
Abstract
Introduction
The concept of healthcare continues to change. Due to the economic imperative to restrain rising healthcare costs, in the context of an aging community and the extraordinary changes in communication technology, different kinds of telemedicine services have made their entry into healthcare. 1 There is not one definitive definition of telemedicine, 2 but according to the World Health Organization, telemedicine services are healthcare services where information and communication technologies are used by healthcare professionals to exchange information for the treatment of a patient. 3 Alongside the potential to lower healthcare costs, telemedicine services have the potential to increase the accessibility and quality of care. 4,5
This article focused on a telerehabilitation service for physical exercise, designed and implemented as partial replacement of a 3-day outpatient group multidisciplinary rehabilitation program (RP) for patients with chronic lower back pain (CLBP) or pulmonary disease (PD). This service makes use of a notebook with a Webcam and consists of two treatment modules. Module 1 contains a database of exercise videos to increase strength, balance, flexibility, and endurance. Module 2, a teleconference service, facilitates contact between patient and therapist. Within these modules, the therapist remotely composes an individually tailored exercise program and supervises the patient. The patient and therapist contacted each other weekly by teleconference or would meet each other during the remaining 2 days to discuss the rehabilitation progress. Based on the experience and rehabilitation progress, the therapist updated the exercise program weekly. During the first 2 weeks (for CLPB) or 4 weeks (for PD) the patients visited the clinic for 3 days and received, in addition to their RP, training (1 h/week) on how to use the exercise-based telerehabilitation service. From the third (for CLBP) or fifth (for PD) week on, the telerehabilitation service was delivered to the patients as partial replacement; 1 day at the clinic was replaced by 1 day of rehabilitation in their own environment. The overall RP lasted 7 weeks for the CLBP patient and 12 weeks for the PD patient, and the telerehabilitation service was used for 5–8 weeks of this program.
An earlier article showed that this service is as effective as the conventional outpatient RP. 6 In face-to-face physical rehabilitation there is increasing evidence that intensive programs (high use levels) are more effective for the health outcome than programs with a lower level of intensity (low use levels). 7 As telerehabilitation services 8 –10 give patients the opportunity to rehabilitate independently from their therapist, the intensity of training is much more controlled by the patient instead of by the professional, and as such it is interesting to investigate what is the actual use and whether it is the case that this (hypothesized) higher use is also related to better outcomes.
This association between use and clinical benefit has been the topic of some articles. According to Hermens et al., 11 chronic stroke patients with high training intensity had better improvement of arm/hand functions using an exercise-based telerehabilitation service. Huis in ‘t Veld et al. 12 showed that chronic pain patients who used a telerehabilitation service more often (i.e., expressed in the number of hours) had higher clinical benefit in pain relief. These findings were verified by Rho et al. 13 Their article showed that high compliance has a positive impact on the clinical outcome.
However, in these articles the telemedicine service was delivered to the patients (service configuration) as an autonomous treatment 12,13 or as follow-up treatment. 11 In none of these articles was the telemedicine service delivered to the patients as a partial replacement of face-to-face physical rehabilitation. To the present authors' best knowledge, there are no studies so far that have investigated the use of telemedicine service when delivered as a partial replacement of face-to-face physical rehabilitation, and as such it is unknown whether in this case higher use is related to better clinical outcome. For this reason the aim of this article is to examine the use pattern of the exercise-based telerehabilitation service implemented as partial replacement for a 3-day outpatient group multidisciplinary RP for patients with CLBP or PD and to examine the association between actual use and clinical benefit experienced by the chronic disease patients. To gain insight in the generality of the actual use and association between actual use and clinical benefit experienced by the chronic disease patients, two pathology groups are included.
Materials and Methods
Patients were recruited by the Roessingh Center for Rehabilitation, Enschede, The Netherlands. CLBP and PD patients referred to the physical outpatient RP were asked to participate. Patients were included when they had sufficient understanding of the Dutch language and were older than 18 years of age. The appropriate ethics committee approved the study. All patients gave their informed consent prior to participation.
Measurements
Actual use of the service
Actual use was expressed as frequency and duration of use. These data were obtained from the service log files that store the duration of each single session time between log-in and log-out. These log files were used to gain insight into: • The number of weeks that patients used the service • The frequency and duration of use expressed over weeks combined as well as per week.
For sessions longer than 2 h only the frequency data were included in the analysis. The duration date was eliminated, due to it being unlikely that patients will exercise longer than 2 h in one session. It was assumed that in these cases patients forgot to log-out. The sessions shorter than 2 min were excluded, due to the average duration of an exercise video being 2 min and in smaller intervals patients were not able to exercise.
