
Abstract
Introduction
Chronic diseases such as hypertension are now routinely managed with telemedicine. 1 Availability of inexpensive home blood pressure (BP) monitors and a range of options to transmit the BP readings have enabled several different telemedicine approaches to BP management. Fax, telephone, mobile text messages, and e-mail have all been used with home BP monitors to achieve BP control without office visits. 2 –4 Using real-time BP telemonitoring and telephonic monitoring, Wakefield et al. 5,6 were able to successfully manage BP and educate patients without office visits. A free-standing Web portal sponsored by the American Heart Association (AHA) has been used to collect and store home BP readings that pharmacists could access and use to manage BP. 7 Virtual visits are also now being used for hypertension management. 8 Sending BP information by secure message over a patient portal is another telemedicine method used to manage BP but has not been well studied. Because there are 39 million office visits for hypertension in the United States yearly 9 and an increasing number of patients have access to a patient portal, it is important to examine whether portal secure messages could substitute for hypertension office visits.
Patient portals vary in their functionality but usually include the ability to view parts of the medical record and are able to perform some administrative tasks such as medication refill and appointment requests. Increasingly, patient portals have additional secure message capability, which allows patients to directly send messages to their healthcare teams. 10,11 Secure messages are often used to communicate with healthcare teams about medication questions and new symptoms, 12 but secure messages can also be used to transmit data collected from home monitoring devices. However, patient portals have not been optimized to manage home-monitored clinical parameters.
In order to explore potential deficiencies in the management of hypertension through a patient portal, we examined patient-generated secure messages containing self-monitored BP content and studied how their providers responded to these messages.
Materials and Methods
This was a retrospective analysis of all patient-generated secure messages from Mayo Clinic Patient Online Services (the patient portal) sent to Mayo Clinic Rochester (Rochester, MN). The study was approved by the Mayo Clinic Institutional Review Board.
Setting
Mayo Clinic Rochester is a tertiary-care medical center. At the time of the study, there were 1.5 million outpatient visits, 300,000 of which were in primary care. Thirty percent of active patients were registered for portal access.
Secure messages during the study period had a structure similar to an e-mail: patients could initiate an interaction and enter text in a subject line and message body. No fee was charged for sending a secure message or for the provider response.
All Mayo Clinic Rochester providers are salaried, and there was no financial or other direct incentive for providers to respond to secure messages or to increase secure message volume.
Identification of BP Telemonitoring Messages
We screened all patient-generated secure messages directed to the Mayo Clinic Rochester patient portal for the calendar year 2012. Text string searches for “BP” and “pressure” identified a subgroup of messages that we individually read. We retained only those messages containing information about patient-monitored BP and matched it with the provider response. We randomly selected approximately one-third of the message–response pairs.
Reference Standard
We used the AHA and American Society for Hypertension (ASH) guidelines to assess whether BP data in the messages met standards for making therapeutic decisions. 13,14 This standard recommends collecting BP values at rest over a 7-day measurement period with an average of at least 12 measurements (both morning and evening).
Demographics and Comorbidities
Age, race, sex, and other demographics were obtained from Mayo Clinic registration data. We used ICD-9 diagnosis billing code data to capture the diagnosis of hypertension for visits from 2007 through 2012. We used the Charlson Comorbidity Index to compare the overall health of the senders. 15,16 Other information about education and smoking status was retrieved from the Mayo electronic medical record.
Content Abstraction
From the 212 messages sampled, we captured categorical information on how the BP data were presented. Patients gave qualitative information (“my blood pressure readings are too high”), quantitative information (“my blood pressure was 150/90”), or both. For those messages with quantitative data we counted the number of BP readings and how patients presented them. We categorized the quantitative data into individual readings (“my blood pressure readings were 120/80 and 134/86”), stated BP averages (“my average blood pressure was 140/90”), implied averages (“my blood pressure was about 140/90”), and blood BP range (“my blood pressure ranged from 140 to 150 over 80 to 90”). We also looked for evidence that the BP information contained in the message met the criteria of the AHA/ASH standard for adequate home BP readings. We also categorized the purpose of the messages. Some patient messages delivered ongoing follow-up of BP readings, some had concern about the level of the readings, and some sent BP information only as a vital sign in the context of a symptom unrelated to BP management. We also looked for any evidence that the patient had reconciled medications with the medication record visible on the patient portal (the electronic medical record medication list). For each message, two physicians used a 7-point Likert scale to independently assess the comfort level of the physician reviewer in writing a new prescription based solely on the BP content of the message. We also obtained the highest systolic and diastolic BP values contained in the messages.
