
Abstract
Introduction
Although comprising about 16% of the population less than 18 years of age in the United States, children with special healthcare needs (CSHCN) account for nearly 50% of all children's medical expenses. 1,2 For many of these children and their families, unique logistical and psychological barriers to access compound their heavy morbidity and financial burdens. These often include needs for special transportation, special equipment, and attendants. Especially for developmentally challenged individuals, transitions to unfamiliar environments, such as traditional healthcare settings, may induce anxiety, fear, and disruptive behavior. These circumstances challenge the healthcare community to reduce the morbidity, financial, logistical, and psychological burdens borne by CSHCN, their families, and their communities.
Health-e-Access is a telemedicine model that initially focused on care of children in regular childcare and schools (CRS) in Rochester, NY, with acute illness. Effectiveness, efficiency, and acceptability to parents and providers for CRS in these settings have been established based on studies involving over 14,000 telemedicine visits since May 2011. Among children attending inner-city childcare centers with telemedicine availability, absence due to illness dropped by 63%. 3 Among telemedicine visits initiated at elementary school and childcare sites, 97% of telemedicine visits have been completed (i.e., diagnosis and management decisions were made, and treatment was implemented), based solely on Health-e-Access. 4 Only 3% of these visits led to referrals to higher-level care. 4 Acceptance of Health-e-Access by parents, providers, and insurance organizations was confirmed by high levels of parent satisfaction, 5 participation in Health-e-Access by over 70 different providers from 10 primary care practices, 4 telemedicine access in all Rochester City Schools, and reimbursement at office visit rates for telemedicine visits by all local payers, including Medicaid Managed Care. For visits by children with a participating primary care practice, continuity of care within the medical home averaged 83%. 4 Children with telemedicine access from childcare or elementary school made 22% fewer emergency department (ED) visits than closely matched counterparts. 6 Based on parent estimates, an ED visit on average takes 4.5 h of parents' time, 3 whereas most childcare- and school-based telemedicine visits enable parents to remain at work.
Based on success among CRS, we proposed to extend Health-e-Access to children attending a school for CSHCN. Yet, providers questioned the safety and effectiveness of Health-e-Access among CSHCN, citing less resilience. This study assessed the hypothesis that effectiveness and safety of Health-e-Access for care of CSHCN with acute illness equaled those for CRS.
Materials and Methods
Health-e-Access use by CSHCN and CRS was compared in an observational study before and after multiyear periods when options for access were enhanced through availability of telemedicine (Fig. 1).
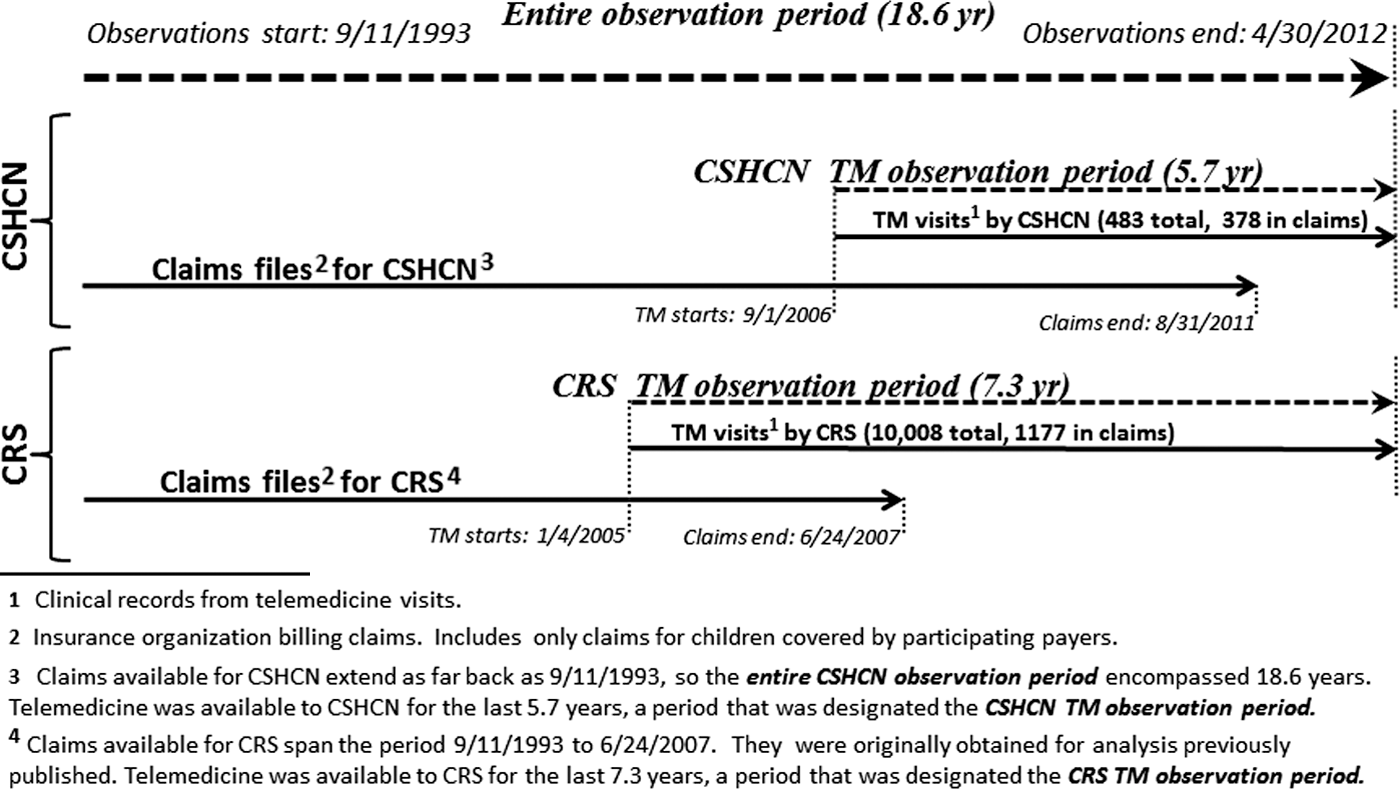
Observation periods and sources. CRS, children attending regular school or childcare; CSHCN, children with special healthcare needs; TM, telemedicine.
