Mandatory Medication Review Consultations (Second Opinion)
Medication reviews were requested for high dose (60%), young age (37%), or polypharmacy (3%) criteria. Reviews occurred primarily with psychiatrists (48%), primary care providers (40%), or psychiatric nurse practitioners/physician assistants (6%). In two-thirds of reviews, continued authorizations of the medication as prescribed were recommended. In one-sixth of reviews, temporary authorizations of the medication were recommended to allow planned medication changes and dose adjustments to occur. In the remaining one-sixth of reviews, immediate changes to the prescribing plan were recommended because of safety or best practice concerns.
Elective Telephone Consultations (PAL)
Elective consult callers were primarily primary care providers (77%), although psychiatrists, psychiatric nurse practitioners, therapists, and system administrators also called. Calls averaged 16.5 min and were most often about children with Medicaid insurance (59%). Patients received a mean of 1.4 psychotropics at the time of the call. In 27% of calls, a medication start was recommended, whereas in 16% a medication stop was recommended. The child and adolescent psychiatrist recommended new nonmedication interventions, such as behavior management training, in 84% of calls.
State Medication Prescribing Trends
From the start of the service through July of 2013, the total statewide percentage of children with Medicaid receiving psychotropics remained stable at 9.1%. However, the number of children ≤5 years old prescribed psychotropics decreased 42% (p<0.001), the number prescribed doses >150% of the adult Food and Drug Administration (FDA) maximum decreased 52% (p<0.001), and the number of children prescribed five or more concurrent medications decreased nonsignificantly, by 14% (p=0.596) (Table 3 and Fig. 1). Among children in foster care, there was a 54% decline in use of psychotropics at doses >150% of the adult FDA maximum (p=0.023). With inflation adjustment (to use 2013 dollars), state expenditures on psychotropics for youth ≤21 years of age decreased during this time frame by approximately $209,500, which is greater than the $29,375 cost of performing these mandatory medication reviews. 22
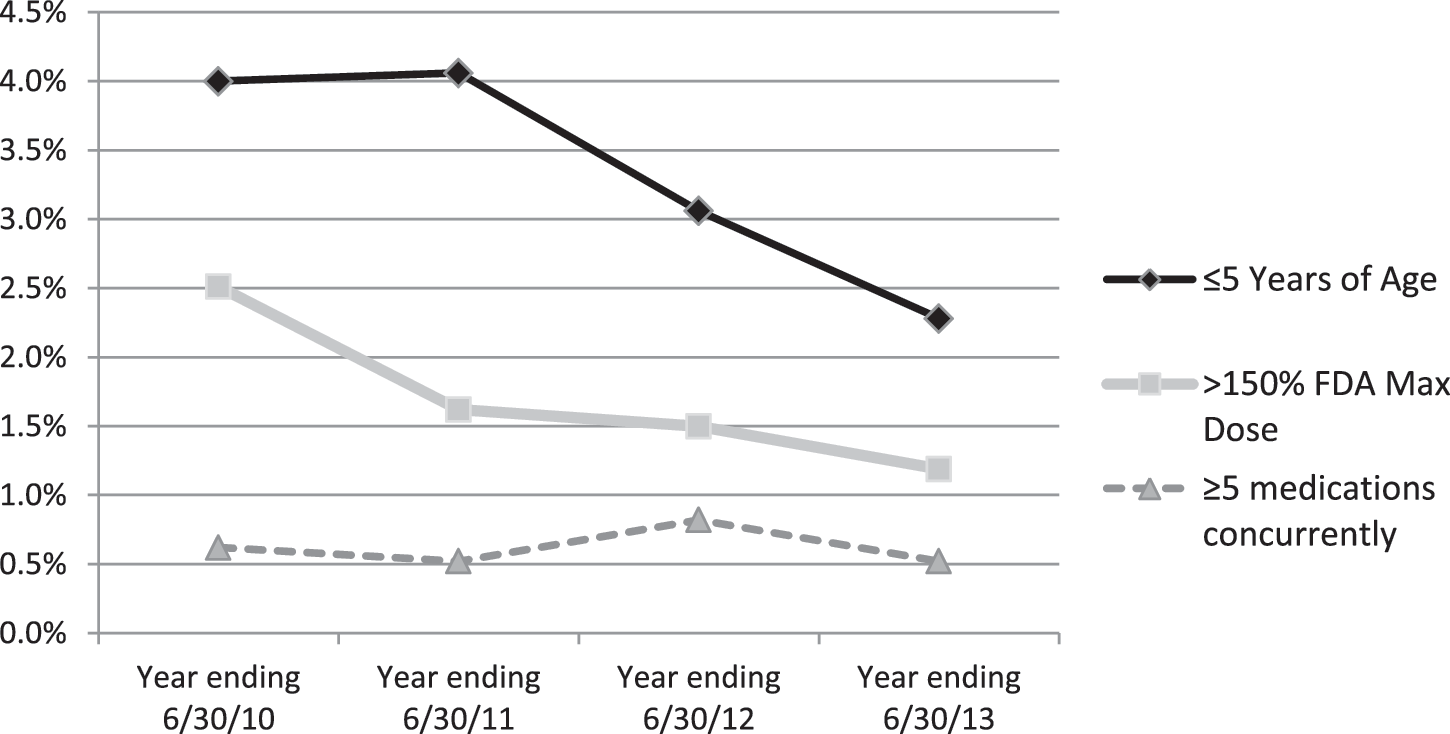
All Medicaid psychiatric medication users ≤21 years of age. FDA Max, Food and Drug Administration maximum.