Provider Responses
We examined provider message responses for new antihypertensive prescriptions and medication dosage adjustment. We also looked for additional communications from the provider, including whether more information was desired. For the patients who had a new medication recommended, we examined the medical record to determine if there had been documented telephone calls or other communication to fill message information gaps.
Message Review Process
Two physician authors (F.N. and M.E.) independently reviewed all of the randomly selected message–response pairs and used a REDCap database to collect the abstracted information. 17 We then compared our results and came to a consensus by arbitration for our final dataset. One physician performed a chart review looking at additional work from messages associated with a new prescription.
Statistical Methods
We used the two-sample difference in proportions test to determine differences in proportions between groups. We used the Cochran–Armitage test for trend for monthly changes in proportion of message use for BP. JMP version 10.0 software (SAS Institute, Cary, NC) provided the statistical calculations and randomly selected the 212 messages for review.
Results
We identified 55,459 patient-generated messages from 20,594 patients. We excluded 3,086 messages from 1,049 patients without research authorization, leaving 52,373 messages from 19,545 patients remaining. Twenty-three percent (4,412) of the patients had a billing diagnosis of hypertension. There were 1,461 messages that had either “BP” or “pressure” in the message body. After individual review of all 1,461 messages, we identified 624 secure messages that had evidence of monitored BP values. These 624 messages were generated from 365 distinct patients.
There were 617 responses to the 624 messages, for a response rate of 99%. There were 148 distinct individuals responding to the messages, of which 80 (55%) were physicians, 46 (31%) were nurses, and 10 (7%) were physicians assistants or nurse practitioners.
Four provider groups received almost all the 624 messages: Primary Care Internal Medicine received 39% (n=245), Family Medicine 21% (n=134), Nephrology 16% (n=98), and Transplant Care 20% (n=124). Pediatrics received only five messages regarding BP.
Physicians directly responded to 88% of the messages (215 of 245) in Primary Care Internal Medicine and to 73% of Family Medicine responses (98 of 134). Over 90% of the physician staff in Primary Care Internal Medicine directly responded to at least one secure message about BP (40 of 44 staff physicians). Ten nurses (RNs) responded to 99% of the 98 messages to Nephrology. Eleven nurses (RNs) in Transplant Care responded to 100% of the 124 messages. No physicians, nurse practitioners, or physician assistants in Nephrology or Transplant Care directly responded to patient messages.
Message counts over time approximated a linear increase (Fig. 1), with the counts per month nearly doubling in the course of a year. The total volume of secure messages also showed a similar increase over the same year, and the proportion of BP secure messages to total patient messages stayed fairly constant at about 1.2% (Fig. 1) (Cochran–Armitage test for trend, p=0.45).
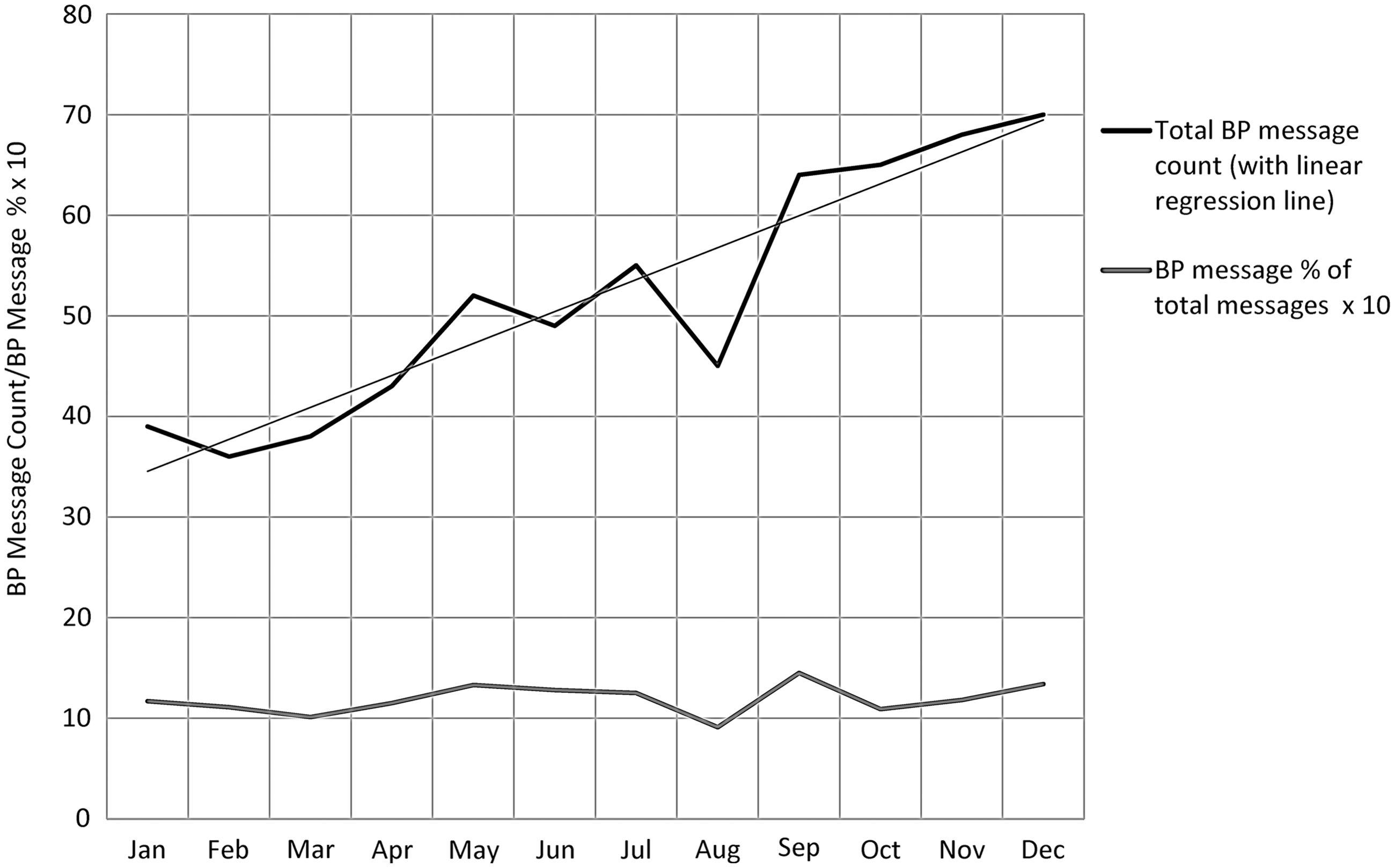
