
Abstract
Introduction
Critical care of infants, children, and adult patients with congenital heart disease require experienced and skilled staff. The scarcity of such specialized physicians is a constant and widespread problem, especially in developing countries. 1,2 Telemedicine has become a useful instrument to provide clinical care and medical education at a distance, in both the intensive care and pediatric cardiology settings. 3 The use of mobile videoconference systems allows remote intensivists to have direct access to the patient's room, vital signs, and monitoring during the communication, and several studies have demonstrated it as a feasible and reliable option to provide medical care. 3 –8 As bigger areas can be served, it may enable a better service to the patient, save time, and reduce the costs for physicians and families. 3
Reports from the intensive care setting have shown conflicting findings related to any effect from a telemedicine system in patient outcomes, 9 but some investigators were able to demonstrate a decrease in mortality and better clinical practice adherence to best evidence-based guidelines while applying systematic telemedicine interventions within a multilayered quality project. Furthermore, in the telemedicine group a decrease in preventable complications and a shorter length of stay (LOS) were detected. 8
Nevertheless, the ideal format to deliver medical care in the international telemedicine setting has not been established. In order to do so, we have previously reported our initial experience with the delivery of telemedicine-assisted pediatric cardiac critical care (PCCC) in an international setting, with a survey demonstrating a high rate of remote physician satisfaction, 10 as well as our multicenter experience during the first 2 years of our international telemedicine program, finding significant differences in staff composition, patient population, and perception of needs among the different remote centers, making a “one size-fits-all” approach unworkable. 11
The objective of this study was to describe factors associated with cardiac intensive care unit (CICU) and hospital survival, as well as hospital LOS, during the first 10 months of the implementation of an international telemedicine program in PCCC in a subset of patients from our previous report, 11 specifically, the ones from the Fundacion Cardiovascular de Colombia (FCV), Bucaramanga, Colombia, in anticipation for future prospective interventions.
Materials and Methods
This was a pre- and postintervention study. A retrospective review was performed of clinical records for all cardiovascular admissions in patients admitted to the CICU at FCV and a telemedicine clinical database of those for whom teleconsultation was done by the Children's Hospital of Pittsburgh of UPMC (CHP), Pittsburgh, PA, from July 15, 2011 to May 15, 2012 (Telemed group), compared with patients admitted during a previous period from July 1, 2010 to February 1, 2011 (Pre-Telemed group). Telemed patients represent a subset of patients from our previously reported multicenter study. 11
The institutional review board of both institutions approved this study separately.
Centers' Characteristics
The FCV is a 26-year-old tertiary-level hospital treating patients with heart disease, both children and adults. It has a general pediatric unit with 22 beds, a CICU with 24 beds, a general pediatric intensive care unit with 10 beds, and neonatal intensive and intermediate care units, each one with 20 beds. CHP is a state-of the-art children's hospital with 289 licensed beds. It has a 36-bed pediatric intensive care unit and an independent 12-bed CICU.
Program Description
A complete description of our international telemedicine program in PCCC as well as pertinent technical information has been published elsewhere. 10,11
In brief, a tele-intensivist from the CHP CICU reviewed patients, providing monitoring and support as well as pertinent studies, and gave formal medical advice at the request by the remote attending physician at the FCV. Patients could be followed as many times as needed according to local physician criteria.
A real-time intervention was defined as any activity performed according to tele-intensivist recommendation and taking place during teleconsultations.
Data Collection
Unidentified data were extracted from our prospectively collected database (e-CICU database). We included specific telemedicine information such as date of consultation, consult type (first versus follow-up), evaluated information (clinical data, X-ray, monitor, electrocardiogram, echocardiogram, computer-assisted tomography scan, angiography, etc.), activities (diagnostic study interpretation, diagnostic change, real-time intervention), type of patient (preoperative versus postoperative and medical), recommendations given, and connection quality.
