
Abstract
Introduction
Dermatology divisions at the Veterans Health Administration (VHA) experience high demand. During the last 15 years, as telehealth has increasingly become an integral part of healthcare delivery in the VHA, the VHA has developed one of the largest teledermatology programs in the United States, serving 505 Veterans Administration (VA) Medical Centers and community-based outpatient clinics. With the passage in August 2014 of the Veterans Access Choice and Accountability Act, which directs VHA to provide healthcare within 40 miles of every enrolled veteran residing in the United States and its territories, telehealth strategies to increase veterans' access to dermatologic care will likely increase further in importance.
Having previously recognized that telehealth allows providers to bridge obstacles to care caused by distance, local teledermatology pilot programs began within the VHA as early as 1999. The federal nature of the VHA healthcare system facilitated this development because American state licensure and malpractice limitations do not apply to VA physicians and patients—for example, in one of the first programs, dermatologists practicing in Rhode Island, at the Providence VA Medical Center, began to perform teledermatology consultations for veterans in Maine, at the Togus VA Medical Center. By 2003, the VHA established a national Office of Telehealth Services and in the following years developed national support systems to support local innovators. By 2011, the VHA evolved a national infrastructure designed to expand telehealth use to a majority of clinicians in critical areas of healthcare delivery; in 2012, it created a standardized national teledermatology program. 1
VHA currently uses two modes of teledermatology: clinical video telehealth (CVT), in which a live interaction between the patient and the physician occurs although at different locations, and store-and-forward telehealth (SFT), which differs from CVT in that the encounter occurs at different times (the patient's history and images are posted hours to days before the provider evaluates them). We describe this program using routinely collected administrative data.
Materials and Methods
The VHA healthcare system is the largest integrated healthcare system in the United States, with more than 1,700 patient care sites and 152 medical centers; these medical centers and their associated care sites are grouped into 21 geographical regions called Veterans Integrated Services Networks (VISNs) (
Results
Teledermatology Subtypes
In FY 2014 the VHA used CVT in 8 VISNs and SFT in all 21 VISNs. National trends show decreasing use of CVT and rapidly increasing use of SFT over the past decade (Fig. 1).

Teledermatology by clinical video telehealth (CVT) versus store-and forward telehealth (SFT) encounters by half year, 2002–2014. FY, fiscal year.
Patient and Visn Numbers
From 2002 to March 2014, the VHA recorded 4,110,649 telehealth encounters, of which 6%, or 234,928, were teledermatology. For the first half of FY 2014, the VHA recorded 492,882 telehealth encounters, of which 7%, or 31,926, were teledermatology. The first half of FY 2014 represents 14% of all teledermatology visits recorded in the VHA since FY 2002. FY 2013, with 53,197 encounters, represents 23% of all teledermatology encounters recorded since FY 2002. These numbers indicate the rapid growth of teledermatology within the VHA.
All 21 VISNs used teledermatology in the first half of FY 2014, but the VISNs varied in the number of encounters, with 4 VISNs collectively reporting 51% of the patient encounters. VISN 8, which serves Florida, Puerto Rico, and the Virgin Islands, reported the highest number of patient encounters (5,237), with 16% of the total. VISN 11, serving Michigan, Indiana, and Illinois, reported 13% of the total (4,132 encounters). VISN 7, serving Alabama, Georgia, and South Carolina, and VISN 20, serving Alaska, Idaho, Oregon, and Washington, each reported 11% of the total (3,588 and 3,505 encounters, respectively) (Figs. 2 and 3).