Clinical benefit
Measurement on clinical benefit focused on complaints (pain or dyspnea) and physical functioning. Complaints and physical functioning were assessed pretest (in the first week of the outpatient RP) and posttest (in the last week of the outpatient RP).
Patients were asked to rate their level of pain for CLBP patients and level of dyspnea for PD patients during the previous week. Levels of pain and dyspnea were assessed on a visual analog scale (VAS). The VAS consists of a 10-cm horizontal line with “no discomfort at all” on the left and “as much discomfort as possible” on the right extremity of the line. 14,15
To assess physical functioning the CLBP patients also completed the Roland Disability Questionnaire (RDQ). 16 This questionnaire is an illness-specific 24-item functional assessment questionnaire that is frequently used for back pain. In this article the Dutch version 17 of the RDQ is used. The PD patient performed a 6-min walk test (6MWT). 18 The objective of the 6MWT is to walk as far as possible (in meters) for 6 min on a flat surface.
Data Analysis
Demographic characteristics and actual use (frequency and duration of use) are described in terms of mean (standard deviation [SD]) or percentage. The compliance to the telerehabilitation service is presented as the percentages of compliant users per week. Outcome for clinical benefit is described in terms of means (SD), with the significance of differences between pre- and posttest outcome being assessed by a paired t test. To investigate the relation between actual use of the intervention and clinical benefit, changes in complaints and physical functioning level were calculated, taking the difference between the pre- and posttest outcome. The correlation between frequency of use, duration of use, and changes in VAS for pain, VAS for dyspnea, RDQ, and 6MWT were examined. The statistical significance level was set at p<0.05 for all analyses. A standard software package (SPSS Inc., Chicago, IL) was used for statistical analysis.
Results
In total, of 104 patients who were asked to use the exercise-based telerehabilitation service during their outpatient RP, 81 patients started the introduction on how to use the exercise-based telerehabilitation service. In total, 19 patients dropped out: 8 patients after the introduction and 11 during the further treatment weeks. The main reasons for dropping out were discontinuation of the treatment due to an exacerbation (n=8), personal circumstances, such as lack of time or motivation (n=7), and problems with the equipment (n=4). Thus, 62 patients (CLBP, n=33; PD, n=29) (85%) finished the outpatient rehabilitation using the exercise-based telerehabilitation service. The demographic characteristics of these patients at baseline are presented in Table 1. There were no significant differences in demographic characteristics and pretest outcomes on complaints between these patients and patients who dropped out after inclusion (n=19) (p≥0.174). Figure 1 presents a flowchart of the recruitment and numbers of patients using the service over the treatment week for both pathologies.
