
Abstract
Background
Chronic disease imparts significant health and care costs to the patient and health system, with previous estimates suggesting the cost to be as much as 75% of U.S. healthcare expenditures. 1 Chronic obstructive pulmonary disease (COPD) and heart disease independently contribute substantially to the overall burden of chronic disease in the United States and are leading causes of hospitalization, re-admission, and death. 2 –5
Demographic characteristics such as socioeconomic status affect chronic disease severity and functional health, 6 which includes the ability to access and/or pay for healthcare services. A recent study reported that underserved patients with diabetes showed patterns of worse health, increased emergency department (ED) use, and increased inpatient stays compared with the general population. 7 With rising healthcare costs and an aging U.S. population, there is an ever-increasing need to determine effective ways to transition these complex chronic disease patients from the hospital back to the home setting in ways that reduce their risk for relapse and re-admission. 8
Telemonitoring has shown promise in reducing acute care utilization for patients with chronic disease. In a recent Cochrane review, 9 the authors concluded telemonitoring for COPD patients impacts quality of life and acute care utilization, although the evidence was relatively weak. Another recent meta-analysis showed telemonitoring reduces death and hospitalizations for heart failure (HF) patients. 10 These telemonitoring interventions were primarily for long-term interventions (3–12 months) implemented in the primary care setting. Furthermore, none of the studies was conducted in underserved populations. 8 Little is known about the potential benefit of telemonitoring in relation to a short-term, transitional care intervention designed to benefit vulnerable populations such as underserved chronic disease patients. Therefore, the purpose of this pilot study was to determine feasibility of a transitional care program that integrated mobile health technology and home visits for underserved COPD and HF patients and evaluate preliminary program outcomes related to acute care utilization.
Materials and Methods
The intervention was a prospective 90-day transitional care program following an acute event that integrated mobile health technology and home visits for underserved COPD and HF patients. The program was structured in part based on the transitional care model of Coleman et al. 11 and Sharp HealthCare's Transitions model for chronic disease patients 12 and incorporated a remote monitoring device. The program coordinator (PC) was a Masters-prepared registered nurse, responsible for patient enrollment, education, coaching, care coordination throughout program, and disenrollment at program end. A retrospective cohort design was used to compare outcomes for patients enrolled in the program with a propensity-matched, nontreated cohort identified through the health system's electronic health record.
Setting
Sharp HealthCare is a not-for-profit integrated regional healthcare delivery system based in San Diego, CA. Two Sharp hospitals were the setting for the study, both with a high proportion of uninsured or underinsured patients and a higher percentage of Medi-Cal and Medicare patients compared with all San Diego County hospitals.
Participants and Recruiting
Patients were enrolled into the program in the hospital setting during an acute chronic disease exacerbation. The enrollment time frame was from October 2010 to August 2012 with inclusion criteria of (a) a primary diagnosis of COPD or HF, (b) underserved, (c) English or Spanish speaking, (d) U.S. residence, and (e) independent in their own care or with reliable caregiver. Underserved status was defined through patient insurance type: no insurance (unfunded, self-pay); Medi-Cal (a California medical assistance program serving low-income families, seniors, and persons with disabilities); County Medical Services (a San Diego County program that funds medical care for indigent adults); or unassigned Medicare fee-for-service. Patients were excluded from enrollment if they had end-stage COPD or HF, were a hospice candidate, had an active cancer or pulmonary fibrosis diagnosis, were on dialysis, spoke a language other than English or Spanish, or were discharged to a setting other than home.
The PC initially identified patients as potential participants through daily review of the hospital census. Potential enrollees were approached if they met initial criteria; the program was described, and enrollment was offered. If the patient agreed, consent for participation was obtained, which included permission to visit patients in their home, to call them as needed, and to send them the remote monitoring device (RMD).
Program Description
Enrollees were provided a folder with program information, contact information, and preprinted education materials about symptom management provided free of charge from Boehringer-Ingelheim (
The initial home visit occurred approximately 1 week after discharge. The PC assisted with RMD set-up and patient education on use. The home visit also included medication reconciliation, self-administration of the functional status questionnaires, and education regarding medication use, symptom awareness and management, nutrition, and stress management. A personal patient health plan was developed, and the PC confirmed or coached patients to set up physician follow-up appointments.
