
Abstract
Introduction
The rising prevalence of overweight and obesity in pediatric populations is a major concern. 1 Globally, the estimated 155 million school-aged children who are overweight or obese represent a 47% increase between 1980 and 2013. 2 Pediatric obesity has a high prevalence among young people living in Australia, with more than 23% of boys and girls being overweight or obese. 2 In the United States, the prevalence of overweight or obesity in young people 2–19 years of age, independent of race and gender, is 32%, 3 and in England, the prevalence is 28% in both boys and girls. 4 Despite national health priorities to limit risks associated with obesity, the success and sustainability of weight management interventions in children and adolescents can be questioned.
Indeed, the potential health consequences of lifestyle changes in young populations with overweight or obesity are well established (i.e., body composition and cardiometabolic markers), but treatments effects are modest, and sustainability has not been extensively researched. 5 Calls for the management of child and adolescent overweight or obesity are urgent and frequent. Being overweight or obese not only leads to physiological and subsequently long-term medical complications, but it also influences social and emotional environments (e.g., stigmatization). 6,7 Initiating and maintaining changes through lifestyle interventions, in order to prevent overweight and obesity progressing into adulthood, are major challenges, and not every trial is successful in improving and sustaining energy balance and positive thinking. 8
The decline of physical activity during adolescence occurs globally, 9 –11 and traditional approaches to weight management (information and advice) largely remain ineffective. Multidisciplinary approaches focusing on behavioral change techniques appear to be a suitable option. Specifically, recently more promising management of body weight occurred when behavioral lifestyle interventions replaced standard care. 5 Understanding the barriers, enablers, and capacity of children and adolescents to cope with lifestyle changes and potential relapse are part of challenges associated with behavioral change targeted in multidisciplinary interventions. When young people make their own choices (self-determination), they feel in control. In a well-managed or controlled state of mindfulness, positive behavioral, cognitive, and psychological outcomes are possible. Exercise and other lifestyle changes can exemplify positive self-determination when children and adolescents are given choices, but when plans are imposed without consultation or choice, feelings of ill-being or dropout may result. Social media offers a vehicle of choice and self-determination for many young people. 12 Access to increasing advances in electronic social media may provide significant support for lifestyle changes. 13
Beyond the global health concern is the fact that overweight and obesity are an economic burden. To minimize costs and maintain limited resources, challenging interventions have been developed. Studies focusing on mobile phone interventions to reduce less desirable lifestyle practices and prevent overweight and obesity are gathering interest. Approximately 95% of countries worldwide have mobile phone networks, and most of them have more mobile phone than landline subscriptions. 14 Despite the fact that smartphones are included in campaigns to limit sedentary behavior associated with excessive electronic screen use, their popularity among the young population could be beneficial if used innovatively. Indeed, since the last systematic review on the effectiveness of weight management strategies for children and adolescents was conducted in 2009, 5 ownership of mobile phone has almost doubled, reaching 90% among Australian adolescents, 15 with 69% of them owning a smartphone. 16 Smartphone ownership is greater among Australian adolescents (69%) than among American adolescents (37%), and using a mobile device to access the Internet is also higher among adolescents from Australia (56%) than the United States (49%). 17 Data from younger children in Australia specifically show that mobile phone ownership has almost doubled between 2007 to 2013, reaching 35%. 18
More than becoming an integral part of adolescents' lives, being connected to the world is also a central behavior in social connection. In Australia, 9 in 10 adolescents have Internet at home, and 72% go online more than once a day for an average of half an hour. 16 When they are connected, data tracking shows they spend most of their time interacting with others and communicating with peers.
Unlike traditional cell phones, smartphones merge the previous differences between mobile phones and computers. Indeed, smartphones have advanced connectivity and computing capability. Smartphones can run software applications, commonly termed “apps.” 19 Recent years have seen a boom in self-management using e-health apps (i.e., fitness, well-being, nutrition). Adolescents in Australia reached a downloading rate for smartphone apps of 79% in December 2013 (games, 66%; social networking, 59%; education, 33%; and sport-related material, 27%). 16 Within a more specific context, e-health apps have the potential to improve the convenience and speed of delivery of care to its users. Because of the ability to deliver immediate contact or resources anywhere and anytime to their users, smartphone technology currently compares favorably with computers, which are seen as the “gold” proximity device.