Surgical procedures were classified according to Risk Adjustment for Congenital Heart Surgery (RACHS)-1 categories. This method allows for discrimination in mortality risk according to surgical complexity, with 1 being the group with the lowest and 6 the one with highest anticipated mortalities, respectively. 12
In addition to the telemedicine data, a second group of data was collected by the staff from the FCV, including demographic data, cardiac diagnosis, operative data including type of surgery, cardiopulmonary bypass and cross-clamp times, use of circulatory arrest, and minimal transoperative temperature.
The primary outcome was hospital mortality. Secondary outcomes were CICU and hospital LOS.
Data Analysis
SPSS version 20 software (SPSS, Inc., Chicago, IL) was used for statistical analysis. We conducted descriptive statistics for all patients in each group (Pre-Telemed, Telemed, and Teleconsulted). We did a log transformation for continuous variables with a skewed distribution. We performed a comparison between study periods and between teleconsulted and nonteleconsulted patients within the Telemed group. For categorical variables we conducted Fisher's exact test and t test for continuous variables. For primary cardiac surgery, we compared RACHS-1 distribution between periods by the Mann–Whitney U test. For comparison of RACHS-1 adjusted CICU and hospital LOS between study periods we used two-way analysis of variance; when the equality of error variances test was significant we used the Kruskal–Wallis test. Results were considered significant when the p value was <0.05. Potential risk markers, including weight, age, RACHS-1 category higher than >3, extracorporeal membrane oxygenation (ECMO), presence of low cardiac output syndrome, sepsis, or necrotizing enterocolitis, bypass time longer than 150 min, circulatory arrest during surgery, and cross-clamp time longer than 60 min, were identified and included in the full multivariate regression model as covariates. For hospital mortality we used Cox proportional hazards, and for CICU and hospital LOS we used a linear regression model.
Results
During the study period, there were, in total, 676 hospital admissions for 571 patients. After 43 admissions were excluded because of missing data as well as 82 additional ones in noncardiovascular patients, in total, 551 cardiovascular admissions in 533 patients were included for analysis: 269 and 282, respectively, for the pretelemedicine and telemedicine periods. A flowchart of patient admissions is shown in Figure 1. Demographic data and operative variables are described in Tables 1 and 2.
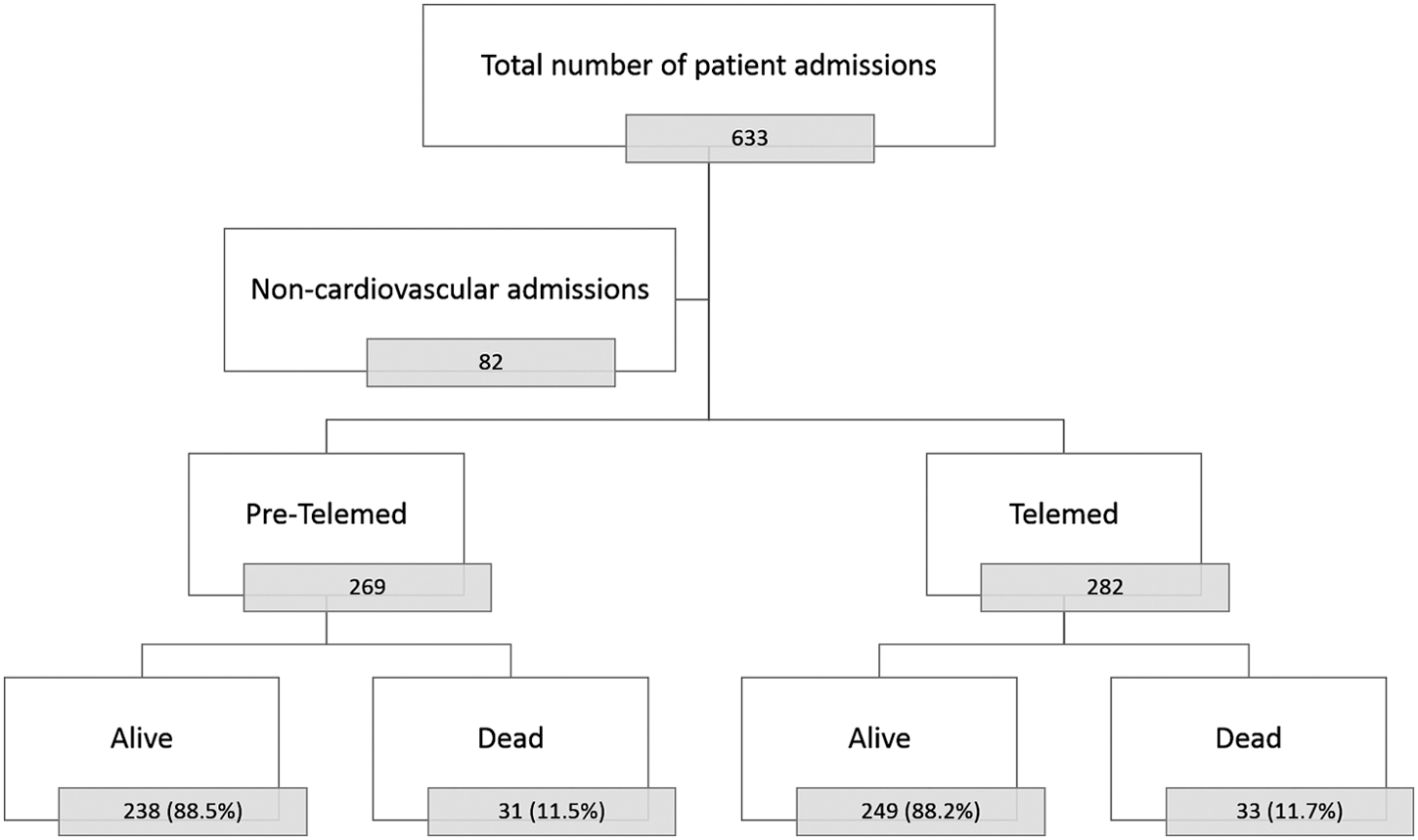
Flowchart of study patients. Pre-Telemed, pretelemedicine; Telemed, telemedicine.
Comparison Between Study Periods
Data are median (minimum, maximum) values unless indicated otherwise.
Percentage calculated from total number of patients.
CICU, cardiac intensive care unit, DIC, disseminated intravascular coagulopathy; ECMO, extracorporeal membrane oxygenation; LCOS, low cardiac output syndrome; LOS, length of stay; NEC, necrotizing enterocolitis; PAH, pulmonary artery hypertension.
Comparison Between Study Periods in Cardiac Surgical Cases
Data are median (minimum, maximum) values unless indicated otherwise.
By Mann–Whitney U test.
CICU, cardiac intensive care unit; LOS, length of stay; RACHS, Risk Adjustment for Congenital Heart Surgery.
Telemedicine Study Period
During the telemedicine study period, 264 patients were admitted, including 71 patients receiving teleconsultations. Hospital and CICU admissions were 303 and 312, respectively.
Telemedicine period patients had similar demographic variables and RACHS-1 distribution compared with pretelemedicine patients; however, there were higher proportions of patients with cardiovascular diagnosis (Telemed versus Pre-Telemed, 93.1% versus 81.5%; p<0.001) and ECMO cases (Telemed versus Pre-Telemed, 4.9% versus 1.6%; p=0.030).
Teleconsultations
One hundred eighty-nine telemedicine consultations were conducted for 71 (12.4%) patients. Thirty-three telemedicine encounters were excluded because hospital admission occurred before the study period or information was incomplete.
The number of teleconsultations by patient ranged from 1 to 11, with a mean of 2. Characteristics of teleconsultations are described in Table 3. In total, 42 real-time interventions were documented in 34 teleconsultations (21.8%). Three hundred twenty-one recommendations were given. The most frequently recommended surgery by teleconsultation was ventricular septal defect closure (n=10), followed by arterial switch operation (n=6), pulmonary artery banding (n=6), re-intervention (n=5), and hybrid approach (n=4).
Teleconsultation Characteristics
CICU, cardiac intensive care unit, ECMO, extracorporeal membrane oxygenation.