Blood pressure (BP) secure message counts by month and percentage of total.
Demographic Comparison
Table 1 compares the demographics of the 365 patients who sent BP messages with those of other patients sending messages.
Baseline Comparison Between Blood Pressure Message Senders and Other Message Users
Data are percentage (n).
Based on the hypothesis that proportions are equal.
CI, confidence interval.
Message Content
For the 624 messages, there was a median of two BP readings per message (range, 0–98). Messages concerned a BP follow-up or ongoing BP monitoring in 53% (95% confidence interval, 42%, 56%]. In 18% (95% confidence interval, 13%, 23%) BP was mentioned in conjunction with a symptom and was not the main topic of the message.
Table 2 shows a breakdown of the patient message content. Messages typically contained more than just BP data.
Patient Message Content (n=212)
AHA, American Heart Association; ASH, American Society for Hypertension; BP, blood pressure; CI, confidence interval.
Assuming an intent to write a new prescription based only on the BP data quality in the message (not the actual BP level), the reviewing physicians were only moderately or extremely confident in doing so in 12% (95% confidence interval, 8%, 17%).
Provider Response
Table 3 contains the results of the provider response review. Additional chart review of the patients who had a new prescription revealed that 53% (8 of 15) had evidence of additional contact with the patient to resolve any lack of information noted in the patient message. For those messages that the reviewer consensus judged needed action for BP greater than 135/85 mm Hg (20%), 44% had a message response containing a prescription or dose change, and 42% had responses that requested more BP data.
Provider Responses (n=212)
BP, blood pressure; CI, confidence interval.
Safety
From a safety perspective, there were some high BP values reported. In 11% (n=19) there was at least one systolic measurement over 180 mm Hg or diastolic over 105 mm Hg. Median provider response time was 17.6 h, and we found no emergency department visits within 30 days of the messages. This is consistent with our previous finding that secure messages in general are low risk. 12
Discussion
Patients are sending secure messages with BP information, and this information is being used for antihypertensive drug management. We found several deficiencies with secure messages for BP management, including limited BP data and insufficient information to prescribe antihypertensive medication. Some patients gave only a qualitative BP interpretation, whereas others gave multiple individual readings over multiple days, including dates, times, and conditions under which the BP was taken. Using AHA/ASH recommendations, only 7% of the messages contained sufficient home BP information for clinical decision-making.
Lack of pharmacy information was a barrier to BP medication management and resulted in extra work to make medication changes. From the 212 message sample, 15 messages were associated with a new prescription, with 53% (n=8) requiring pharmacy information, generating a total of 11 additional notes in the record. In 98% of patient messages about BP there was no evidence patients had checked their portal drug list for discrepancies.