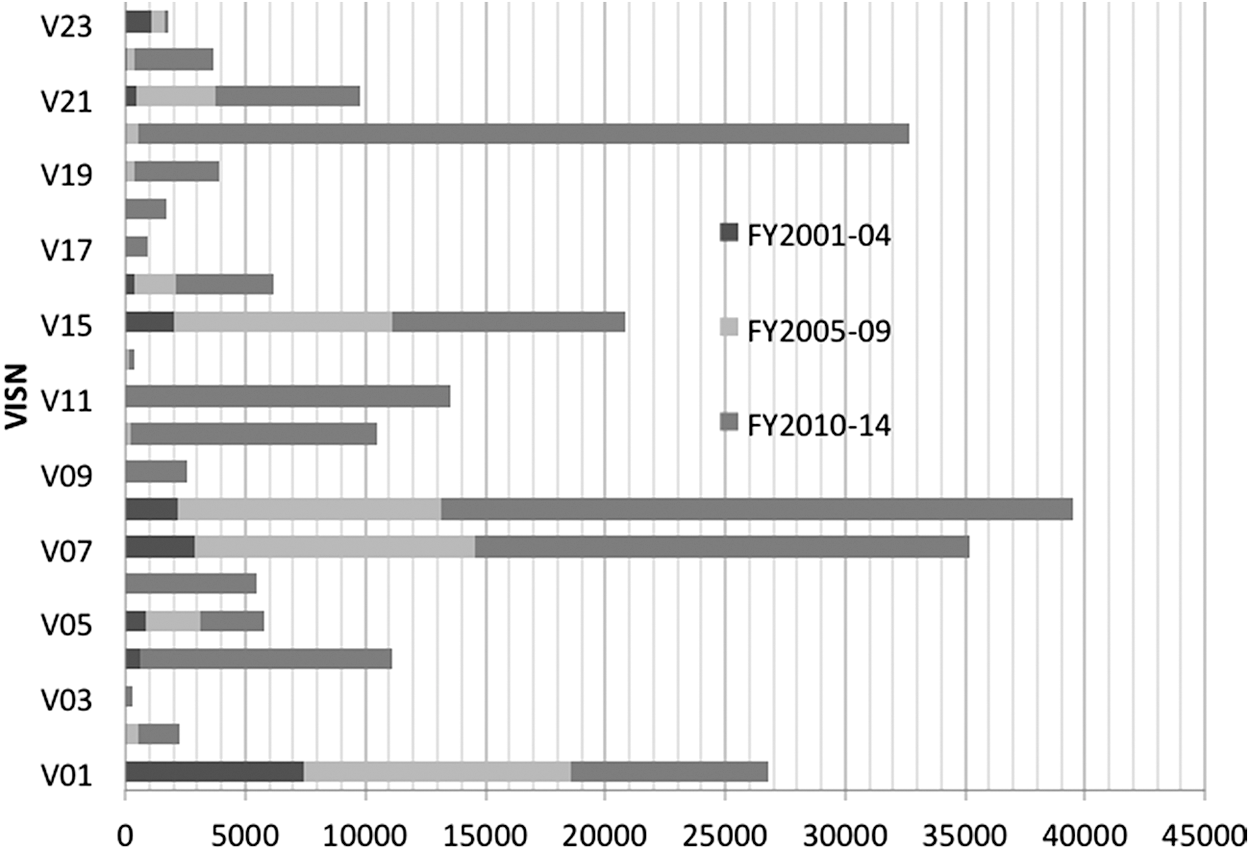
Teledermatology store-and-forward telehealth encounters by Veterans Integrated Services Network (VISN) and fiscal year (FY), 2002–2014.