Understanding the objectives and design of Health-e-Access is essential to evaluating its effectiveness. The Health-e-Access mission was to “enable healthcare when and where you need it, by providers you know and trust.” Consistent with this mission, Health-e-Access initially focused on care of acute childhood illness in regular childcare and elementary schools. Care was always provided with parental consent, generally by a provider from the child's primary care medical home. Health-e-Access relied on real-time and store-and-forward interactions and on commercially available telemedicine units. 7,8
After a problem was identified by parents or by child site staff, personnel on-site collected information, following templates built into the telemedicine software, about the present illness and past medical history. These on-site telemedicine assistants completed templates and acquired still images, video clips, and audio files. Digitized input was acquired from an electronic stethoscope and an all-purpose digital camera that captured ear canal, tympanic membrane, nose, throat, eye, and skin images. Information was saved to a secure, central server. This information was then accessible via secure Internet connection to providers at a distant location. Store-and-forward material was supplemented as required by the clinician, both with real-time videoconferencing and with additional history obtained through the provider's videoconference interaction or phone conversations with telemedicine assistants, childcare or school staff, or parents.
Interactions between provider and parent and between provider and child site generally occurred within 1 h of the time that concerns were brought to the attention of Health-e-Access staff. Clinicians faxed prescriptions to a pharmacy that delivered, in many instances, to the child site. Further details of operations are provided elsewhere. 8
Study Populations
Observations among CRS began with the launching of Health-e-Access in a single, inner-city Rochester childcare center in May 2001. By September 2011, in addition to six city childcare sites, Health-e-Access was available in all schools of the Rochester City School District.
Health-e-Access became available at a school for CSHCN in September 2006. This site is located in Rochester but serves about 550 children dwelling in both Rochester and 10 counties and 50 surrounding school districts. All children served had intellectual disability plus other disabilities, most commonly including autism, cerebral palsy, degenerative conditions, seizure disorders, and emotional problems. In addition to preschool (ages 3–5 years) and school-age (age 5–21 years) programs, a program for school-age children with profound special needs averaged 70 enrollees. All in this latter program had a combination of severe physical, cognitive, and medical needs. Most were medically fragile and wheelchair bound. Many received tube feedings. On-site nursing staff employed by the Development Center served as telemedicine assistants for CSHCN.
De-identified insurance organization billing claims (claims files) and telemedicine clinical records were used (Fig. 1) to compare visits for CSHCN and CRS. Insurance organizations provided claims on children registered for Health-e-Access and whose parents consented for use of these data. Claims data, which extended as far back as September 11, 1993 for some participating children, were not available for those without a collaborating payer.
Among CSHCN, claims data were available for 300 children attending the Development Center at any time during the CSHCN Telemedicine Observation Period of 5.7 years. Claims data were available also for 1,950 children attending regular schools or childcare sites at any time during the CRS Telemedicine Observation Period of 7.3 years.