Patient concerns about high and low BP accounted for over one-third of the messages. There were concerns about BP medication side effect in about 10%, and dosage changes were mentioned in 13% of the patient messages. In essence, about 50% of the messages involved BP medication management. Despite the medical concerns voiced by patients in their secure messages, there was little evidence that patients were using messages to gain face-to-face access. We only found a patient request for an appointment in 3% of the messages, and providers suggested an appointment in only 11% of the message responses. These findings suggest that BP information transmitted asynchronously via the portal was acceptable both for patients and providers as a means for BP management without a face-to-face visit.
Although the messages had deficiencies that hampered BP management, there were few other barriers to its use. For providers, patient-generated secure messages were already a part of normal daily workflow so no new training was required. Patients likewise already knew how to send secure messages, and there was the potential to avoid the cost and inconvenience of an office visit. From the institutional perspective, secure messages about BP were a part of normal portal traffic—no new infrastructure was required to support them. Lack of barriers for the institution and no cost for the patient likely explains some of the steady growth of messaging that we observed (Fig. 1).
There is likely to be continued uptake of portal telemonitoring from patients. Patients can access the patient portal from their mobile smartphones, 87% of patients have Internet, 18 and 45% of patients with hypertension are already monitoring their BP at home. 19 Healthcare institutions can also easily accommodate secure messages because the infrastructure for secure messages is already in place.
The BP secure messages were compatible with different care processes. For example, in primary care, the workflow of these messages mainly involved physicians; in transplant and nephrology, nurses were the responders. In our review, pharmacists had not been integrated into the care process for answering these messages, but we found nothing in the message content to exclude pharmacist participation. Pharmacists are likely to play a future role in responding to messages about BP as they have with other BP management care processes. 7,20
Secure messages for BP management need to be examined in the context of an overall telemedicine strategy for BP management. We know that real-time BP telemonitoring can successfully be used for BP management, 5,6 but at $500 for 12 months it can be quite expensive. 20 Although virtual visits (e-visits) are being used for BP management, 8 they have not been well studied, and we do not know the best type of information management needed for these types of asynchronous visits. Secure messages may fit into a niche alongside dedicated telemonitoring (with hubs and servers) and e-visits. Patients with adequate control of their BP and no concerns about their antihypertensive medication could use a secure message to confirm adequate BP control without requiring an office visit. Patients needing frequent BP measurements or titration of antihypertensive medications would need more robust data-capturing support from dedicated telemonitoring systems or e-visits.
We found secure messages generally lacked sufficient information for providers to prescribe an antihypertensive medication. However, patient-generated secure messages about BP do yield important information. Patients who are sending BP information by secure message have the equipment and motivation necessary for BP management online and thus would be good candidates for tailored BP e-visits. The information gaps we found in secure messages could be resolved with e-visits using specific information-gathering forms. BP readings, medication reconciliation, and pharmacy information could all be built into portal forms that would support a BP management e-visit. Designers of BP e-visits could use the findings from this study to examine best ways of addressing those information gaps. For example, some patients appear comfortable transmitting BP averages, whereas others use individual readings (Table 2). Input forms for BP e-visits might need to take those data input preferences into account.
Secure messages occur in a context that may mitigate some of the shortcomings we found. Patients sending secure messages could have a history of providing reliable home BP readings to their provider that was verified during multiple previous face-to-face visits. Under such circumstances providers might be quite comfortable making decisions on home BP readings not conforming to AHA/ASH standards. Likewise, providers might be comfortable that patients were taking medications as listed in their electronic medical record and that confirmation of medication reconciliation was not essential.
This study had limitations. We did not measure the effort required by the provider to respond to these secure messages and did not determine whether the secure messages actually decreased office visits. We do know that studies on BP telemonitoring and secure messages have not consistently demonstrated that office visits decrease after introducing these technologies. 21,22 Additional limitations are that our patient population using the portal for telemonitoring BP was highly educated and racially homogeneous, so our findings may not generalize to a wider audience of portal users. Our providers are also not compensated on a fee-for-service basis. Secure messages for BP are likely to get a different response from providers who have income generated by BP office visits. Regional quality measures also may present a barrier to the implementation of BP telemonitoring. 23
Patients are using secure messages to engage their providers in BP management. These secure messages often lack data that providers need for well-informed decisions about BP management. Providers ask for additional information to fill in these data gaps, but that requires extra messages and telephone calls and results in an inefficient process of BP management. Ongoing BP management should additionally be supported by care processes with dedicated BP telemonitoring systems or by tailored BP e-visits that are able to deliver the structured data necessary for more efficient BP management.
Footnotes
Acknowledgments
The authors thank Eric Manley, Barbie Mundt, and Stephen Cha for their contributions to this manuscript.
Disclosure Statement
No competing financial interests exist.