Emergence of apps has given opportunities to healthcare industries to improve clinical communication as well as patients' information. 20 E-health apps have established some capacity for healthcare improvement. This two-way interactive communication allows individuals to select and self-monitor healthcare delivery. 14 By adapting face-to-face overweight and obesity treatment, smartphone interventions have the potential to encourage small, but significant, health behavioral changes. 21 The multimodal and interactive nature of Web-based technologies, including smartphone applications, can capture personal relevance and motivation via broad opportunities for feedback, offer individual choices for learning and literacy styles, and provide a diversity of interactive components capable of matching specific behavioral change goals. 22
This systematic review provides a comparative evaluation of the effectiveness of smartphones in multidisciplinary treatment of childhood obesity in the last 5 years, with a specific interest in behavior change.
Materials and Methods
Eligibility Criteria
The review sought to identify randomized controlled trials (RCTs) examining the relationship between smartphone technology and behavioral change to treat overweight and obesity in children and adolescents. Trial participants needed to be between 7 and 17 years of age and be overweight or obese. Trials were eligible for inclusion when targeting combinations of behavioral change using smartphone technology, plus nutrition and/or physical activity (apps, short message service [SMS], or e-mail), to treat and or manage overweight and obesity. Trials were excluded if they were related to overweight or obesity prevention, surgical intervention, pharmacology, genetic rather than lifestyle-related obesity, supplementation, if the trial referred to obesity as a secondary outcome (e.g., trials targeting diabetes), or if the publication was a trial protocol rather than an outcome publication.
Information Sources
Studies were identified by searching electronic databases and related article reference lists. The search was applied to Medline complete, OVID, CINAHL, EMBASE, and PubMed. The last search was conducted on August 2014. The search was developed as a collective effort of the research team and the collaboration of a librarian from the Australian Catholic University, Melbourne. There was no necessity to contact trial investigators or sponsors to acquire any information missing from the published article.
Search Strategy
To remain current, searches using Medline complete, OVID, CINAHL, EMBASE, and PubMed were limited to publications from 2009 to mid-2014, without any language restrictions and using the following terms to denote obesity (“obesity” OR “pediatric obesity” OR “obesity, abdominal”; “obesity” OR “obese” OR “overweight” OR “over-weight”), childhood (“adolescent” OR “adolescent behaviour”; “adolescen*” OR “teen*” OR “youth”), or treatment (“treatment outcome” OR “treatment failure”; “treatment” OR “outcome” OR “intervention” OR “lifestyle” OR “life style” OR “behavio*”) in articles with the study design limitation of “randomized controlled trial.”
Study Selection
Two reviewers (E.C. and G.N.) developed the review protocol, determined inclusion and exclusion criteria, and assessed potential articles for inclusion into the review. Retrieved abstracts were independently assessed to be eligible for inclusion by these two reviewers. Any disagreements on inclusions were resolved through discussions among three reviewers (E.C., G.N., and D.G.).
Study Quality Scale
Multiple scales are available to assess the quality of clinical trials. We selected the “PEDro scale” 23 to rate the methodological quality of the RCTs. We decided to use PEDro scale as it contained all the items from an original Delphi list 24 obtained from experts who reached a consensus on the most rigorous criteria to assess the characteristics related to the reporting of trial quality. Moreover, the PEDro scale includes two additional items from the original list of nine items that provide more information about the quality of reporting sustainability of participants and statistical comparisons. The “PEDro scale” comprises 11 items, and items are scored as either present (1) or absent (0). Higher scores are denoted by a higher quality of trial Specifically, a score of 9–10 is considered “excellent” quality reporting, 6–8 represents “good” quality reporting. and a score of 4–5 is considered to be only “fair” quality reporting. By using this scale we assessed the following items: disclosure of eligibility criteria, randomization procedures, concealed allocation, similarity of groups at baseline, blinding of subjects, trainer blinding, investigator blinding, reporting of less than 15% dropout, intention-to-treat analysis, between-group statistical comparison for at least one key outcome and point, and the reporting of variability measures.
Results
Study Inclusion/Exclusion
Articles were extracted and imported to reference manager software (EndNote; Thompson Reuters, San Francisco, CA). The process for trial inclusion is shown in Figure 1. The initial search strategy yielded a total of 548 references after the duplicates were removed. Titles and abstracts of potentially relevant articles were screened, and 517 articles were excluded. Full-text copies were obtained for 31 articles, with seven studies matched the inclusion criteria. Reference lists from the obtained articles were scanned for additional relevant articles. The main reasons for trial exclusion among the remaining 31 trials were (1) prevention rather than treatment designs (n=16), (2) conference abstracts rather than full articles (n=7), (3) computer software devices rather than more specific smartphone technology in the trial (n=2), (4) qualitative rather than quantitative analysis (n=2), and (5) nonrandomized pilot trials rather than RCTs (n=1). We chose to not include conference abstracts as they did not provide sufficient information about the trial's methodology. All the eligible seven trials stemmed from only two large RCTs extensively published in the last 5 years: “The Loozit® study” (n=5 publications) 25 –29 and “The SMSMT (SMS Management Technics) study” (n=2 publications). 30,31 To avoid duplication of data, we included only one RCT from each of the two large trials; the publication selected from these large trials was the one that most closely described the effectiveness of smartphone technology for promoting health-related outcomes.