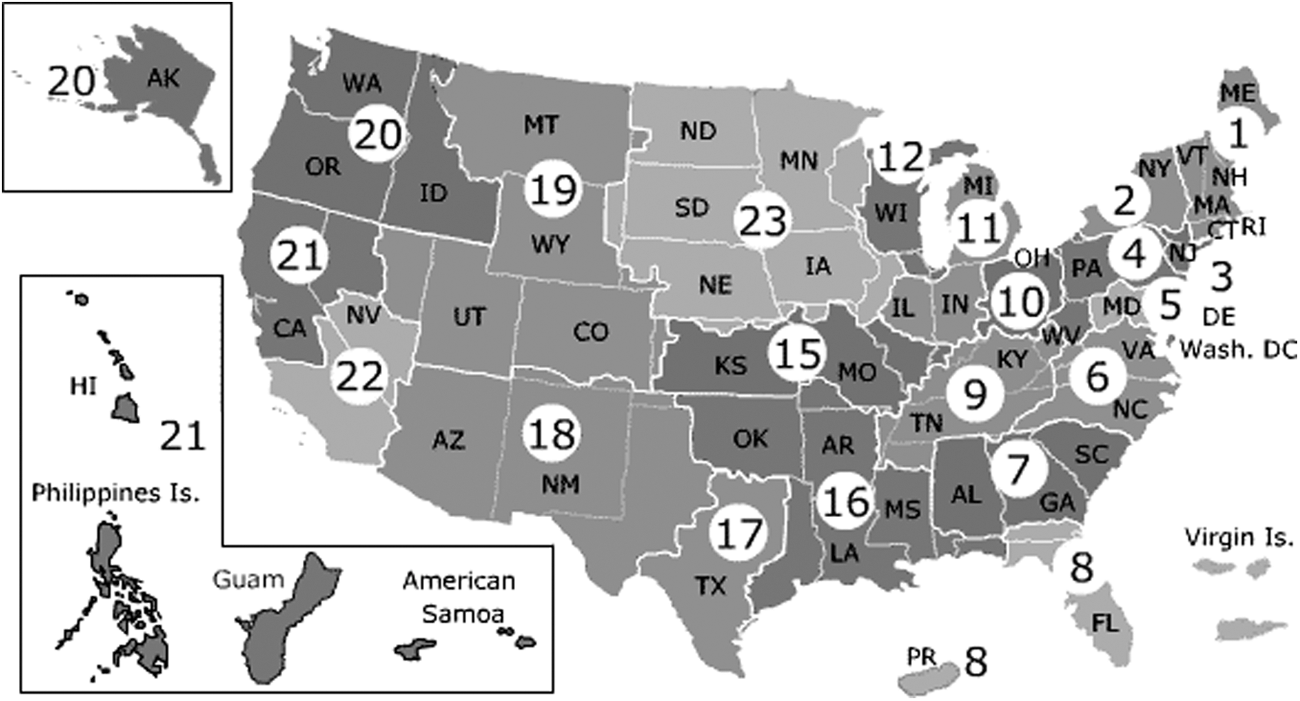
Veterans Integrated Services Networks of the Veterans Health Administration (
Patient Demographics
The VHA defines “urban” and “rural” according to the U.S. Census definitions, “highly rural” as any area within a county with fewer than 7 civilians per square mile, and “unknown” when it lacks a valid, geomapped address for the veteran. In 2007, when the VHA first recorded information about degree of rurality for those using teledermatology, most patient encounters were for veterans living in rural areas. Starting in 2012, encounters for patients in urban areas exceeded those in rural areas (Fig. 4).
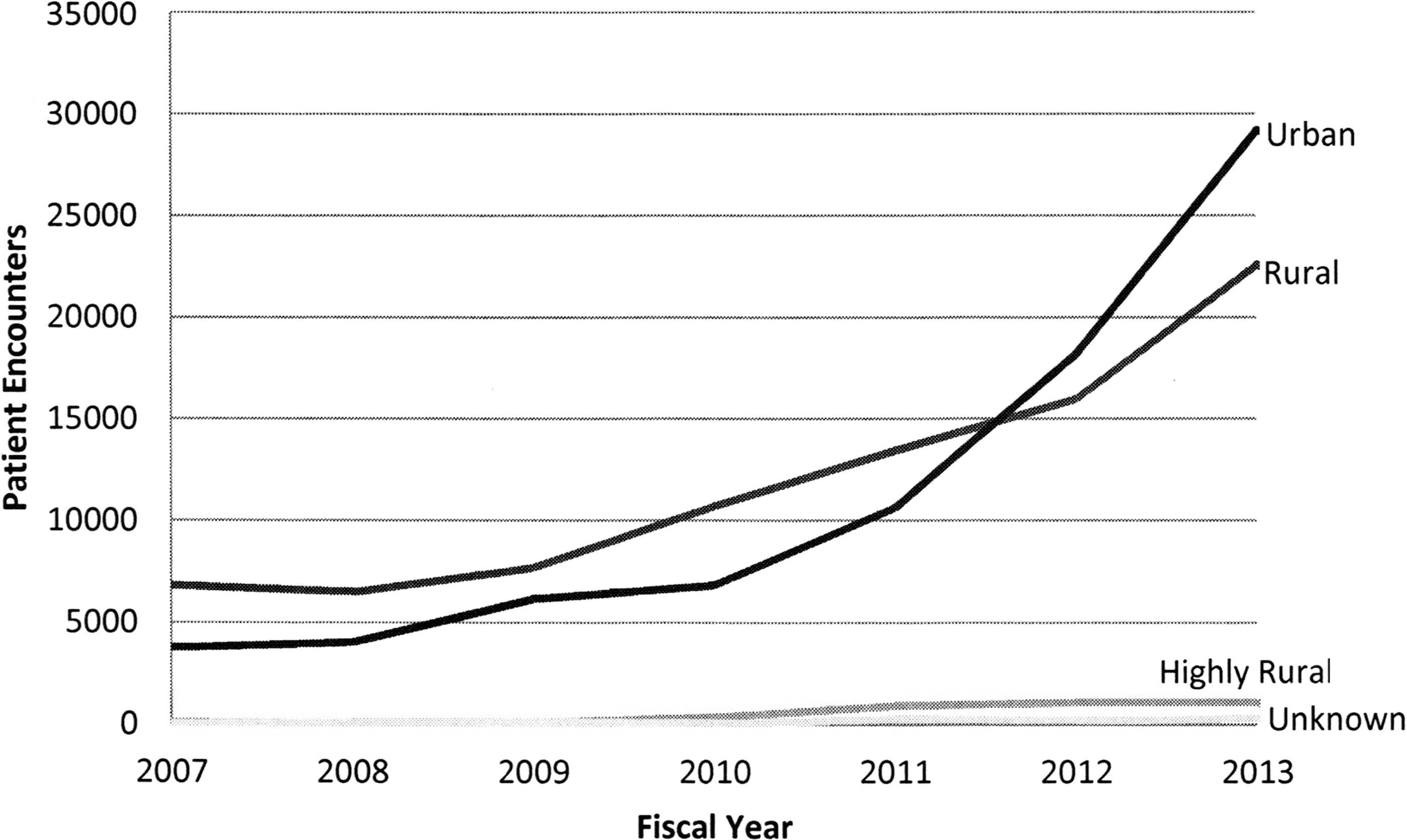
Dermatology encounters by patient demographics by fiscal year.
In FY 2014, by far the largest users of teledermatology were veterans of the Vietnam era: 18,454 patients 60–69 years of age represented 40% of the total. The next largest group was veterans 70–79 years of age, with 7,866 and 17% of the total. Fifteen percent of the total encounters were for patients 49 years of age and younger, and 12% were for those 80 years of age and older. Ninety-three percent of all teledermatology encounters in FY 2014 were with male veterans compared with 95% in FY 2002.
Time to Consult Completion
VHA teledermatology defines a 7-day turnaround time as a condition of participation. Nationally, 71% of SFT encounters for the first half of 2014 and 65% of all SFT encounters since 2002 were completed within 7 days of referral. These numbers show modest improvement in speed of consult completion since the program's inception. They also show a vastly decreased wait time for patients seeking dermatology consultations compared with the usual experience of patients in the United States, for whom several studies have shown it can take more than a month to obtain a dermatology appointment. 2,3
Discussion
With the exception of the review by Armstrong et al. 4 of American teledermatology programs, this report is the first to describe the VHA's teledermatology program. The article by Armstrong et al. used survey methods to describe the range and extent of programs within the United States; hence it was limited by the response rate and possible inaccuracies in responses received. Because we were able to use VHA data from routinely collected patient encounters, we could describe the program with greater precision.