Measures
Health-e-Access effectiveness was assessed as rates of visit completion, visit duplication, and adverse events. Completion of visits was defined as a visit with diagnosis and management decisions made, and treatment implemented, based solely on the Health-e-Access model (i.e., there was no in-person physical examination, imaging, or laboratory testing beyond what was available at telemedicine access sites). Completion was assessed through examination of telemedicine visit records during the Telemedicine Observation Periods.
Noncompleted visits were examined by two of the authors (K.M.M. and S.D.R.) in detail through clinical records because of the possibility that they might constitute “sentinel events,” pointing to opportunities to improve system performance. Telemedicine visit records are uniquely suited for detailed clinical review because they provided original material (e.g., images, video clips, lung sounds) in addition to standard text documentation.
Lack of effectiveness was inferred if duplication of services provided in a Health-e-Access visit occurred within a short period of time. Duplication within 1 day was used as a narrow definition, and duplication within 3 days was adopted as the broad definition of this construct. We also evaluated duplication by assessing the likelihood that the problem addressed in the second visit was related to the problem addressed at the initial visit. For example, if the primary diagnosis for the index telemedicine visit was acute otitis media and the primary diagnosis for a next-day visit was autism, the second visit was not counted as a duplicate visit. If the primary diagnosis for the next-day visit were again acute otitis media, however, the second visit would be counted as a duplication of services. Likelihood was based on agreement of two clinician-investigators (KM.M. and S.D.R.).
Adverse events were indexed by the occurrence of an ED visit following the Health-e-Access visit within 3 days when the ED visit's primary diagnosis was at least probably related to that of the Health-e-Access index visit. Duplication of Health-e-Access services with ED services was considered a measure of effectiveness as well as a measure of safety, consistent with the view that a service is effective only if it is safe.
All telemedicine visit records were examined to determine completion rates, including the 483 CSHCN telemedicine visits and the 10,008 CRS telemedicine visits. Duplication and adverse events were ascertained from claims files that captured 378 and 1,177 of these visits, respectively.
Results
Health Services Utilization
As shown in Figure 2, CSHCN claims file extending through August 31, 2011 included 20,722 claims, with 13,770 occurring during the CSHCN Telemedicine Observation Period. CSHCN claims encompassed 15,161 child-months of observation and included variable periods of enrollment for the 300 children included in this group. Of the 483 telemedicine visits that occurred during the CSHCN Telemedicine Observation Period, 378 (78.3%) were captured in claims.

Observations among children with special healthcare needs (CSHCN) and children attending regular school or childcare (CRS). ED, emergency department.
The CRS claims file extending through June 24, 2007 included 56,798 claims, with 21,107 occurring during the CRS Telemedicine Observation Period. CRS claims encompassed 19,652 child-months of observation, similarly reflecting variable periods of enrollment for 1,950 children. In total, 10,008 telemedicine visits occurred during the CRS Telemedicine Observation Period. Among them, 1,177 (11.8%) were captured in claims. The proportion of telemedicine visits by CRS captured in claims is smaller than for CSHCN (11.8% versus 78.3%) largely because the proportion of respective telemedicine observation periods for which claims were available was smaller for CRS than CSHCN (33.7% versus 88.2%). The difference in proportion of telemedicine visits captured by claims is, to a lesser extent, also attributable to the fact that a larger proportion of CRS than CSHCN was covered by insurance that did not provide claims.
Completion
Among the 483 CSHCN telemedicine visits, 9 were not completed, yielding a completion rate of 98.1% (95% confidence interval, 97.5–98.7%). Among the 10,008 CRS telemedicine visits, 240 were not completed, yielding a completion rate of 97.6% (95% confidence interval, 97.4–97.8%).
Duplication
Among the 483 telemedicine visits by CSHCN, 378 were made by children whose claims files were available, thus allowing assessment of duplication. Use of one or more health services followed 20 (5.3%) telemedicine visits within 1 day and 61 (16.1%) within 3 days. As detailed in Figure 2, these 61 telemedicine index visits were followed by a total of 72 visits within 3 days. These 72 subsequent visits included visits to the ED (0.5%), telemedicine again (3.7%), or office (14.8%). A substantial proportion of subsequent visits was clearly not related to the telemedicine visit (43.1%). Among all 378 telemedicine visits, the proportions followed by visits classified as at least possibly and at least probably related were 10.6% and 7.1%, respectively (Fig. 2). Table 1 lists all diagnoses at subsequent visits.
Visits Among Children with Special Healthcare Needs Following 61 Telemedicine Index Visits Within 3 Days
In total, 72 visits followed the 61 index visits within 3 days. Among these 72, 31 were clearly for problems not related to the index visit.
Percentage of the 378 telemedicine index visits captured in insurance claims.