Additional home visits were triggered by request or by review of symptomatology by the PC. Patients could call the PC or the RMD monitoring staff at any time with health concerns or questions about their personal disease management plan. The PC contacted patients as they approached the program end date (90 days from enrollment) for a final home visit. During the final visit, the PC and the patient reviewed the personal health plan, and the functional status questionnaires were re-administered along with a telemonitoring satisfaction survey. The device was packed up at that time and returned by mail.
RMD and Activities
Cardiocom (
Outcomes
Primary outcomes were acute care utilization, defined as use of an ED for any reason, and all-cause re-admission or observation stay in an acute care hospital. Outcomes were quantified at 30 days, 90 days, and 180 days after program enrollment. Patient identifiers were used to query the organization's electronic health record for all documented acute care visits. Satisfaction with the program was measured with the Centura Telehealth Patient Satisfaction Survey. 13 Program participants' health status was measured at enrollment and discharge from the program using validated functional status instruments. COPD patients self-administered the Clinical COPD Questionnaire. 14,15 HF patients self-administered the Self-Care of Heart Failure Index (SCHFI). 16
Statistical Analysis
Due to resource restrictions, randomization into program and control groups was not possible. However, a control cohort was obtained using an innovative integration of sampling and statistical methods to gain an efficient comparison. First, a preliminary control cohort was identified in the electronic medical record with the same hospital setting, admission type and date range, primary discharge diagnosis, payor, and discharge disposition as the program cohorts. The preliminary control cohorts were then propensity-matched to program cohorts based on 15 demographic, clinical, and socioeconomic indicators extracted from the enterprise data warehouse to achieve a sample size with balanced baseline characteristics with respect to group membership. Propensity matching variables included age, gender, ethnicity, race, marital status, employment status, payor, comorbid status based on the Charlson comorbidity algorithm, 17 visit type, mental health issue, defined as ICD-9 codes 290–319 in the 1–20 discharge code position, 18 3M All Patient Refined Diagnostic Related Group (APR-DRG) risk for mortality, 3M APR-DRG severity of illness, and prior hospital and emergency department utilization to any Sharp HealthCare hospital within the last 180 days.
The evaluation followed an intent-to-treat approach, and all enrolled program patients were included in the propensity matching calculation. Baseline characteristics were assessed for balance using standardized differences. The propensity score matching was investigated for efficiency, and logistic regression modeling was performed to investigate the odds of outcomes. All data management and statistical analyses were completed using SAS version 9.4 software (SAS Institute, Cary, NC).
Results
Sample Size
In total, 69 COPD and 80 HF patients enrolled into the program (Fig. 1). In total, 550 COPD and 478 HF control patients were initially identified in the data warehouse. Subsequent propensity matching of the 15 variables removed all discernible probability of selection to the program or control group. For the COPD cohort the likelihood ratio statistic dropped from 52.4 (p=0.004) to 7.3 (p=1.0), suggesting that all 15 variables had regression coefficients equal to 0 in the model predicting program assignment. For the HF cohort, the likelihood ratio statistic dropped from 70.5 (p<0.0001) to 11.6 (p=1.0), also suggesting that all 15 variables had regression coefficients equal to 0 in the model predicting program assignment. Final HF sample size after propensity matching was 59 control and 59 program patients (1:1). Final COPD sample after propensity matching was 174 control and 58 program patients (3:1).