Teleconsulted Patients
Characteristics of patients receiving teleconsultation are described in Table 4. The most frequent diagnosis in teleconsulted patients was atrioventricular canal (n=7, 9.9%), followed by hypoplastic left heart syndrome (n=6, 8.5%), ventricular septal defect (n=5, 7%), and transposition of great arteries (n=5, 7%). The most common associated factors present in these patients were arrhythmia (n=12, 17%), low cardiac output syndrome (n=7, 9.9%), sepsis (n=7, 9.9%), and pulmonary artery hypertension (n=7, 9.9%). Ten (14.1%) were ECMO cases.
Telemedicine Period Patients According to Teleconsultation Status
Data are median (minimum, maximum) values unless indicated otherwise.
By Mann–Whitney U test.
CICU, cardiac intensive care unit; DIC, disseminated intravascular coagulopathy; ECMO, extracorporeal membrane oxygenation; LCOS, low cardiac output syndrome; LOS, length of stay; NEC, necrotizing enterocolitis; PAH, pulmonary artery hypertension; RACHS, Risk Adjustment for Congenital Heart Surgery.
Within the Telemed group, teleconsulted patients had a significantly increased proportion of male patients and a younger age, had higher surgical complexity as categorized by RACHS-1 distribution, and longer bypass and cross-clamp times compared with patients without teleconsultation (Table 4).
Outcome Analysis
Overall surgical CICU and hospital mortalities were 7.2% and 9.1%, respectively, for the telemedicine and pretelemedicine periods. RACHS-1 adjusted CICU and hospital survival were similar between study periods (Table 5).
Risk Adjustment for Congenital Heart Surgery-1 Adjusted Survival for Primary Surgical Cases
Data are n (%).
CICU, cardiac intensive care unit; RACHS, Risk Adjustment for Congenital Heart Surgery.
CICU and hospital LOS intervals were significantly shorter in the telemedicine period as described in Table 1 and Figure 2.
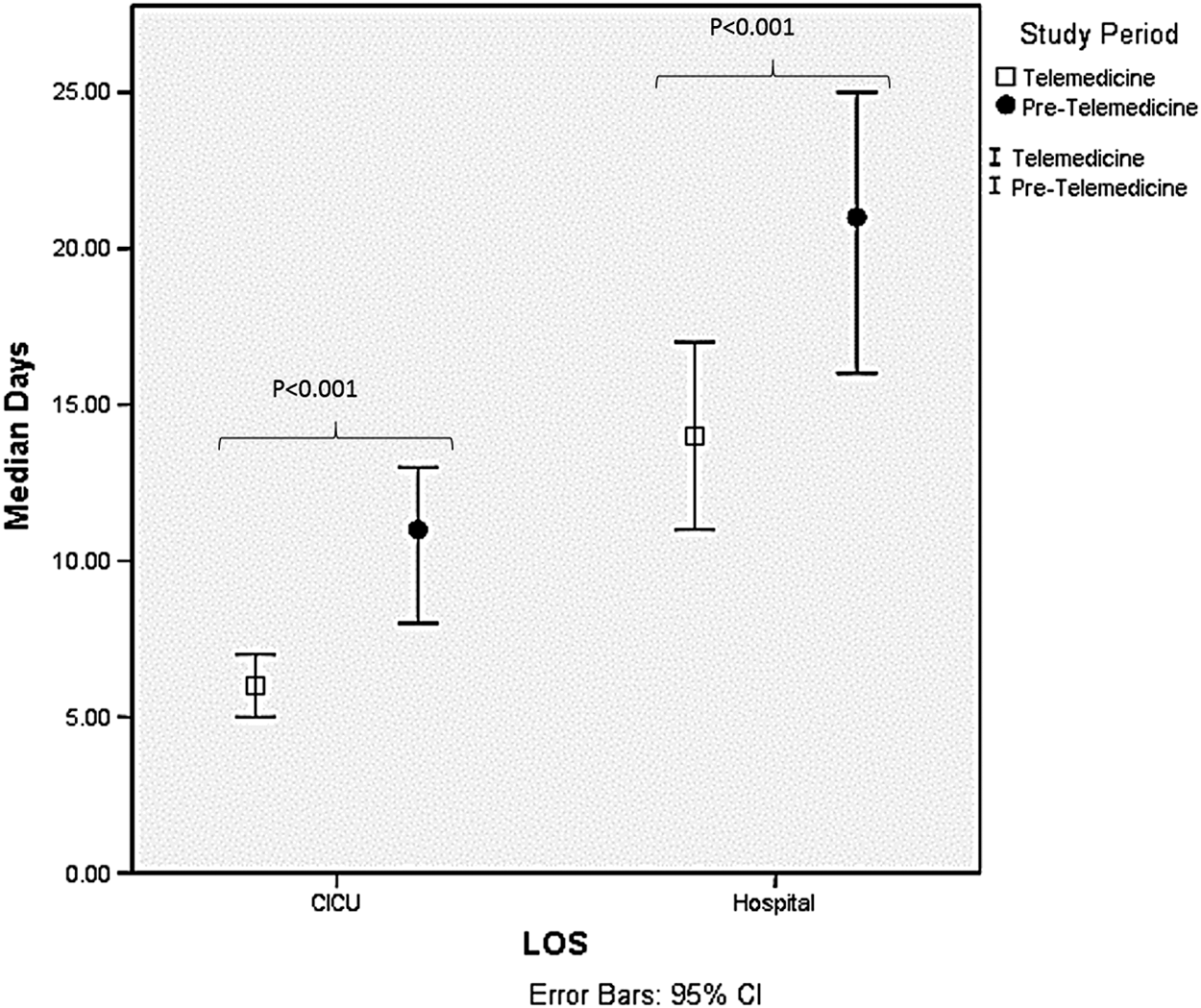
Length of stay (LOS) of cardiovascular patients. Error bars indicate 95% confidence intervals. CICU, cardiac intensive care unit.
RACHS-1 adjusted CICU and hospital LOS are described in Table 6 and Figures 3 and 4, respectively.
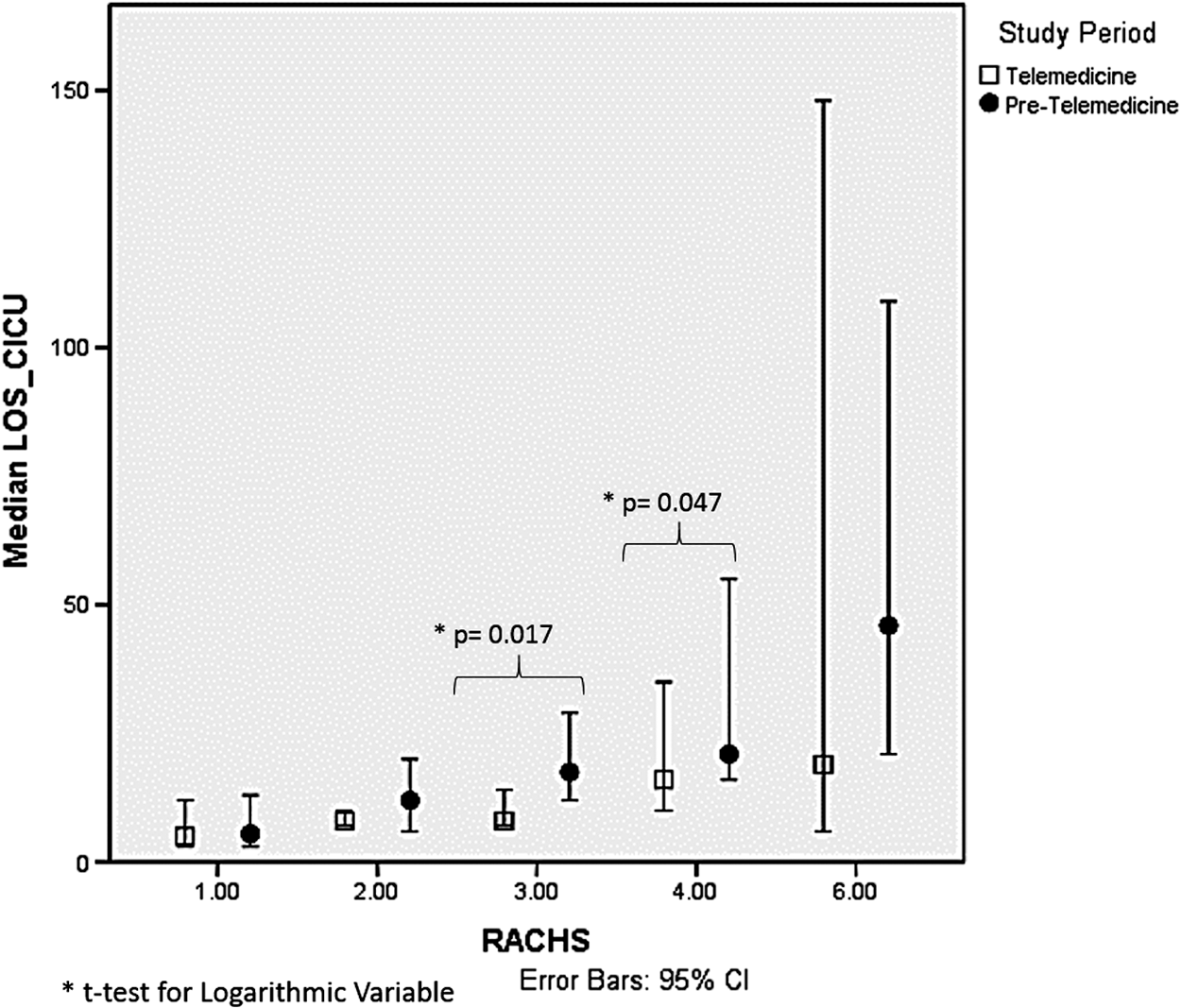
Cardiac intensive care unit (CICU) length of stay (LOS) by surgical category (Risk Adjusted for Congenital Heart Surgery [RACHS]-1). Error bars indicate 95% confidence intervals. *By t test for logarithmic variable.
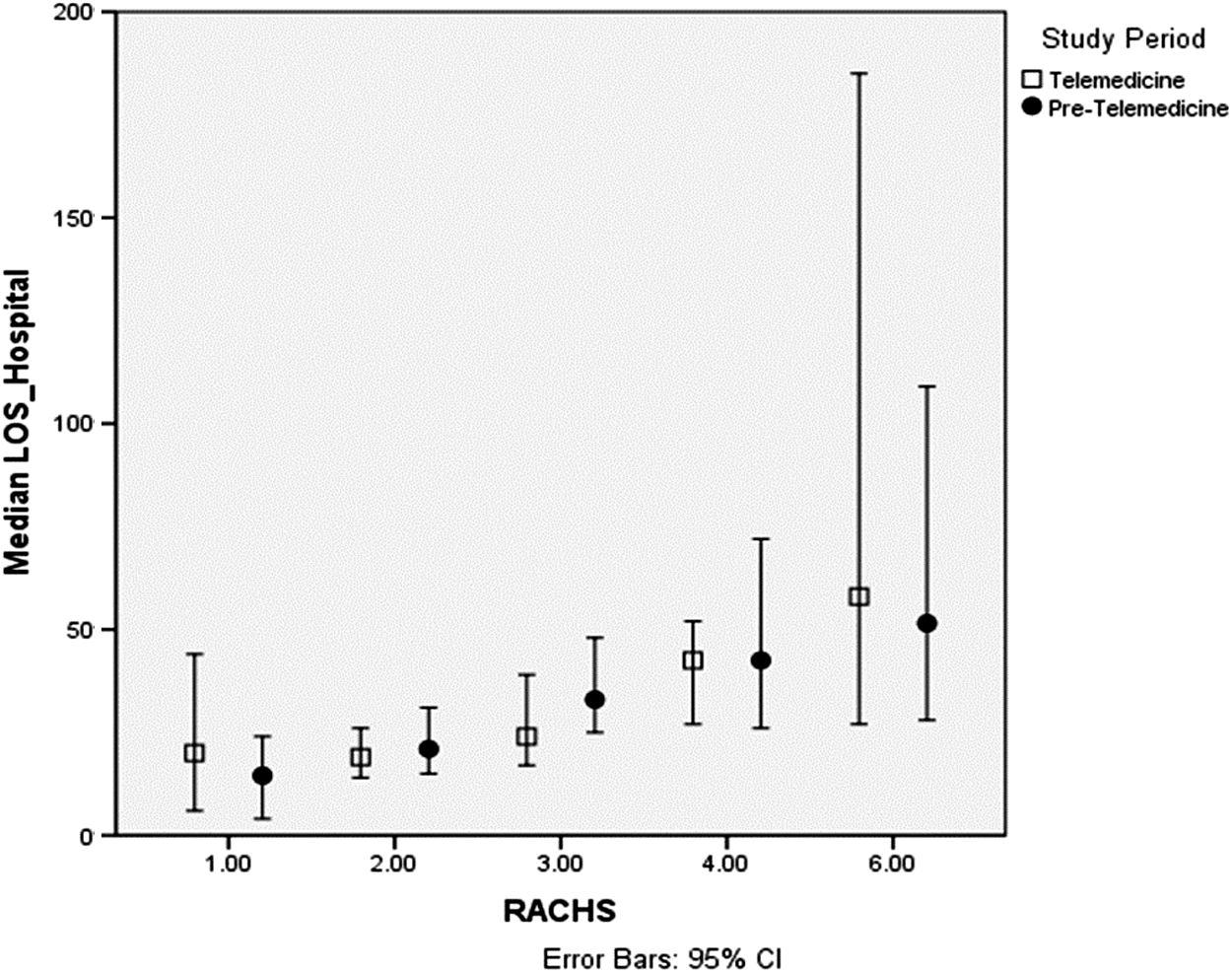
Hospital length of stay (LOS) by surgical category (Risk Adjusted for Congenital Heart Surgery [RACHS]-1). Error bars indicate 95% confidence intervals.
Risk Adjustment for Congenital Heart Surgery-1 Adjusted Length of Stay for Surgical Cases
Data are median±standard deviation values.
By t test for logarithmic variable.
CICU, cardiac intensive care unit; RACHS, Risk Adjustment for Congenital Heart Surgery.
After potential confounding factors were examined using a Cox proportional hazard model, patients with higher RACHS-1 categories, lower weight, bypass time longer than 150 min, use of circulatory arrest during the procedure, and the presence of sepsis or NEC were associated with higher hospital mortality (Table 7).
Multivariate Analysis for Hospital Mortality
CC, cross-clamp; CI, confidence interval; ECMO, extracorporeal membrane oxygenation; HR, hazard ratio; LCOS, low cardiac output syndrome; NEC, necrotizing enterocolitis; RACHS, Risk Adjusted for Congenital Heart Surgery.
To identify independent risk factors for prolonged CICU LOS and hospital LOS, a multivariate linear regression model was conducted. Lower weight, ECMO, and cross-clamp time longer than 60 min were identified as significant (Table 8).
Linear Regression Model
Estimates are of the effect on unit increase in absolute value of length of stay.
CICU, cardiac intensive care unit; ECMO, extracorporeal membrane oxygenation; LCOS, low cardiac output syndrome; NEC, necrotizing enterocolitis; RACHS, Risk Adjusted for Congenital Heart Surgery.
Discussion
Different models of care have been proposed for the management of critical patients with congenital heart disease, and one of the most accepted one includes the use of a dedicated CICU covered by pediatric cardiac intensivists. 13 Consequently, there is a demand for a high number of skilled physicians, who are lacking worldwide. At the same time, every pediatric cardiovascular center team goes through a necessary learning curve in the process of acquiring collective expertise, with a potential for an excess in complications or problems at multiple levels in the process of care. A telemedicine model can be an alternative to the scarcity of specialized physicians, and it can be used to leverage quality improvement interventions, thus potentially shortening the learning curve while providing real-time quality assurance to remote teams.
Since 2010, CHP developed an international telemedicine program in PCCC, and this study represents the first reported experience related with patient outcome in this setting.
Typically, telemedicine models in the critical care setting (a complex system) allow for complex interventions, potentially impacting both the CICU workflow and model of care. Consequently, its effects may be seen in admitted patients irrespective of their consultation status. 14 Given this and the fact that different interventions unrelated to telemedicine were being implemented at the same time (i.e., an increase in the proportion of cardiovascular patients) as well as the relatively short period of observation, we are cautious in ascribing a distinct causal association between patient outcome and the use of telemedicine technology. Nonetheless, there are some observations worth mentioning.
In cardiovascular patients, there was no significant difference in hospital mortality. Adjusted for surgical complexity (RACHS-1) in surgical patients, there was no significant difference in CICU and hospital mortality. This is not unexpected given the short observation time since program inception, as discussed above.
There was a significantly shorter CICU and hospital LOS for cardiovascular patients in the telemedicine period compared with those in the pretelemedicine period. Likewise, in surgical patients there was a significantly shorter CICU LOS; in particular, both the preoperative and CICU LOS were significantly shorter in the telemedicine period, suggesting a possible effect of telemedicine consultations in earlier surgical decisions. After adjusting for surgical complexity, we observed this decrease mainly in surgical complexity categories 3 and 4, and in category 6 patients there was also a decrease that did not reach significance, probably because of the small sample size in that subgroup of patients. We believe these findings suggest that telemedicine use had its major impact in higher surgical risk patients.
A systematic approach focusing on specific aspects of care may be an important component of effective telemedicine interventions. Therefore, we sought to define specific variables associated with survival and LOS: namely, patients in the higher surgical complexity categories (RACHS-1 of >3), lower weight, longer bypass times (>150 min), use of circulatory arrest during surgery, and the presence of necrotizing enterocolitis or sepsis were identified for mortality, whereas lower weight, use of ECMO, and longer cross-clamp times (>60 min) were identified for hospital LOS. These findings are in accordance with multiple previous reports on series of pediatric patients postoperative from heart surgery, including the analysis of the European Association for Cardiothoracic Surgery Congenital Database, 15 demonstrating that neonates with lower body weight, higher Aristotle Score, longer cardiopulmonary bypass time, longer aortic cross-clamp time, longer circulatory arrest time, and univentricular physiology were risk factors for hospital mortality.
These findings are very important to us in order to modify our current telemedicine model for these patients, so we can focus our attention in patients with higher risk of mortality and prolonged LOS, as well as focusing on preventive strategies for selected complications with the goal to produce a major impact in patient survival and overall quality of care.
Finally, teleconsulted patients were significantly younger, had longer bypass and cross-clamp times, and different RACHS-1 distribution, with a higher frequency of complex heart surgery, which may explain their appropriately lower CICU and hospital survival and longer CICU and hospital LOS.
Study Limitations and Future Directions
The retrospective nature of this study limited a more powerful data analysis. In particular, we were not able to make a more detailed analysis in nonsurgical patients. Subgroup sample size was small when patients were analyzed by RACHS-1 categories. Other variables among multiple interventions during the typical hospital stay of these patients with the potential to alter outcomes were not included. Further research is warranted to establish whether a more systematic approach, considering the findings in this report, will be of additional benefit for children with cardiovascular disease in the international cardiac critical care setting.
Conclusions
Compared with a historical cohort, an international telemedicine service in PCCC was associated with lower CICU and hospital LOS in pediatric cardiovascular patients. Patients postoperative of congenital heart surgery had comparable survival adjusted for surgical complexity but shorter CICU and preoperative LOS. Prospective telemedicine interventions aimed to decrease mortality and LOS should focus on patients with a higher RACHS-1 category, neonates and lower-weight infants, and those with prolonged operative times and selective perioperative techniques and complications. Potential effects from such interventions may impact both teleconsulted and nonteleconsulted patients.
Footnotes
Acknowledgments
We are indebted to the staff of the Fundacion Cardiovascular de Colombia for their enthusiastic and unwavering support during the implementation of our telemedicine program. The project described was supported by the National Institutes of Health through grants UL1 RR024153 and UL1TR000005.
Disclosure Statement
No competing financial interests exist.