Percentage of the 72 visits following the 61 index visits within 3 days.
NOS, not otherwise specified.
Among the 10,008 telemedicine visits by CRS, 1,177 were made by children whose claims files were available, thus allowing assessment of duplication. Use of one or more health services followed 104 (8.8%) telemedicine visits within 1 day and 186 (15.8%) within 3 days. As detailed in Figure 2, these 186 telemedicine index visits were followed by a total of 190 visits within 3 days. The 190 subsequent visits included visits to the ED (0.5%), telemedicine again (3.7%), or office (14.8%). A substantial proportion of subsequent visits was clearly not related to the telemedicine visit (45.3%). Among all 1,177 telemedicine visits, the proportions followed by visits classified as at least possibly and at least probably related were 8.8% and 6.5%, respectively.
Adverse Events
Following the 378 CSHCN telemedicine visits, two ED visits occurred. For the preceding telemedicine visits, the primary diagnoses were upper respiratory illness and tinea corporis, respectively. Primary problems addressed at the subsequent ED visits were upper respiratory tract illness and cerebral palsy (Table 1). The ED visit for an upper respiratory tract illness met the definition of an adverse event (0.26% of all CSHCN telemedicine visits).
Following CRS telemedicine visits, 21 ED visits occurred within 3 days. Six of these visits (0.51% of all 1,177 CRS telemedicine visits) were assigned a primary diagnosis that was at least probably related to the primary diagnosis for the telemedicine visit, thus meeting the definition of an adverse event. Nine more of these visits were assigned a primary diagnosis that was possibly related to the primary diagnosis for the telemedicine visit, so that, in total, 15 subsequent visits (1.3% of all CRS telemedicine visits) were followed by a visit that was at least possibly related to the primary diagnosis for the telemedicine visit. Diagnoses for the 14 telemedicine visits among CRS and the 15 subsequent ED visits that were at least possibly related are listed in Table 2.
Telemedicine Visits and Emergency Department Visits Following Within 3 Days Among Children in Regular Schools or Childcare: Ascertainment of Adverse Events
The telemedicine visit was the first visit in each cluster, by definition. For cluster #7, two emergency department (ED) visits followed the telemedicine visit within 3 days.
An adverse event. An adverse event was defined as an ED visit following a telemedicine visit within 3 days and having a diagnosis that was at least probably related to that of the index visit.
NOS, not otherwise specified.
Discussion
Prior research has supported the use of telemedicine in addressing ongoing care needs of CSHCN in rural communities, 9 –11 but no reports of acute illness care via telemedicine among either rural or urban CSCHN have been published. Findings reported herein support the safety and effectiveness of the Health-e-Access care model, as implemented for both CSHCN and CRS. Examination of reasons for failure to complete CSHCN visits (Table 3) suggests that noncompletion might occur even less frequently if parents and providers were more familiar with this care model. Detailed review of the nine noncompleted CSHCN visits (Table 3) suggested that two (cases 2 and 9) were beyond the scope of Health-e-Access, although completion of both might have been possible if arrangements had been made for collection of laboratory specimens that were not part of the usual Health-e-Access model. For three more visits, failure to complete appeared to be because of provider uncertainty (cases 3, 4, and 8), a barrier that might be overcome by a primary care provider who is both familiar with telemedicine and has an ongoing relationship with the family. In two instances, it is plausible that completion would have occurred if the parent were more familiar and confident with telemedicine (cases 1 and 5). Greater skill in cerumen removal or communication with the child might have enabled completion in case 7. Failure of completion in case 6 was attributable to a failure of the technology.
Reasons for Failure to Complete Telemedicine Visits Among Children with Special Healthcare Needs
The completion rate of 98.1% for CSHCN was similar to that observed for CRS (97.6%). This was accomplished despite more underlying chronic problems, less physiological resilience, and greater challenges in eliciting cooperation with examinations among CSHCN.
Effectiveness was also supported by the large proportion of Health-e-Access index visits not followed within 3 days by visits even possibly related: 89.4% for CSHCN and 91.2% for CRS (Fig. 2).
Subsequent visits within 3 days that were at least possibly related (10.6% for CSHCN and 8.8% for CRS) may have occurred for various reasons. The course of common illness episodes often includes worrisome manifestations. Close follow-up is rightly considered an important attribute of quality. Follow-up in-person or via telemedicine may be the only way to resolve diagnostic uncertainty, as with an acute illness in which diagnostic attributes, such as characteristic skin lesions, only appear later in the course of an illness. Follow-up examination may be important to confirm that treatment is being effective, as with cellulitis. Subsequent visits may be valuable regardless of how the initial visit was accomplished.