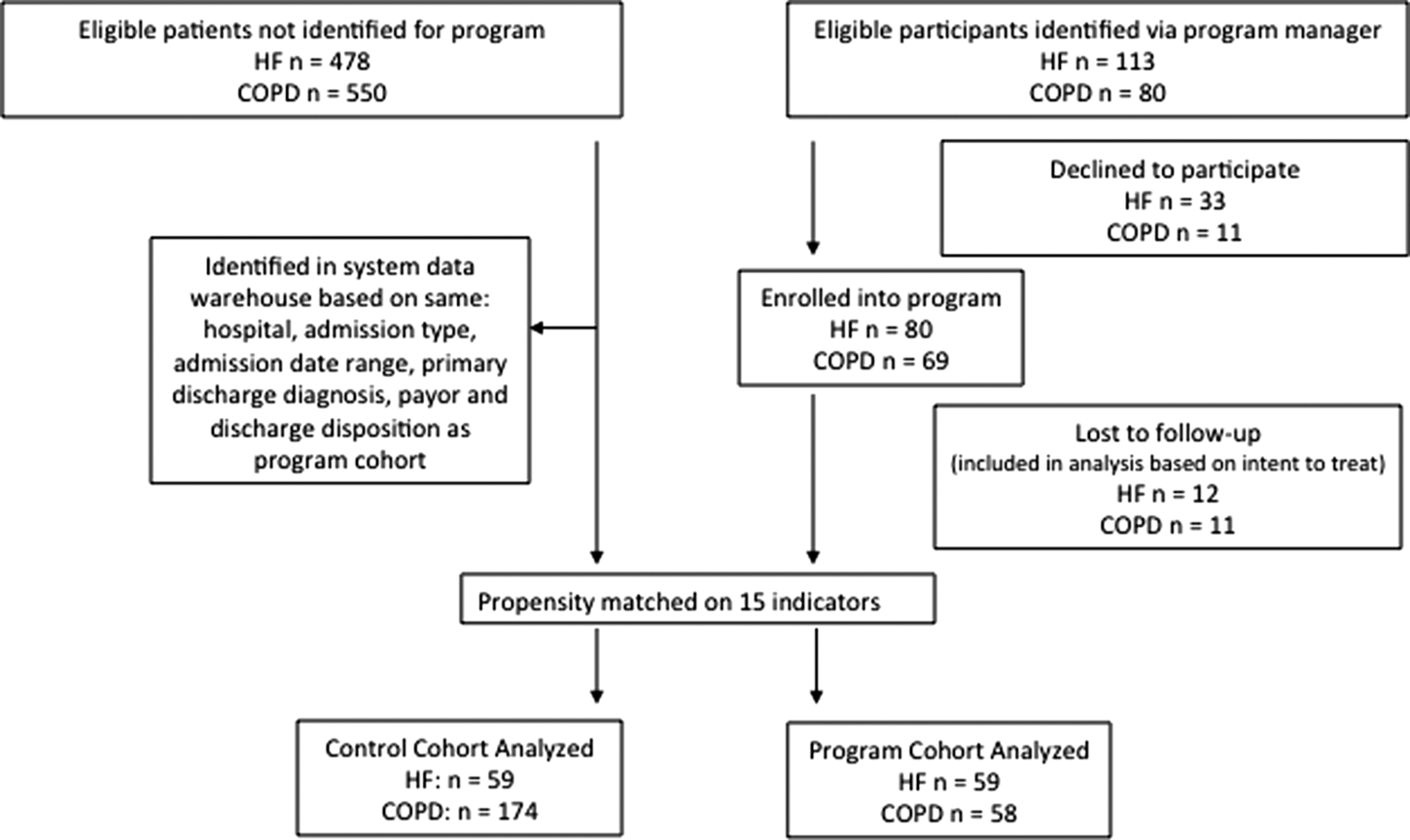
Flow diagram for remote monitoring program and control patients. COPD, chronic obstructive pulmonary disease; HF, heart failure.
Cohort Demographics
Cohort demographics are listed in Table 1. Overall the HF cohort was sicker, with a higher severity of illness, higher risk for mortality, greater incidence of comorbid conditions, a higher incidence of mental health issues, and a longer length of stay than the COPD cohort. Cohorts were similar in respect to acute care utilization prior to the index event.
Remote Monitoring Patient Demographics
Propensity-matching variables.
CHF, chronic heart failure; COPD, chronic obstructive pulmonary disease; ED, emergency department; HF, heart failure; LOS, length of stay; SD, standard deviation.
Program Adherence and Interventions
In total, 11 (16%) COPD patients and 12 (15%) HF patients did not complete the 90-day program. For the COPD cohort, 2 patients were lost to follow-up, 2 died before program end, and 7 were disenrolled per patient request or change in eligibility status. For the HF cohort, 2 patients were lost to follow-up, 1 died before program end, and 9 were disenrolled per patient request or change in eligibility. Table 2 describes telemonitoring interventions by category. Both cohorts averaged 70% or greater adherence to daily monitoring. The majority of alerts triggered by RMD data transmission did not necessitate contact by RMD staff (COPD, 59%; HF, 73%), for example, a weight loss alert that is expected after a change in medication. Symptom and vital sign alerts were the greatest triggers for patient contact, accounting for 27% of COPD and 19% of HF patient contact and patient contact.
Telemonitoring Interventions by Type
COPD, chronic obstructive pulmonary disease; HF, heart failure.
Primary Outcomes
Although there was a 37% reduction in ED use in the 30-day postdischarge period for COPD cohort compared with control patients (6.9% versus 10.9%), there was actually a 75% increase in ED use for the HF cohort (11.9% versus 6.8%) in the 30 days after the index discharge (Table 3). For the COPD cohort the reduced trend evened out by study end, with no difference in ED use at 180 days postdischarge compared with control patients (31% versus 31.6%). For the HF cohort the trend reversed dramatically, and by 180 days postdischarge there was a 46% reduction in ED use compared with control patients (23.7% versus 44%).
Remote Monitoring Program Outcomes
CI, confidence interval; COPD, chronic obstructive pulmonary disease; ED, emergency department; HF, heart failure; OR, odds ratio.
The trends for COPD and HF re-admission rates were similar across time periods. The 30-day re-admissions were reduced 50% for both chronic disease cohorts compared with control patients (COPD, 10.3% versus 21.8%, HF, 8.5% versus 17%). The trend in reduced re-admission continued through 180 days postdischarge (COPD, 46.6% versus 53.5%; HF, 35.6% versus 44.1%). The only statistically significant difference in primary outcomes was for COPD 30-day re-admission rates (10.3% versus 21.8%, p=0.02). Details are given in Table 3.
Functional Status
Total Clinical COPD Questionnaire scores (Table 4) decreased from a mean of 3.82 (±0.95) to 1.90 (±0.99). The difference in scores is well above the reported minimal clinically important difference threshold of 0.4, 19 suggesting patients who completed the program sustained clinically meaningful improvements in their health status.
Pre- and Postfunctional Status of Program Patients
COPD, chronic obstructive pulmonary disease; SCHFI, Self-Care of Heart Failure Index; SD, standard deviation.
The Self-Care of Heart Failure Index has three subscales: (1) Maintenance (physiologic stability), (2) Management (response to symptoms), and (3) Confidence (ability to perform maintenance and management). A score of 70 or above indicates achievement of each subscale. 16 Patients had not achieved maintenance at the start of the program (50.25±19.68) but had by program end (88.77±9.62). Patients had not achieved symptom management at the start of the program (13.6±13.79) but were almost at achievement by the program end (67.80±20.23). Patients had limited confidence at the start of the program (54.63±28.13) but had achieved confidence by the program end (91.95±11.77).
Satisfaction
Patients reported overall satisfaction with the RMD and felt the RMD was easy to use (HF score, 4.98; COPD score, 4.99), helped them to monitor their health (HF score, 4.84; COPD score, 4.56), and helped them to improve their health (HF score, 4.84; COPD score, 4.40). Details are given in Table 5.
Patient Satisfaction with Program Telemonitoring Equipment
Ratings were on a scale of 1 = No, definitely not, 2 = I don't think so, 3 = Maybe yes, maybe no, 4 = Yes, I think so, and 5 = Yes, definitely.
COPD, chronic obstructive pulmonary disease; HF, heart failure; SD, standard deviation.
Discussion
This study assessed the feasibility and preliminary outcomes of a 90-day transitional care program following an acute care event that integrated mobile health technology and home visits for underserved COPD and HF patients. Program participant outcomes were compared with those of a propensity-matched nontreated cohort identified through the enterprise data warehouse. The program was feasible and very satisfactory to patients. Adherence to daily reporting was greater than 70% for both cohorts. There were clinically meaningful trends in disease self-maintenance and acute care utilization between groups at 30, 90, and 180 days after program enrollment.
One of the most interesting findings was the similar trend in re-admissions for HF and COPD patients. Both showed the greatest reduction in re-admission at 30 days, with reduced but similar reductions (approximately 15%) at 90 days after the program end. It is notable that 41% of the HF cohort also had COPD, and 29% of the COPD cohort had HF. The total sample can generally be considered a complex multichronic disease cohort, with the additional burden of being underserved. The results suggest the program may be beneficial for other patient populations with complex conditions and socioeconomic health barriers.
A recent Cochrane review of telemonitoring for HF patients 20 concluded it appears to have benefits, but the mechanisms are unknown. The authors noted patients reported the constant link to expert care induced a sense of security with telemonitoring. Another Cochrane review of telemonitoring for COPD patients 9 reached similar conclusions: telemonitoring reduces acute care utilization, but the mechanisms are unknown. The authors noted personalized consistent feedback may be a benefit. In our study, all-cause re-admissions were reduced up to 90 days after the program end. This suggests the program was successful in sustaining patient self-maintenance beyond program end, which may be a mechanism for the reduction of acute care re-admissions. It could be that the upfront loading of information and attention via the PC during home visits were the driving force behind patients better managing their chronic disease, which was then reinforced through a daily habit of uploading information via the telemonitoring technology. Empowering this patient population is difficult in the best of circumstances; add illness, limited finances, and lack of resources, and it can seem impossible. This feasibility study showed the promise of telemonitoring integrated into a transitional care program to promote positive effects on patient engagement in their own care.
What remains unclear is the individual effect of telemonitoring versus transitional care in influencing outcomes noted. Does one affect change more than the other, or does the implementation of both create a synergistic effect? In our study, it was noted that extensive care coordination was necessary to ensure the underserved study participants got the assistance they needed receiving their medications, transportation to follow-up visits, etc., which is why home visits were structured into the program. In a recent review of transitional care interventions, 21 the authors found inconclusive evidence for telemonitoring alone in reducing re-admissions, and there was very limited evidence for all programs in reducing 30-day re-admissions. Our study included both telemonitoring and home visits and was most beneficial in reducing 30-day re-admissions. The benefit of telemonitoring for complex patients, compared with patients with lower severity of illness and risk for mortality, was also found in another recent systematic review. 22 This study provides necessary data on short-term acute care utilization related to telemonitoring use and suggests telemonitoring in combination with transitional care home visits is a potential beneficial transitional program option for this complex patient population.
Limitations
It is important to examine the separate components of our intervention to determine the most effective components related to improved patient health and the mechanism of action. This includes a better understanding of the scalability of telemonitoring care transition programs based on multiple components. It should also be noted that based on a 1:1 ratio in each cohort, 80% power, 5% alpha, and a finding of an approximate 50% reduction in 30-day re-admission, statistical significance would have been established if the cohort was closer to 359 patients for COPD and 528 patients for HF. A more robust sample size and randomization would yield greater ability to establish additional precision and generalizing capability.
Conclusions
This study showed that a transitional care program incorporating telemonitoring and home visits for COPD and HF patients with limited financial resources is feasible and has the potential to reduce acute care utilization during and after program end. The results warrant further examination, including a well-powered, full-scale experiment examining telemonitoring as part of a transitional care program to improve the health and self-care maintenance of underserved patients with chronic care disease.
Footnotes
Acknowledgments
Funding for this study's program intervention was provided by a grant from the Center for Technology and Aging (a program of the Public Health Institute, through a grant from the California HealthCare Foundation), the SCAN Foundation, and the San Diego Beacon Community.
Disclosure Statement
No competing financial interests exist.