Medicaid Psychiatric Medication Utilizers ≤21 Years of Age
For unduplicated clients during the stated state fiscal year.
p value from Pearson's chi-squared test, relative to reference point of the state fiscal year ending June 30, 2010 (before consult services began).
FDA, Food and Drug Administration.
Provider Feedback
The Wyoming Medicaid Director obtained the following provider feedback on medication second opinions: “The physicians said they really appreciated [medication reviews], even though it cut a bit into their work flow, as they were challenged to defend their decision, they often changed their therapy after consultation, or if Seattle agreed with the decision it gave them greater confidence.” Foster care case workers receiving MDT consults offered similarly positive feedback about their experiences. Provider feedback on elective PAL consults was uniformly positive and similar in nature to findings in another state. 21 Examples of specific written feedback from Wyoming providers include: “PAL is a lifesaver”; “This consultative service is unique and invaluable!”; and “I'm so grateful for your service!”
Discussion
Unlike the growth in pediatric psychotropic use seen elsewhere nationally, psychotropic use among Wyoming's Medicaid children did not grow after these teleconsult services started. 5,23 Furthermore, significant reductions in medication use were found in two key categories of concern. After the intervention only about half as many Medicaid children under 5 years of age were using any psychotropics, and about half as many were using high doses (>150% of the adult FDA maximum) of psychotropics. For the subgroup of children in foster care, the same significant decline was found in high-dose users. Clinically, this was an excellent outcome in decreasing unnecessary exposure to psychotropic medication side effects.
Mandatory medication teleconsultations are an obvious contributor to the above psychotropic use changes, but they should not be viewed as solely responsible. For instance, only 20% of all Medicaid users <5 years of age were ever the subject of a medication review, and of these, only 34% received a medication change recommendation. Other contributors include prescribing habits changing to avoid triggering new reviews once the review system was established. 24 Elective PAL teleconsults, regional educational conferences, and use of the care guide may have changed prescribing habits by educating providers about appropriate medication use and other nonmedication treatment strategies. Finally, televideo MDT consultations shaped prescribing and care plans for children with particularly high service needs. Although it is possible that additional unaccounted-for changes may have influenced prescribing in this state, all of these coordinated teleconsultation services were influential and linked in timing to the changes in community prescribing.
Prior to initiation of services, it was difficult to obtain a skilled child psychiatrist's assessment and treatment plan for a child heading toward long-term PRTF hospitalization in this rural state with few child psychiatrists. Adding quick academic center–affiliated telemedicine evaluations into the care pathway greatly impacted the MDT court hearing and placement process that directs children into residential care and hospitalizations. After implementation, a majority of the consulted children who would have otherwise been sent away for a (mostly out-of-state) PRTF admission instead received clinically appropriate treatment plans that could be implemented in their home communities instead. This is good for foster care children in that maintenance of a child's family and community connections is a well-recognized way to improve long-term foster care outcomes. 25
Decreasing the need for PRTF admissions also creates significant Medicaid cost savings. Because rapid-access televideo MDT consultations would not have been possible without the guaranteed consultant availability provided by PAL, the costs of both elective PAL and televideo MDT consult services need to enter the return on investment calculation. Therefore, after accounting for all related costs, a 1.82 to 1 return on investment was found for Wyoming Medicaid (Table 2). Positive community feedback about these services further supports their utility.
A limitation in the savings calculation is that despite evidence from past experience, it is an assumption that every child referred for a PRTF admission confirmation would have gone on to be PRTF admitted if not for the advice of the televideo consultant. This possible overestimate should be considered in the context of other systems changes that resulted in cost savings not included in the return on investment. For instance, the observed reduction in total state medication expenditures was not included because of less certainty in attributing the change to these programs. There is also educational impact, in that MDT members and community providers would learn more appropriate treatments to use earlier with future patients, which would predictably prevent the need for higher-level care later. Program-supported primary care-led mental health care in rural communities also fulfills a key “stitch in time” role to prevent patient deteriorations to the point where PRTF admissions or outlier prescription strategies might be needed.
Conclusions
Changes in pediatric medication use and long-term psychiatric care placements occurred in Wyoming following implementation of a coordinated teleconsultation program with child and adolescent psychiatrists. Clinically important outcomes included a reduction in both preschool-age and high-dose pediatric psychotropic prescribing, as well as increased maintenance of high-service-need children in community-based treatments. A cost analysis revealed that these teleconsult programs had a significant net fiscal savings of a 1.82 to 1 return on investment. In addition to financial benefits, feedback from the provider community was very positive. In sum, the Wyoming child telepsychiatry consultation program shifted mental health treatment of children toward best practices, provider satisfaction, and cost efficiency. Linking three complementary telepsychiatry programs together efficiently uses psychiatrist time to provide broad specialist access and substantially impactful outcomes. Other states or large health systems with concerns about child psychotropic medication use patterns or community mental health service quality may want to consider replicating Wyoming's programs.
Footnotes
Disclosure Statement
No competing financial interests exist.