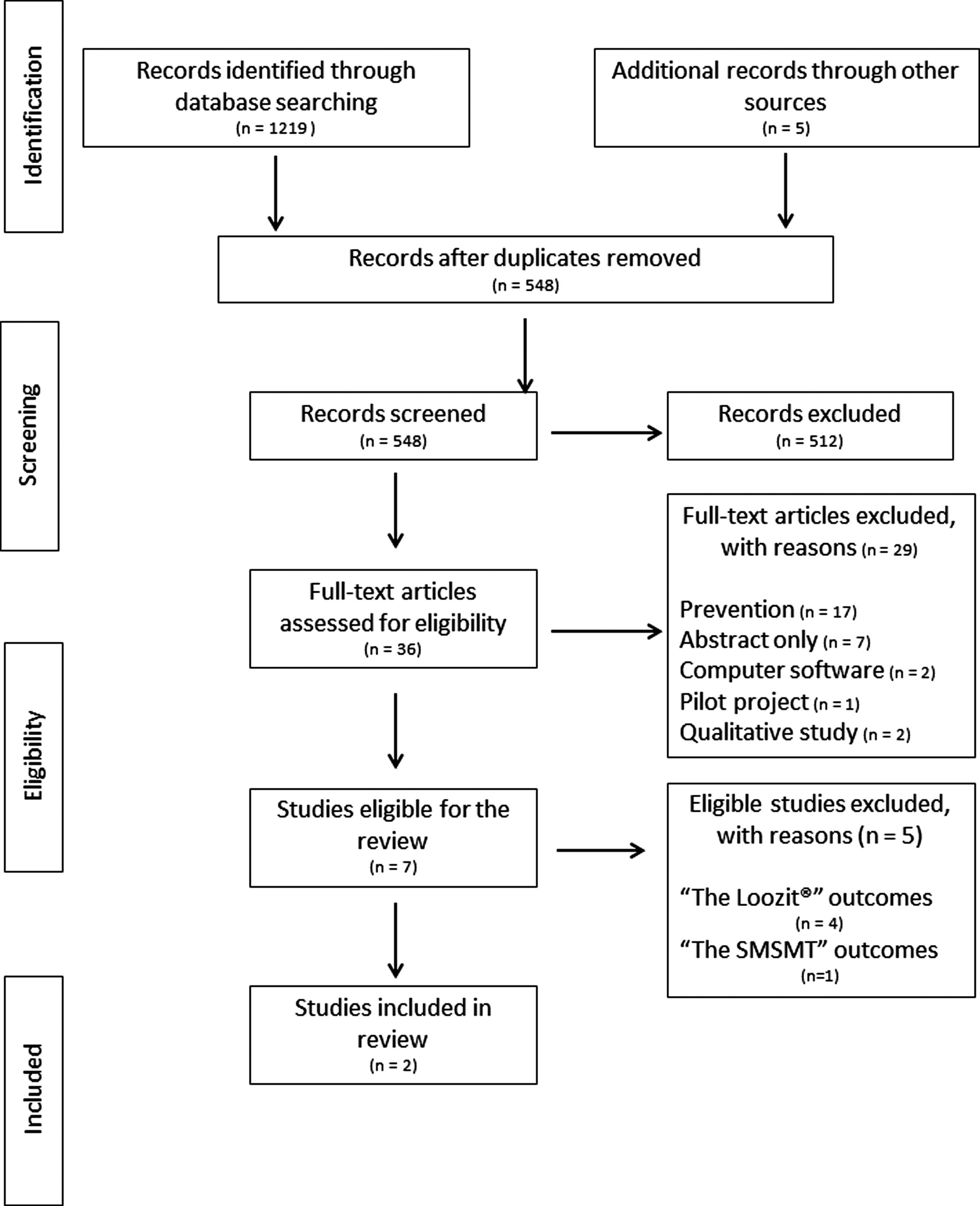
Study inclusion flow diagram.