The occurrence of subsequent visits within 3 days might also reflect lack of confidence in diagnosis or in treatment recommendations at the index visit, either on the part of the parent or on the part of an office nurse managing a follow-up phone call from a concerned parent. In situations where the subsequent visit only provides reassurance that the initial visit might have provided in most instances, it seems appropriate to consider the subsequent visit as duplicative. Information provided in Tables 1 and 2 is consistent with the view that a substantial proportion of subsequent visits within 3 days might have been avoided with more effective counseling at the initial visit, but they might also have provided reassurance that the family considered important. Regardless, duplicative service appeared no more common among CSHCN than among CRS.
Finally, adverse events were uncommon among both CHSCN and CRS, and the adversity was limited to financial and psychological effects; physiologic deterioration did not occur. We have previously demonstrated that Health-e-Access has an important impact on utilization of the ED for nonemergency problems for both CRS 6 and CSHCN. 12 Because payment within fee-for-service financing systems is much greater for ED visits than for Health-e-Access or office visits, 13 replacement of an ED visit with a Health-e-Access visit has significant financial consequences.
Limitations
The process of selecting children for Health-e-Access visits must be considered when interpreting findings. For both CSHCN and CRS, decisions to use Health-e-Access involved decisions by both parents and child site staff. Given substantial biological differences in the children and differences in structure of child sites, between-group comparability (CSHCN versus CRS) of illness episodes selected for Health-e-Access cannot be assured despite large numbers of observations extending over multiple years and despite similarities in distributions of age and sex. Illness episodes among CSHCN selected for Health-e-Access might have been less severe than those selected among CRS; parent and site staff for CSHCN may have been more risk-averse. Although this may be considered a limitation of this study, the fact that observations were heavily influenced by behavior of parents and staff also suggests that results are likely to represent the impact of this care model in the “real world” where such selection does, in fact, occur. This research was not conducted under circumstances controlled by investigators.
Effectiveness and safety are both broad constructs. Several dimensions of effectiveness, and observations reflecting them, were not considered in the analysis presented. Analysis related to impact on utilization patterns, healthcare costs, acceptance by providers, and satisfaction of families is in progress. The most important dimension of effectiveness depends on one's perspective. In the eyes of many parents and providers, convenience is the dimension that dominates effectiveness for problems that are mostly minor and self-limited. Given that the vast majority of Health-e-Access visits were completed and are more convenient than both office and ED alternatives, high completion rates strongly support effectiveness. Arguably, impact on safety, addressed herein, should be addressed first.
Conclusions
Observations indicate that safety of the Health-e-Access telemedicine model is comparable for CSHCN and CRS and sufficiently effective to be valuable for both groups.
Footnotes
Acknowledgments
The authors gratefully acknowledge the collaboration and trust of staff of the Mary Cariola Children's Center, of the schools in the Rochester City School District, and of the several participating childcare centers in Rochester, NY, and of the parents whose children were served. The different observation phases involved in this analysis were supported by several grants, as follows: Agency for Healthcare Research and Quality (R18 HS018912, R01 HS016871, and R01 HS15165); New York State Healthcare Foundation (Optimizing Access to Avoid Emergency Department Use for Non-Emergency Problems); New York State Health Department (Telemedicine to Optimize Access to Primary Care); Health Resources and Services Administration, Maternal and Child Health Bureau (R40 MC03605); the Robert Wood Johnson Foundation (RWJF Local Initiative Funding Partners); and the U.S. Department of Commerce Technology Opportunities Program (Telemedicine in Daycare). Robert Wood Johnson Foundation funds were matched by funds from several anonymous donors and from 11 Rochester-area foundations, including the Rochester Area Community Foundation, Daisy Marquis Jones Foundation, United Way of Rochester and Monroe County, Halcyon Hill Foundation, Rochester's Child, Gannett Foundation, Marie C. and Joseph C. Wilson Foundation, Fred and Floy Wilmott Foundation, Weyerhaeuser Company Foundation, Feinbloom Family Supporting Foundation, and Frontier Telecommunications Corporation.
Disclosure Statement
K.M.M. and N.E.W. both held a significant financial interest in TeleAtrics, Inc., which owned the Internet-based telemedicine application that was used in providing the service described herein. TeleAtrics was acquired by Trifecta Technologies in August 2008. These individuals were cofounders of TeleAtrics and, as a result of the sale, accrued a percentage of potential revenues through July 2013. Neither TeleAtrics nor Trifecta provided any funds for support of Health-e-Access or for the research described herein. S.D.R. and P.K.N. declare no competing financial interests exist.