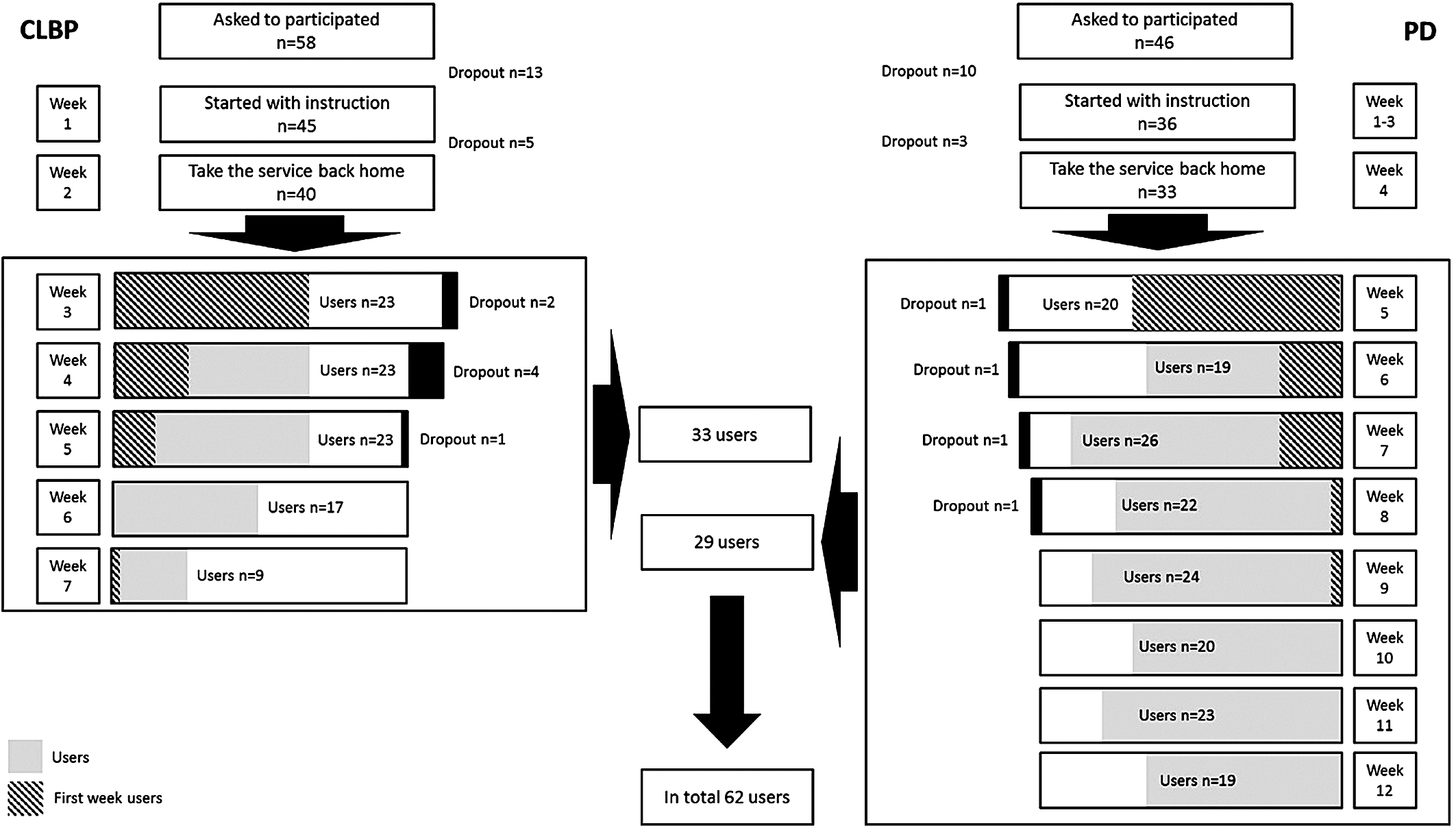
Flowchart of recruitment and users over the treatment week for both pathologies. CLBP, chronic lower back pain; PD, pulmonary disease.
Demographic Characteristics at Baseline for Chronic Lower Back Pain Patients, Pulmonary Disease Patients, and All Patients
CLBP, chronic lower back pain; PD, pulmonary disease; SD, standard deviation.
Actual Use of the Telerehabilitation Service
Sixty-one percent of the patients (CLBP, 57.5%; PD, 66.7%) started to use the telerehabilitation service in the first week when this service was available. Another 21% of the patients (CLBP, 22.5%; PD, 20%) started to use the telerehabilitation service in the second week when this service was available. On average the patients used the telerehabilitation service 10.8 (SD 9.5) times during the weeks of home rehabilitation: CLBP, 7.2 (SD 9.5) times; PD, 14.8 (SD 10.9) times. This is on average 1.4 (SD 1.3) times a week for CLBP and 1.8 (SD 1.4) times a week for PD. The frequency of use for the final 2 weeks for both pathologies declined compared with the first 2 weeks, and as the time proceeded the duration of use of the telerehabilitation service at first increased and then decreased in the final weeks (Table 2).
Overview of the Frequency and Duration of Use and the Percentages of Compliant Users per Week of the Exercise-Based Telerehabilitation Service
Data are mean (standard deviation) values or percentages as indicated.
CLBP, chronic lower back pain; PD, pulmonary disease.
On average the patients used the telerehabilitation service for 237.8 (SD 226.3) min during the weeks of home rehabilitation: CLBP, 178.7 (SD 226.3) min; PD, 305.1 (SD 208.1) min. This is on average 35.7 (SD 37.5) min/week for CLBP and 38.1 (SD 26.0) min/week for PD. The duration of use for both pathologies decreased over the treatment weeks (Table 2).
Compliance to the Telerehabilitation Service
For the CLBP patients the service replaced a rehabilitation day of 2 treatment-h (in total 10 treatment-h) weekly, and for the PD patients the service replaced a rehabilitation day of 2.5 treatment-h (in total, 20 treatment-h) weekly. The patients were advised by the therapist to use the service at least once a week. Table 2 shows an overview of the percentages of users per week who were compliant with home treatment, based on frequency of use. Overall, 55% of the CLBP patients and 75% of the PD patients were compliant to the advice of the therapist. Only 2 CLPB patients and 4 PD patients used the telerehabilitation service every week.