Study Quality/Bias Risk
The study design quality is presented in Table 1. Because The Loozit study protocol was described elsewhere, 32 the article by Kornman et al. 29 did not give precise information about design details. This necessitated reference to the previously published protocol article in order to complete PEDro scale criteria 1–3 and 5–7. As previously described, both trials used randomization, but only assessors in The Loozit study were completely blinded to the groups. The two trials shared a percentage dropout rate of less than 15% for the electronic arm of the intervention. Furthermore, both trials provided measures of variability and the magnitude of differences, resulting in the reporting of statistical differences between groups. Overall, the Loozit study had slightly higher quality of reporting with a PEDro scale score of 7, whereas the SMSMT study had a PEDro scale score of 6. However, both studies were considered as “good” quality as their PEDro score was between 6 and 8.
Study Design Quality
1 point=•.
From The Loozit study. 32
Electronic contact group only.
SD, standard deviation.
Study Interventions
Details from the trial interventions are reported in Tables 2 and 3. Primary eligibility criteria in both studies centered on children or adolescents who were overweight or obese. These two studies 29,31 collectively included 190 overweight or obese children and adolescents, between 7 to 16 years of age. In the trial from The Netherlands, 31 the mean age at baseline was 9.9 years, and the body mass index (BMI) [mean (standard deviation [SD])] was 2.60 (0.4). In the Australian trial, 29 the participants were slightly older (14.6 years) with a BMI z-score of 2.03 (0.37). The main exclusion criteria described in the publications were related to behavioral problems, overweight or obesity as a secondary cause, the use of medication known to alter metabolism and/or exercise responses, participants with an intellectual disability, participants with a poor level of language spoken, an inability to practice physical activity, and/or an expressed lack of motivation to commit to trial demands. As both studies required mobile phone usage, participants either received a mobile phone 31 or used their own for the duration of the intervention. 29
Participants' Characteristics and Study Interventions
BMI, body mass index; SDS, standard deviation score; SMS, short message service.
Studies, Interventions, and Outcomes
Arrows indicate the following:  =higher,
=higher,  =lower, and ↓=decrease.
=lower, and ↓=decrease.
BMI, body mass index; e-contact, electronic contact; e-intervention, electronic intervention; msg, message; SD, standard deviation; SMS, short message service; Ø, no effect/no changes.
Both studies had an intensive phase intervention with a duration of between 229 to 331 months, followed by a maintenance phase lasting from 10 to 9 months, respectively. Again, both studies delivered intensive phases that focused on behavioral change with a multidisciplinary approach inclusive of physical activity, nutrition, and psychological support for the children and adolescents, as well as sessions for parents. During the maintenance phase, both studies reported between-group comparisons, related to the impact of receiving electronic contact (e-contact). However, control group and e-contact group comparisons were only conducted in the SMSMT study. 31 The other trial 29 compared the results of the e-contact with a group who also received the lifestyle intervention.
The maintenance phase of the e-contact group in the SMSMT study 31 can be considered as an “active” phase. Indeed, during this period, participants were asked to send weekly SMS texts relating to their physical activity, nutrition practices, and feelings of happiness. Moreover, they were encouraged to contact researchers any time they wanted to communicate about life events, feelings, and other thoughts. In return, supporting and encouraging SMS texts personalized for each individual were sent by researchers within 2 days, followed by a reminder after a week without response. Personalization of feedback messages consisted of participants' personal information (i.e., participant's first name, personal goals, personal difficulties, content of previous messages). In addition, both the non–e-contact and the e-contact groups and their parents attended collective and individual “booster” sessions with researchers at 6, 9, and 12 months.
During the maintenance phase of the Loozit study, 29 the non–e-contact group received “booster” sessions once every 3 months, whereas the e-contact group had “semipassive” electronic contact. Semipersonalized SMS texts and/or e-mails were sent to participants monthly or fortnightly during school holidays. Specifically, the semipersonalized aspect of the messages consisted of incorporating the child's or adolescent's first name. E-messages were based on the reinforcement of the key lifestyle principles (i.e., being active, healthy eating, goal setting, self-esteem, and stress management) and finished either with a statement or with an invitation to reply.
Study Outcomes
Study outcomes are summarized in Table 2. Data were collected at baseline, at the end of the intensive phase, and at 12 months. 29,31 Compared with baseline values, the effect of the intervention on BMI z-scores showed significant decreases after 12 months in one trial 31 and a moderate decrease after the intensive phase in the other. 29 However, no additional BMI changes were reported following the electronic intervention phase, 31 nor was there any association of BMI changes with the number of messages sent.