The data show a SFT teledermatology program within the VHA as rapidly expanding in recent years due to institutional support. The expansion has been facilitated by systematic initiatives in telehealth overall and in teledermatology specifically. These initiatives included creating incentives in the form of performance measures for telehealth adoption, as well as providing the resources to do so, including hiring 1,150 telehealth technicians so that every VA Medical Center would have two and every community-based outpatient center one trained imager by 2012. Additionally, VA implemented a standardized and rigorous training curriculum for teledermatology imaging that has recently leveraged online and video technologies to enable large numbers of imagers to acquire necessary skills. VHA has furthermore created a standardized operation manual and templates for SFT teledermatology for each user in the process (referring provider, imager, and teledermatology reader). Equally important is that its quality management requirement, known as Conditions of Participation, ensures that approved clinical, technical, and business standards apply to every VHA telehealth program. These standards increase the likelihood that teledermatology care is both high quality and sustainable.
Within this national framework, in which every VISN within the VHA now provides teledermatology consultations according to national standards, there is local variation. For example, dermoscopy use varies by program. Additionally, the extent that VISNs use teledermatology varies widely: the data show that one-half of the patient teledermatology encounters occurred in 4 of 21 VISNs. The reasons for local variation are beyond the scope of this report but may include factors such duration of program initiation and local infrastructure and policies.
It is notable that CVT use has been variably decreasing or stagnant since 2005. Due to its increased time efficiency for providers compared with CVT, SFT accounts for the rapid expansion of teledermatology programs. Also notable is that teledermatology, originally designed to serve rural patients, has since 2012 served more urban patients than rural. This change demonstrates that the existence of a national teledermatology program has expanded access for patients regardless of their physical location. That the majority of veteran users of teledermatology were 60–79 years of age (our data show that 57% of the total users in 2014 were of this age group) most likely reflects the demographics of enrolled veterans and is consistent with the notion that teledermatology is becoming increasingly integrated into the care of the average veteran.
Limitations
The accuracy of this report is limited by both potential data entry errors and evolving definitions. Coding and data entry errors would most likely lead to underestimation of encounters as well as overestimation of time to consult completion. The effect of other misclassification errors—such as recording the wrong type of patient location if the veteran had an incorrect address listed—is difficult to assess. In addition, although the VHA may have improved accounting accuracy over time as its coding of teledermatology encounters has evolved, these changes may distort the picture of teledermatology expansion.
Additionally, certain types of teledermatology encounters, such as same-facility teletriage and teledermatology for patients at non-VA sites, are located in a different database than the one described for this article. Because we cannot include every type of teledermatology practiced at the VHA via the Telehealth Workload Cube, there is some potential for inaccuracies in encounter numbers. For example, VISN 1, which serves the New England region, currently performs approximately the same number of teletriage encounters within its Providence facility as it does teledermatology for outside locations. 5 Because same-facility teledermatology and chart review “e-consultation” use identical codes, obtaining these teletriage numbers is beyond the scope of this article. Most likely, however, the number of teletriage and nursing home teledermatology practiced nationwide is so small that it minimally underestimates the VHA's national teledermatology impact.
Last, the Telehealth Workload Cube does not contain clinical or quality control data. As a result, a description of the diseases encountered, or the readability of the images, within the VHA teledermatology program lies beyond the scope of this article. Most likely the diseases seen by teledermatologists mirror the wide variety of inflammatory and neoplastic skin conditions, with regional variations, with which veterans present at the face-to-face dermatology clinics nationwide.
Conclusions
Despite the limitations, the data in this report demonstrate that the VHA is a major provider of teledermatology in the United States. Most likely the program has grown rapidly, not only due to the VA's widespread adoption of telehealth in general, but also because teledermatology, with its readily available standardized guidelines and tools and its facilitation of patient triage, 6 can be used to help address VA's dermatology access and workforce issues. Teledermatology is transforming the VHA's overall delivery of dermatologic care; as access measures inevitably move from “time to a dermatology visit” to “time to receipt of dermatologic care,” the implications of this transformation will become more apparent.
Footnotes
Acknowledgments
We thank the following for their assistance with this project: Ms. Kim Marcolivio, Dr. Kaveri Korgavkar, Mr. Junius Lewis, and Dr. Adam Darkins.
Disclosure Statement
No competing financial interests exist.