Correlation of Actual Use and Clinical Benefit
Immediately after the RP the complaints and physical functioning outcome for both patients groups significantly improved (p<0.05) (Table 3). The relationship between actual use and clinical changes during the rehabilitation period are summarized in Table 4. There is a moderate significant correlation between frequency of use and the difference between the pre- and posttest outcome in physical functioning (change in RDQ and 6MWT) for both pathologies (CLBP, r=0.41, p=0.02; PD, r=0.55, p=0.003). This indicates that the patients who use the telerehabilitation service more frequently benefit more from the intervention.
Overview of the Pre- and Posttest Outcomes on Complaints and Physical Functioning for Chronic Lower Back Pain and Pulmonary Disease Patients
Data are mean (standard deviation) values.
6MWT, 6-min walk test; CLBP, chronic lower back pain; PD, pulmonary disease; RDQ, Roland Disability Questionnaire; SD, standard deviation; VAS, visual analog scale.
Correlations Between Actual of Use and Clinical Benefit
6MWT, 6-min walk test; CLBP, chronic lower back pain; PD, pulmonary disease; RDQ, Roland Disability Questionnaire; VAS, visual analog scale.
Discussion
The aim of this article was to examine the use pattern of an exercise-based telerehabilitation service by chronic disease patients and to examine the association between actual of use and clinical benefit experienced by these patients. During the weeks of home rehabilitation the majority of the patients used the exercise-based telerehabilitation service, and 83% of all patients started to use the exercise-based telerehabilitation service in the first or second week when the service was available. However, only 6 patients used the service every week. On average the service was used one or two times a week for a total of 35–38 min for both pathologies, with this interval being lower than the time that is replaced from rehabilitation at the rehabilitation center. Given the results of this article, the conclusion of previous articles of Hermens et al., 11 Huis in ‘t Veld et al., 12 and Rho et al. 13 that patients who use the telemedicine service more frequently have a greater improvement on physical functioning can be underlined even when this telemedicine service is delivered to chronic disease patients as a partial replacement of face-to-face physical rehabilitation. Given the results of this article and these previous articles, it can be stressed that the actual use of a telemedicine service should be taken into account when studying its outcome.
Concerning the high percentage of nonusers and the decrease of duration of use over time, there are various explanations. First, it can be due to the fact that patients get used to using the telemedicine service and get familiar with the exercises. In this case patients do not need the service anymore to exercise independently in their own environment. This is of course is a positive development as it could mean that a patient is able to self-manage his or her disease and sustain his or her healthy behavior, but so far this is not known.
Second, it could be possible that the gained experience diminished, and further use does not increase the patients' functional capacity.
Third, the role of the therapist in this study was primarily focused on the rehabilitation progress. The therapists were not trained to coach the patients to use the telerehabilitation service. The only instruction given to the patients was that patients should use the service at least once a week. From experience we know that for patients it is very difficult to translate their good intention into behavior. Besides that, from behavioral science literature it is known that intentions account for less than 30% of the actual behavior, 19,20 which means that someone's behavior is mostly influenced by other factors. A solution could be that therapists help patients to formulate very specific and detailed intentions, so-called implementation intentions. 21 These intentions specify exactly when, where, and how the behavior will be performed, as well as what will be done to overcome potential barriers. Translating this to the use of a telerehabilitation service, this means that patients plan exactly on which day and time they use the service at home and how for how long they exercise.
Fourth, it might be related to a decreased motivation of the patient over time. The patient is in the first weeks motivated, but after those first weeks it becomes harder to be motivated and use the service. The aim of the exercise-based telerehabilitation service was to motivate patients to rehabilitate in their own environment and to execute their exercises at home. In a previous article only a fifth of the patients stated that the service motivated them to exercise. 6 This means that better motivational strategies in telemedicine are needed.
In conclusion, chronic disease patients do use a telerehabilitation service as partial replacement of their face-to-face RP. Most patients used the service weekly, but the duration of use was lower than the interval that was replaced. In addition, there is a significant association between the amount of use and clinical benefit. Therefore, the actual use of a telemedicine service should be taken into account when studying its outcome, and motivational strategies are needed to increase the actual use of telemedicine services.
Footnotes
Acknowledgments
Special thanks go to the rehabilitation professionals of the Roessingh Center of Rehabilitation. This work was funded by the European Union within the CLEAR project (ICT-PSP CLEAR 224985).
Disclosure Statement
No competing financial interests exist.