Nevertheless, the effect of e-contact on participants' engagement patterns highlighted better compliance during the first 3 months of the maintenance phase, 31 and e-mail responses included more words than SMS texts but also registered a longer response time. 29 Only 32% of participants responded when an invitation to reply was added to the message, with the majority of responses related to healthy eating. 29 Another positive outcome was shared by both studies reporting a lower percentage of dropout in the e-contact group compared with the non–e-contact group (respectively, 12% 29 and 14% 31 ). Moreover, dropping out was 3.25 times less frequent when participants received e-contact during the maintenance phase. 31
Discussion
As mobile phones may be seen as the primary mode of communication worldwide, smartphones can become an integral part of the users' life. Smartphones allow users to accomplish tasks anywhere and anytime they desire. Furthermore, they offer researchers additional capacity to track the effectiveness of electronically generated health promotion strategies that target specific risk factors and behaviors. 33
Currently, there is less evidence on the use of electronic devices in pediatric obesity treatment compared with their use in prevention trials. Among the few specific overweight and obesity management trials, multidisciplinary interventions have been conducted mainly using mobile phones or computer-based support. 31,32,34 –36 Results from the limited evidence suggest the insufficiency of e-contact in significantly reducing body weight. However, the strategy of using e-contact with adolescents should not be dismissed because of the capacity to prolong engagement and decrease withdrawal during critical maintenance phases. Therefore, in studies targeting strong maintenance in children and adolescent weight management, it may be a successful strategy.
RCT protocols on childhood overweight and obesity treatment using smartphone are emerging. 37 However, protocol publications typically precede interventions, and the publication of the outcomes detailing the effectiveness of the trials occurs only after short- and sometimes long-term results have been obtained. Therefore, in just a few years, more will be known about the effectiveness of smartphone technology in assisting weight management for overweight or obese young people. Based often on the transtheoretical model and social cognitive theory, multidisciplinary interventions are combining nutrition, physical activity, and psychological support and proposing to assess the effectiveness of such strategies (smartphone apps) in reducing or at least managing overweight and obesity. The capacity of smartphone apps to match the diversity of goal setting behavior inherent in individuals belonging to a group supports the role of self-determination and respects the need to conduct this behavior at the time and pace selected by the individual.
Although limited in number, the results available from outcome trials for this systematic review reinforced findings from computer-based studies treating 34 or preventing 38 overweight and obesity and other overweight and obesity prevention trials in adolescent girls 39 and boys. 40 However, health facilitator technology programs appeared not to influence anthropometric outcomes changes, even if they have the capacity to reduce sedentary time (i.e., screen-time). The role of e-contact as a facilitator may best lie in supporting or initiating health-related behavior changes that may sometimes be readily forgotten or poorly prioritized.
Smartphone technology may therefore offer a useful strategy in supporting overweight and obesity management behaviors. Indeed, the readily obtainable smartphone technology can have a major role in the prompting processes required to develop new strategies to manage overweight and obesity. Accessibility, feasibility, and attractiveness of smartphone technology have supported a rising interest in providing e-health information. 13 Smartphones increase realistic opportunities to adapt and deliver personalized messages targeting its users. Text messages and/or “apps” have the potential to create virtual interchange and support, helping owners to adopt lifestyle changes through implementation and reinforcement of behavior change (i.e., goal setting, self-modeling, and environmental restructuring 41 ). However, as previously stated, e-contact is only one part of a multicomponent program and appears to have promising use following intensive phases of weight management interventions. The capacity of e-contact for providing children and adolescents with personalized self-determination skills and feedback, extrinsic initiators, or reminders about goal-setting behavior support for relapses in management, as well as generous flexibility of how the contact is selected, received, and responded to, is yet to be explored in child and adolescent weight management.
Limitations should be considered when interpreting the results of this review. First, the data available to examine the effectiveness of smartphone technology in pediatric overweight and obesity treatment are limited. Results from only two RCTs were available to demonstrate the effectiveness of using a smartphone in children and adolescent weight management. The lack of substantial evidence renders the findings equivocal.
It is worth noting that studies using smartphone technology in overweight and obesity treatment are currently an emerging interest; to our knowledge, none has fully detailed the methods involving behavioral change techniques within existing devices. This is a notable omission as failure to identify behavioral change techniques limits internal and external validity of much-needed interventions. 42 Given the necessary focus on behavioral change in the management of adolescent obesity, further investigations documenting behavior change responses delivered with support of e-contact during maintenance phases of long-term weight management interventions may add urgently required relevance for this highly vulnerable population.
Footnotes
Acknowledgments
The authors would like to acknowledge Kathryn Duncan for her valuable help and contribution to the literature search strategy.
Disclosure Statement
No competing financial interests exist.