
Abstract
Introduction
Home-based telemental health (HBTMH) is the provision of mental healthcare services directly to the homes of patients with the use of communications technologies. The U.S. Veterans Health Administration has successfully implemented a national home telehealth program that included veterans with posttraumatic stress (PTS) disorder (PTSD), depression, and chronic medical conditions. 1 A HBTMH pilot program 2 and several clinical studies 3,4 have also demonstrated the benefits of home-based treatments for veterans. The potential benefits of HBTMH have also been recognized for some time within the U.S. Department of Defense. For example, a 2010 memorandum from the Chairman of the Joint Chiefs of Staff advocated that the military health system's model of care “…must deliver options for mental health services in the comfort and security of the Service member's own home….” 5 Service members who are living in geographically remote locations or in areas that have a shortage of specialty healthcare professionals may especially benefit from HBTMH options. Moreover, some service members may be drawn to HBTMH because of the privacy it offers to those who are concerned about stigma associated with seeking mental health treatment. Despite the call for home-based care within the U.S. Department of Defense, and the benefits it may offer, the military health system has not established the necessary policies and pathways for a HBTMH model of care to occur.
The U.S. military has unique network and data security requirements compared with other settings as well as specific protocols and procedures for care that have not yet been tested for HBTMH. Although the existing empirical literature provides initial support and guidance for the safe and effective use of home telehealth services for appropriate populations, 6,7 there remains a need to demonstrate that home-based care is technically feasible, safe, and effective and meets the military health system's standards of care before widespread implementation can be achieved. The purpose of the present study was therefore to evaluate the feasibility of providing a behavioral activation (BA) treatment for PTSD 8 delivered via synchronous (two-way) videoconferencing to the homes of U.S. military service members. BA is a well-established treatment for depression that counters patterns of avoidance and withdrawal with a pattern of engagement in valued activities through activity planning. 9 Given that avoidance and withdrawal processes also serve to maintain the symptoms of PTSD, BA has been evaluated as a treatment for PTSD. 8,10 –12 Although previous studies have examined military veterans, our study is the first to evaluate BA for PTS among active duty military members.
Materials and Methods
This study is an initial part of a multisite clinical trial that is comparing the effectiveness of BA for depression delivered in-office versus in the home. 13 Although the randomized clinical trial provides an opportunity to test the effectiveness of home-based BA for service members and veterans with depression, this evaluation allowed us to assess the feasibility of the technology, to examine safety management procedures, and to evaluate a promising treatment for PTSD. We predicted that the BA intervention would result in a reduction in PTS and depression symptoms. We also included measures of anxiety and sleep quality as exploratory outcomes. The procedures of this study adhere to the principles and recommendations of the World Medical Association and the Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects. This study was approved by the Madigan Army Medical Center Institutional Review Board and the U.S. Army Medical Research and Materiel Command's Human Research Protection Office.
Participants
The sample consisted of 10 active duty members of the U.S. Army. All participants were referred to the study from medical and behavioral health clinics at a large Army medical treatment facility. The study inclusion and exclusion criteria were determined by initial screening interview. To be eligible for the study, participants had to endorse experiencing at least one criterion A stressor and have a score of 45 or higher on the Clinician Administered PTSD Scale (CAPS). 14 The cutoff score of 45 has been used in other studies. 15 Participants taking any psychoactive medications had to have maintained a stable regimen for a minimum of 30 days prior to study entry.
Procedures
As part of the informed consent process, participants were provided with detailed information about how their identity and private health information would be protected, the limits of confidentiality, and the record keeping system used in the study. This included an overview of the telehealth equipment and instructions pertaining to setting up the treatment environment in a private area free from distractions. All participants completed a release of information form so that a contact person, of their choice, could assist in case of clinical emergency. The requirements and processes for engaging with third parties were disclosed and discussed during the informed consent process.
Study personnel
Treatment providers included five clinicians (four licensed psychologists and one postdoctoral fellow). The postdoctoral fellow was supervised on a weekly basis. All study providers participated in initial and annual BA training workshops.
Clinical assessment
PTS symptom severity assessments were completed by two independent, doctoral-level outcomes assessors. These assessors were trained in the administration of the CAPS and possessed prior experience with this measure. The CAPS, along with the self-report battery, was completed at the baseline, midtreatment, posttreatment, and 3-month posttreatment assessments. All assessments were video-recorded and reviewed regularly by a supervisory psychologist. Feedback was provided on an as needed basis to improve compliance with CAPS administration rules.
Treatment protocol
The intervention consisted of eight sessions of BA for PTS. The treatment protocol is adapted from a BA treatment manual 11 that has been expanded into an early intervention for PTSD and depression. 8 The protocol places a strong emphasis on an outside-in approach to behavior change whereby values-consistent activities are identified, planned, and tracked. The treatment is guided by behavioral theory, with functional behavioral analysis being a primary treatment component. 16
The primary tasks during the first two treatment sessions are (a) to provide psychoeducation about PTSD and the rationale for treatment, (b) to identify values, priorities, and treatment goals and to translate those into scheduled activities, and (c) to establish a pattern of daily monitoring and planning for activities. The goal of the remaining sessions is to support the ongoing implementation of BA strategies. During sessions 3–8, the treatment provider conducts functional analyses of avoidance behaviors that prevent participants from engaging in scheduled activities and reinforce progress towards goals. During sessions 7 and 8, the provider also discusses relapse prevention and encourages participants to use BA principles if/when symptoms return.
Telehealth procedures
All participants were issued a Dell (Round Rock, TX) M6500 laptop computer and a Tandberg (Oslo, Norway) Precision High Definition Webcam. Participants were also provided with a username and password for access to preloaded Jabber Video software (Cisco Systems, San Jose, CA). This software was selected because its level of security and encryption is approved for use by the U.S. Army. Prior to the first treatment session, a treatment station set-up appointment was scheduled between participant and treatment provider to familiarize participants with the equipment and the Jabber Video software and to test the network connection. Participants were required to use their home Wi-Fi or cable Internet connections to log-in for treatment sessions. Participants were instructed to initiate the Jabber Video connection with their assigned treatment provider at scheduled appointment times.
Some modifications to the original BA protocol were necessary in order to deliver the treatment remotely via telehealth technology. A treatment session checklist 12 was administered at the beginning of each session for the purpose of reminding study clinicians of procedures and for documenting patient safety and technical issues. Several modifications were also required for sharing homework and study handouts (BA worksheets, self-report questionnaires, etc.), such as use of screen shots of homework and handouts and holding handouts up to the camera.
Measures
The following measures were assessed: • Demographic questionnaire. Participants provided demographic information including occupation/work status/income/living situation, branch of service/highest rank, pain rating (0–10), and medications. • CAPS. The CAPS
14
is a structured interview that assesses all DSM-IV PTSD criteria in terms of frequency and intensity. The CAPS Current and Lifetime Version, which measures a 1-month symptom duration, was used for the baseline and follow-up assessments. The CAPS One Week Version, which measures symptoms over the past week, was used to assess participants after treatment sessions 4 and 8. PTSD severity, measured by the CAPS (total score), served as the primary PTSD outcome. • PTSD Checklist Military Version. The PTSD Checklist
17
is a self-report measure that evaluates all 17 DSM-IV PTSD symptoms across the three primary symptom clusters using a 5-point Likert scale. Internal consistency for the total score is high (0.97), as are reliability estimates (0.96). The PTSD Checklist Military Version (PCL-M) is used here. A total score of 50 typically serves as the threshold for identifying probable PTSD among those reporting military-related trauma(s). • Beck Depression Inventory-II. The Beck Depression Inventory-II
18
(BDI-II) is the most commonly used self-report measure of clinical depression severity. It consists of 21 items that are rated on a 4-point scale and that yield a range of scores from 0 to 63. • Beck Anxiety Inventory. The Beck Anxiety Inventory
19
(BAI) is a self-report measure consisting of 21 items designed to discriminate anxiety from depression. It has high internal consistency (0.92) and 1-week test–retest reliability (0.75) and discriminates anxious from nonanxious diagnostic groups.
20
• Pittsburgh Sleep Quality Index. The Pittsburgh Sleep Quality Index (PSQI)
21
is a 10-item measure of sleep quality. This measure assesses both the quality and quantity of an individual's sleep pattern over a 1-month period. Internal consistency for this measure has been found to be 0.80, with a reliability coefficient of 0.83 and test–retest reliability of 0.87.
22
• Safety measures. Safety data collected included any adverse events, psychiatric hospitalizations, suicides and nonfatal suicide-related behaviors, number of times the patient support person was utilized during treatment, treatment adherence, and frequency of requests for patient or therapist technical support. Safety-related data were recorded after each treatment session on the Treatment Session Checklist. We also followed the suicide assessment and risk management Standard Operating Procedure (SOP) used at Madigan Army Medical Center to assess and document suicide risk. The SOP requires clinicians to assess and document current ideation, presence of a plan, suicidal intent, history of previous attempts, and degree of impulsivity. Risk correlates (e.g., recent loss, financial problems), preparatory behavior (e.g., available means), and other risk factors (e.g., substance dependence) are also assessed and documented. The SOP was administered at the baseline assessment and the first treatment session and re-administered at each subsequent session if a patient endorsed current elevated risk per the SOP. • Treatment Session Checklist. The Treatment Session Checklist
13
is designed to collect information for the evaluation of clinical telehealth sessions. It is used to document safety information including current suicidal ideation, homicidal ideation, and other signs of risk (including the visual presence of a weapon at the patient's location). Clinical factors such as indicators of intoxication, disorientation, and severe emotion dysregulation are also included, as are questions related to the in-home environment, such as “Is anyone else at home today?” and “Do you feel that your environment is safe and private?” This checklist is also used to document telehealth equipment and connectivity status, adequate lighting, and any disruptions to session. • Client Satisfaction Questionnaire. The Client Satisfaction Questionnaire
23
is an eight-item self-report measure of general satisfaction with psychotherapeutic treatment. (The instrument is reproduced with permission of C. Clifford Attkisson.) Participants are asked to rate satisfaction on a 4-point scale, with a possible range of 8 to 32, with higher scores indicating greater satisfaction. Internal consistency and construct validity have been established, and the measure is widely used in research.
24
Results
All participants were men, between the ages of 21 and 45 years with a mean age of 31.8 (standard deviation [SD]=7.44) years. All were enlisted members of the U.S. Army with an average length of military service of 9.3 (SD=5.21) years. Five of the 10 participants reported having some college education, and 9 of the participants reported that they were currently married. Seven of the 10 participants resided in private housing off of the military installation.
Seven of the 10 participants had deployed to Iraq at least once in support of Operation Iraqi Freedom, and 6 had been deployed to Afghanistan in support of Operation Enduring Freedom. Two participants had also experienced other deployments. The number of deployments that any single participant reported ranged from one to four. All of the index traumas assessed on the CAPS were combat related and occurred during Operation Enduring Freedom/Operation Iraqi Freedom deployments. All of these traumatic events met DSM-IV criterion A for PTSD. On average, these traumas had occurred 6 (SD=3.33) years prior to the patient presenting for treatment. The span of time since trauma exposure ranged from 2 to 11 years.
Clinical Outcomes
We examined clinical treatment outcomes based on similar procedures used in a pilot study of BA for PTSD that was conducted with veterans. 11 Table 1 shows the results of paired-sample t tests (two-tailed) of clinical outcome measures and individual responses to the treatment. We calculated Hedge's g to represent effect size and used Cohen's definition 25 to interpret them. The criteria we used for reliable change was based off of previous research 11,26 and was as follows: CAPS,±9; PCL-M,±5; BDI-II,±5; BAI,±8; and PSQI,±2.
Treatment Clinical Outcomes
p<0.05.
BAI, Beck Anxiety Inventory; BDI-II, Beck Depression Inventory-II; CAPS, Clinician Administered Posttraumatic Stress Disorder Scale; PCL-M, PTSD Checklist Military Version; PSQI, Pittsburgh Sleep Quality Index; RC, reliable change; SD, standard deviation.
As shown in Figure 1, there was a trend of decreased symptom levels from pre- to posttreatment for all clinical measures. There was a statistically reliable decrease in PTS severity and symptoms as measured by the CAPS and the PCL-M, with five participants showing improvement on the CAPS and seven on the PCL. There was a statistically reliable reduction in BDI-II scores, with 6 patients meeting criteria for clinical improvement. There was no reliable change in mean scores for the BAI; however, five participants showed improvement, and one deteriorated. There was also not a statistically reliable change in the mean PSQI scores for the sample.
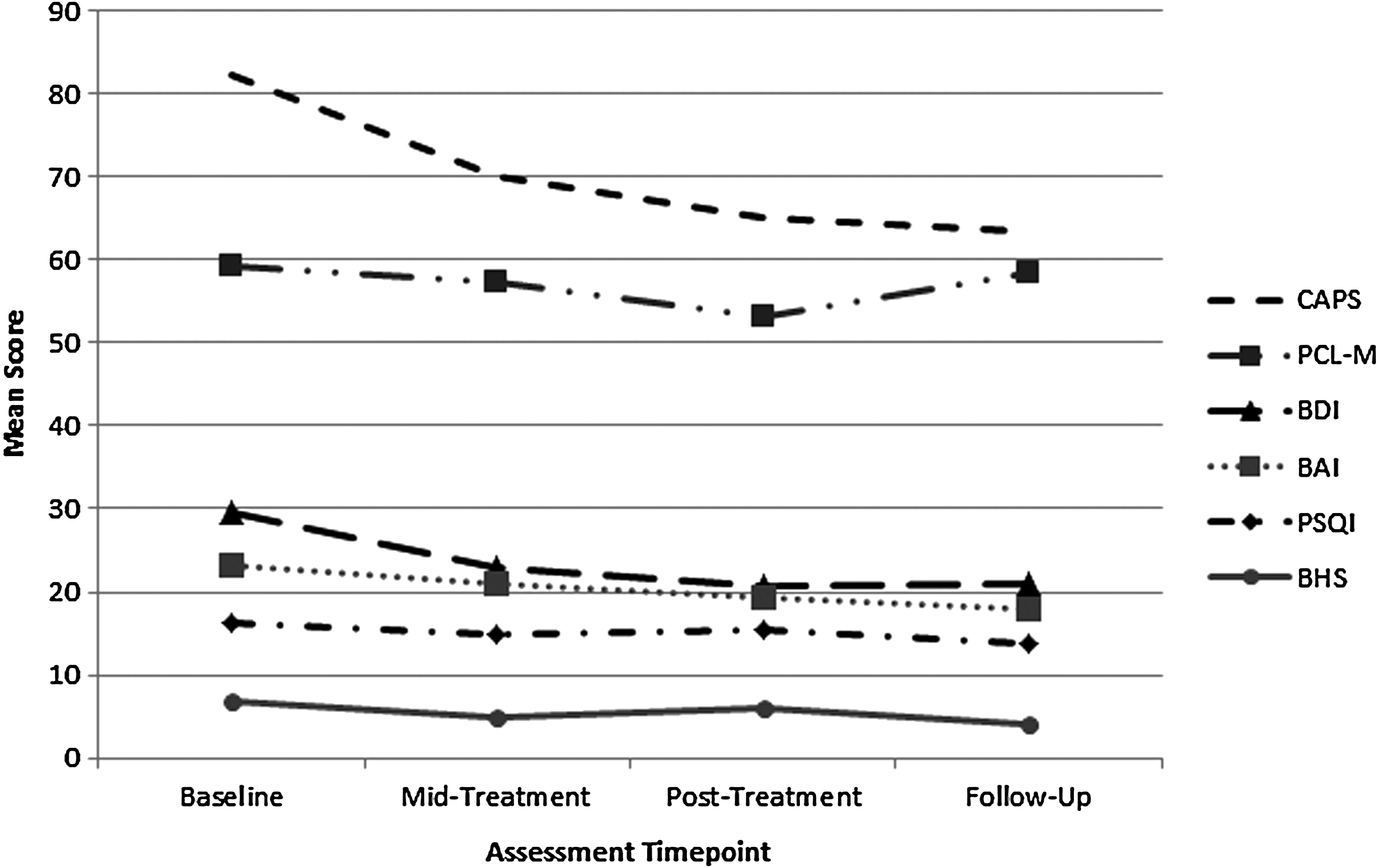
Means of clinical outcomes measures at each time point. BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; BHS, Beck Hopelessness Scale; CAPS, Clinician Administered Posttraumatic Stress Disorder Scale; PCL-M, Posttraumatic Stress Disorder Checklist Military Version; PSQI, Pittsburgh Sleep Quality Index.
Treatment Adherence and Satisfaction
Two of the 10 participants did not complete all eight treatment sessions; both withdrew from treatment following session 5. These participants reported that despite noticing that treatment had led to improvements in their quality of life and PTS symptoms, participating in the treatment required too much time away from their Army duties. One of these participants had experienced frequent technical difficulties that may have been a contributing factor to his decision to withdraw from treatment. Treatment completers indicated high overall satisfaction with the treatment on the CSQ-8 (mean=25.86, SD=4.74).
Technical Feasibility
As shown in Table 2, the most frequent technical issue was difficulty establishing a connection to the videoconferencing server. This problem was typically resolved with additional sign-in attempts. The average length of these disruptions was less than 6 min. More serious connection difficulties developed during an Army-wide network security upgrade that caused the Internet protocol addresses associated with some of the laptops to be blocked from accessing the video teleconferencing software's network. This occurred over a 2.5-month period during the study and necessitated multiple treatment sessions to be completed via telephone. One participant who completed the entire treatment protocol experienced six treatment sessions conducted by telephone. The second case completed five treatment sessions, three of which occurred over the telephone. This participant withdrew from the study after session 5. Although technical issues with initiating and maintaining a videoconferencing connection were more frequent than expected, they were managed effectively by study clinicians with simple troubleshooting steps and use of alternative contact methods per the study's protocol.
Technical Difficulties Occurring Across All 73 In-Home Telehealth Sessions
SD, standard deviation; VTC, video teleconferencing.
Safety Outcomes
There were no adverse events during the study or incidences that necessitated activation of our emergency protocol. At the baseline assessment, one participant endorsed thoughts of suicide but reported no desire or intent to act on those thoughts and was therefore eligible for participation. At the midpoint assessment this participant continued to endorse thoughts of suicide. However, by the end of treatment those thoughts were no longer present, and suicidal ideation remained absent throughout the follow-up period. Two other patients (who did not indicate suicidal thoughts at baseline) reported single-occurrence endorsements of suicidal thoughts midway through treatment but did not report any plan or intent to act on those thoughts. Both of these patients no longer reported suicidal thoughts at posttreatment or follow-up assessments. None of the participants expressed any specific desire or intent to harm others, and there were no incidences that required notification of a patient's emergency contact person or emergency services. There was never a time when a patient deliberately terminated the video teleconferencing connection during a treatment session.
Discussion
This study is the first to examine BA for the treatment of PTS symptoms among active-duty U.S. military personnel and the first, to our knowledge, to assess a home-based synchronous telemental health intervention in the U.S. military. The overall results provide initial support for the feasibility of HBTMH treatments in the military setting. The results also showed positive treatment effects of this novel intervention on symptoms of both PTS and posttraumatic depression that are consistent with other recent studies. 8,10 –12 Although the results did not show statistically reliable overall reduction with the sleep quality measure (PSQI), this is not surprising given the small sample size of our study. The results also suggest high levels of treatment satisfaction with HBTMH and the absence of any safety events provide additional data that mental healthcare can be delivered safely to service members in their homes when using workable safety standards and planning.
Although we did experience several temporary technical issues that caused some inconveniences for both patients and our study care providers, these issues did not appear to be detrimental to the treatment process. The technological aspects of HBTMH were manageable, and disruptions (primarily caused by the unanticipated network security upgrade) were usually corrected within several minutes of a problem. Our use of U.S. Army-approved and standardized laptops, software, and cameras helped assure technical compliance and control of potential hardware technical issues; however, this is also a limitation of the study. An ideal capability would be to use a network infrastructure that meets U.S. Department of Defense network security requirements but that also allows for the use of privately owned end-user equipment (i.e., personal computers, Webcams, mobile devices, etc.). Ultimately, the capability to use readily available privately owned equipment would be more convenient and economical for broad implementation. The optimal infrastructure for supporting enterprise-wide HBTMH videoconferencing capabilities in this setting needs to be determined.
In conclusion, HBTMH has the potential to greatly expand the range of services available to U.S. military members, veterans, and the general population. Although the current study is limited by its small sample size and lack of a control group, the findings support the notion that it is possible to deliver a similar quality and standard of care (i.e., an established, evidence-based treatment) to the home as in the clinic in the military setting. This study can serve as a model to investigate and implement other forms of home-based healthcare, and it provides decision makers with necessary preliminary data to make decisions regarding the expansion of HBTMH options for the U.S. military community.
Footnotes
Acknowledgments
This project is partially supported by the U.S. Department of the Army through federal grant award W81XWH-11-2-0118. The Military Operational Medicine Research Program, Fort Detrick, MD is the awarding and administering acquisition office. We are grateful for the contributions to this project made by Amy Wagner, PhD, