
Abstract
Recent discussions have focused on using health information technology (HIT) to support goals related to universal healthcare delivery. These discussions have generally not reflected on the experience of countries with a large amount of experience using HIT to support universal healthcare on a national level. HIT was compared globally by using data from the Ministry of the Interior, Republic of China (Taiwan). Taiwan has been providing universal healthcare since 1995 and began to strategically implement HIT on a national level at that time. Today the national-level HIT system is more extensive in Taiwan than in many other countries and is used to aid administration, clinical care, and public health. The experience of Taiwan thus can provide an illustration of how HIT can be used to support universal healthcare delivery. In this article we present an overview of some key historical developments and successes in the adoption of HIT in Taiwan over a 17-year period, as well as some more recent developments. We use this experience to offer some strategic perspectives on how it can aid in the adoption of large-scale HIT systems and on how HIT can be used to support universal healthcare delivery.
Introduction
Recent efforts at healthcare reform in the United States have ignited discussions about the organization of national health systems. One issue related to this discussion is how health information technology (HIT) can help achieve goals related to universal healthcare delivery. 1 In addition to other structural and cultural changes, it is hoped, for example, that usage of HIT on a large scale (i.e., national scale) will support cost containment and overall efficiency and quality of the system and thus make universal healthcare more achievable. 1,2
To date, these discussions have mostly relied on visions about the potential for future HIT systems 1 but have not included experiences taken from using national-scale HIT systems to support universal healthcare. In the United States, such experience is difficult to draw upon as large-scale HIT systems have proven more difficult to implement in practice than it was hoped for a few years ago. The reasons for this include both technical and sociotechnical (organizational) factors related to successful implementation and utilization of HIT. 3 A technical perspective is that HIT systems generally need to be custom-built or adapted on-site for healthcare organizations, and this is a difficult task due to the complexity of these organizations. 3,4 The fragmented healthcare system in the United States presents additional challenges compared with other countries, as it can be difficult to address all the stakeholders' concerns regarding the costs and benefits of HIT systems in order to allow them to unite around one overall implementation strategy. 4
There are several other countries, such as the United Kingdom, Denmark, Norway, and Australia, however, with experience using national-scale HIT systems to support universal care. 5,6 In Taiwan, for example, universal healthcare is organized under the Bureau of National Health Insurance (BNHI), and the healthcare system is supported by HIT in a more extensive way than in many other countries. National-level HIT systems aid in administration, clinical care, and public health. 6,7
The HIT system in Taiwan is interesting to consider in these discussions as Taiwan has been quite successful at building a high-quality and efficient healthcare system. 8 In 2008, Taiwan spent about 7% of gross domestic product (GDP) on healthcare and covered over 99% of its population with a satisfaction rate of above 83%. 9 The major health indicators like life expectancy at birth are almost the same as the United States, and the infant mortality rate is also comparatively better in Taiwan (Table 1). 8,10
A Summary of the Major Health Indicators, Utilization, and Expenditure for Taiwan and the United States
GDP, gross domestic product.
In this article, we present an overview of some key historical developments and successes in the adoption of HIT in Taiwan over a 17-year period. Our goal is to contribute to the discussions around how large-scale HIT systems can support universal healthcare and to help efforts at implementing HIT for this purpose by addressing the following research questions: 1. How has national-level HIT aided the universal healthcare system in Taiwan, and what does that tell us about how national-level HIT might support healthcare systems in other countries? 2. What key lessons can be taken from the Taiwanese experience that can aid in the successful adoption of large-scale (i.e., national-scale) HIT systems in other countries?
The Taiwanese Healthcare System
Taiwan is an Eastern Asia Island with a population of 23 million. Despite its political isolation internationally, Taiwan is a leading exporter of hi-tech products, particularly computer technology, and has a GDP per capita of U.S. $38,200, 10 making it one of the richest countries in the Asia–Pacific region. 9
Since 1995, the national health insurance in Taiwan has been run by BNHI, one of the bureaus of the Department of Health (DOH), and enrollment is mandatory for all citizens and legal residents. All public and private healthcare providers (about 19,000 in total) are affiliated with the program, including regional and district specialist hospitals, local clinics, and general practitioners' offices. Citizens may obtain services from the hospitals and/or clinics they choose and can make appointments with a specialist without needing a referral from a general practitioner and without needing to spend extra time on a waiting list. There is a small financial incentive for patients to go through a general practitioner and receive a referral, but in practice many patients choose to visit a specialist directly.
Although the single-payer system in Taiwan has generally been a success, there are some challenges with its delivery. 9 Cultural factors result in a high usage rate of healthcare by the citizens. Today each person in Taiwan visits a health facility on average 14–15 times annually, 9 whereas Americans visit only four times a year. There are challenges related to the overutilization of emergency rooms. 11 Taiwan faces challenges similar to those faced by healthcare systems in other developed countries, such as an increase in costs due to technological advances that increase the cost of care while contributing to the longevity of the population.
Despite these challenges, as noted in Figure 1, Taiwan's national health expenditure as a percentage of GDP has been maintained at a fairly constant rate for the last 17 years. Although in this article we focus on the role of HIT in helping to support the healthcare system, there are also other issues related to how the healthcare system is organized that contribute to its overall efficiency and quality. BNHI has introduced a global budget 2,9 and diagnosis-related group payment system to cap costs. This policy has resulted in the reduction of salaries along with increased working hours for healthcare staff. BNHI has full control over provider payments and over the cost of pharmaceuticals and procedures. Administrative costs are quite low, with the administrative costs of BNHI being only 2.23%, for example, compared with 25–30% of the healthcare expenditure in the United States being devoted to administration. 2,12

Health expenditure trends by gross domestic product (GDP) for the United States and Taiwan (TW).
The Role of HIT in Taiwan
The usage of HIT in Taiwan has been strategically pursued since the inception of the BNHI. The evolution of the national-scale HIT system is shown in Figure 2. The first component was implemented in 1995, when it became mandatory that all health providers should submit electronic claims (e-claims) to BNHI. The e-claims must include information like the demographics of the patient, diagnosis, laboratory investigations ordered, and medications prescribed. 6 As the e-claims include such extensive information, the system became an extensive data repository.
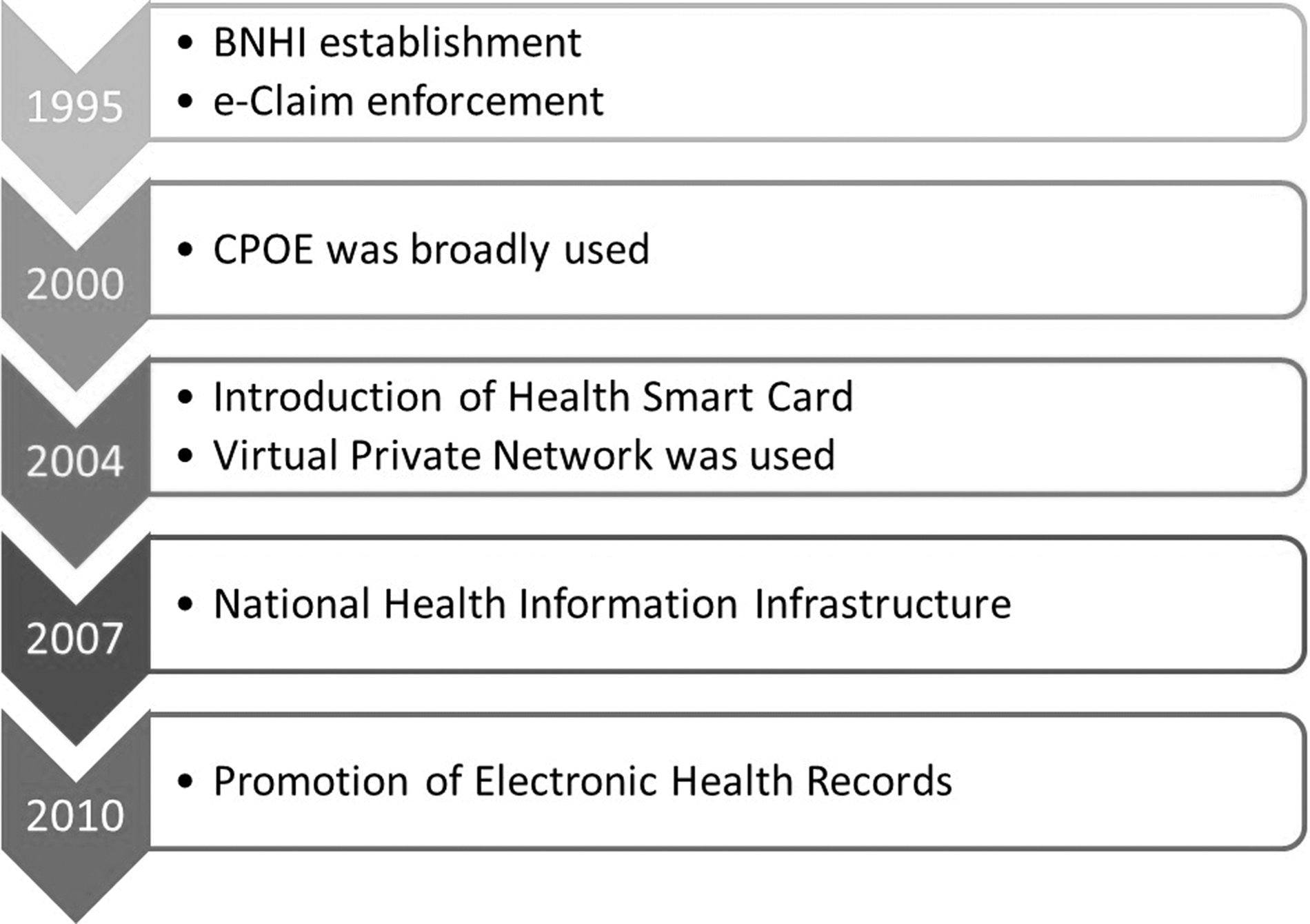
Evolution of health information technology in Taiwan. BNHI, Bureau of National Health Insurance; CPOE, computerized physician order entry; e-Claim, electronic claims.
The e-claims database accumulates records for hundreds of millions of patient visits each year and allows the DOH to gain access to daily reports that summarize all the claims submitted to the BNHI. 13
The national-scale HIT system is also used in various ways to reduce abuse and misuse of health resources. 9 Medical institutions must file an application and receive approval before surgery. Efforts are taken to reduce medical treatments prone to misuse, such as heart, liver, and bone marrow transplantation, radiation therapy, stereotactic radiosurgery, and other high-technology treatments. In 2000, in total, 633 cases were fined, suspended, or terminated in contracts. 9 BNHI also traces and counsels individuals who make an excessive number of outpatient visits. This prevents waste by guiding these heavy users of the healthcare system on how to properly seek treatment. Malpractice and medication errors can be traced, and measures can be taken to reduce them. 14
The e-claims database has become a resource for researchers to develop knowledge-based and evidence-based guidelines for best practices and computerized decision support systems. 15 Annually, hundreds of research articles are published based on analysis of the data contained in the e-claims database. The e-claims system has had a positive impact on the adoption of computerized physician order entry systems and electronic medical record (EMR) systems, as it resulted in providers implementing a workflow that included extensive input of digital information.
Over the years additional measures have been taken by the DOH to further the development of HIT on a national scale. A common information security infrastructure was implemented, an EMR interoperability subsidy program was created, and the DOH took additional measures to make healthcare administration more efficient with HIT. 8 These measures included the adoption of health smart cards in 2004, as a means for the identification of patients, physicians, and healthcare facilities, and medical affairs management systems that provide the DOH and local public health agencies with a framework for managing medical, pharmaceutical, nursing, and psychiatric rehabilitation institutions. 6
The adoption of EMR systems in Taiwanese hospitals is fairly high, compared with other developed countries. 6 The computerized physician order entry and EMR usage rates have become high, which has supported the adoption of computerized decision support systems. Such systems are proven to improve the safety and quality of the healthcare system. 16,17 One study from Taiwan, for example, reported that with the use of electronic prescriptions, medication errors have been reduced from 4% to 0.71%. 18 The health smart card system provides clinical advantages because the essential information contained in the cards helps to inform treating physicians about drug/food allergies, immunization status, medical procedures, and willingness to be an organ donor. 14,19
HIT is used in order to overcome geographical barriers to delivering equitable care in 30 townships in mountainous regions and 8 townships on outlying islands. A “medical care network” has been established that consists of 145 points of service in remote areas, as well as teaching hospitals, medical centers, and regional hospitals have joined the network to provide teleconsultation. It also is used as a platform to provide training for medical personnel. 9 This is a notable achievement when considering the extreme difficulty that telemedicine experts consider is faced for the development of national-level telemedicine systems. 20
The BNHI has sought to use the Internet in order to improve general functioning and planning of the healthcare system by opening a two-way dialog with different stakeholders that might normally have trouble communicating with health authorities. The government allows the public to gain information through the Internet on BNHI in the shortest possible times and allows them to communicate and share opinions and engage in discussions with BNHI via e-mail. 9 More recently, we also have used Facebook in order to better understand issues related to challenges with emergency rooms, as expressed by the health staff. 11
Looking toward the future, the DOH is continuing to improve the HIT infrastructure in Taiwan to expand the benefits to the healthcare system. One of the more interesting projects that has been initiated over the past few years, for example, is that the information inputted into the e-claims system is being used to develop an information exchange system that will reduce the number of tests repeated when a patient visits a new hospital. 8 The e-claims system is already being used by several hospitals, with national-scale implementation expected in the next few years.
Discussion
The systems described above illustrate how HIT is used to support universal healthcare delivery in Taiwan, which is driven by e-claims adoption. They provide advantages on a national scale in healthcare administration, clinical medicine, and public health. They also enable synergy among these areas, as data created in one bureau of the DOH can be used to support other bureaus. 6,21 The experience in Taiwan thus provides a concrete example of how HIT can be used to generally support universal healthcare, as recently proposed by Fineberg. 1
As healthcare systems vary greatly among countries, it is worth discussing how the experience in Taiwan can provide strategic perspectives on how to approach the adoption of large-scale HIT systems to support universal healthcare more generally. It has been noted that large-scale integrated institutions have advantages in adopting HIT, for example, due to their ability to more clearly manage potential conflicts among different stakeholder groups. The Taiwanese experience is similar to that in countries such as United Kingdom, Denmark, Norway, and Australia, as they have a single-payer system and use HIT extensively. 5,6 Together, these experiences suggest that the single-payer model might have advantages over other models in adoption of HIT on a national scale.
A few aspects of the experience in Taiwanese provide some indications, however, on how to succeed with the adoption of HIT on a large scale using other models. One important feature is that success in Taiwan has come with a system that involves both public and private health providers. Another important issue is how the adoption of HIT on a national scale in Taiwan was supported heavily by the implementation of an e-claims system to support administration of the national health insurance. The implementation of the e-claims system made it easier to promote the adoption of EMR systems, computerized decision support systems, and computerized physician order entry systems in the future and is being used to improve meaningful use of data generated at clinics and hospitals.
These issues clarify how it may not be necessary to organize healthcare delivery so it is conducted by a single integrated organization in order to successfully adopt integrated and large-scale HIT systems. Instead, it is the economic integration of different elements of healthcare that seems to be more significant in removing barriers in the adoption of HIT on a large scale.
This is supported by other evidence. Israel, for example, is quite far along in the adoption of HIT and is noted for having an efficient and high-quality universal healthcare system. Its healthcare system consists of four separate health maintenance organizations (HMOs), and the government pays the membership fee for citizens to the HMO of their choice. 22 It has been reported how one of these HMOs was able to successfully overcome barriers related to the adoption of EMR systems on a wide scale more easily than would be the case with a more fragmented healthcare delivery model. 4 In the United States, there are also a few “islands” where HIT use is highly successful, and these islands tend to be organizations such as HMOs (e.g., Kaiser Permanente, Massachusetts General Hospital, Boston's Beth Israel, and Brigham and Women's Hospital) that are economically integrated.
The Taiwanese experience thus suggests that organizing healthcare delivery to achieve economic integration can provide long-term advantages by making the adoption of large-scale HIT more possible. This could be accomplished through other mechanisms rather than the creation of a national single-payer system. One strategy, for example, could be to enable the development of universal healthcare based on HMOs supported by HIT, as has occurred in Israel, and another could be to develop single-payer systems at the state level, similar to recent efforts in Vermont. 23,24
Another lesson that can be taken from the Taiwanese experience is that it demonstrates how a strategic focus on support for electronic administration, and specifically e-claims, can be used to further national-scale HIT systems more generally. The connection between the adoption of e-claims and other HIT systems is sometimes not mentioned, and thus the possibility for e-claims to indirectly lead to greater benefits than only administrative efficiency may be overlooked. 2 An overview of how different countries have approached the implementation of national-level electronic health record systems has identified several challenges such as “acceptance and change management,” “basic legal conditions and data protection,” “project management,” “funding,” and “health policy-related goals and implementation strategy.” 5 These issues are important for any national-level HIT system, so experience in implementing an e-claims system nationally can provide stakeholders with experience on these issues while dealing with a system that is less technically complex and generally more homogeneous (i.e., similar usage at each site) than electronic health record systems.
The benefits of focusing on e-claims systems is interesting when considering that research efforts are less focused on e-claims. The terms “electronic claims” (110 hits) and “e-claims” (10 hits) in PubMed return a total of only 120 hits, whereas the terms “electronic medical records” (2,130 hits) and “electronic health records” (3,702 hits) return a total of 5,832 hits. It is important to note that the Affordable Healthcare Act does mandate the adoption of e-claims. 25 This has the potential to provide additional benefits in the future beyond just direct administrative efficiency. It is noted that additional efforts are still needed beyond that in the legislation in order to optimize the gains from e-claims, and suggestions have been made for “…the government to lay out a set of milestones and a path for meeting them, as it has sought to do with electronic medical records.” 26
Conclusions
The experience of a national-scale HIT system in Taiwan provides an example of how HIT can be used to support an efficient and high-quality universal healthcare system. Economic integration (through a single-payer system) is an important feature of the healthcare system that has enabled the widespread adoption of HIT in Taiwan. The adoption of a national-scale e-claims system by the BNHI has proved to be a critical step in the overall development of the national-scale HIT system infrastructure. Researchers and policy makers should thus increase their focus on supporting the adoption of e-claims and making meaningful use of claimed data for public health initiatives.
National healthcare systems and other large-scale healthcare organizations may thus benefit if they view HIT as a “standard” component of healthcare delivery and take sustained efforts over the long term to continually develop and improve their HIT systems. This can lead to incremental benefits as HIT systems continuously evolve and improve over time.
Footnotes
Disclosure Statement
No competing financial interests exist.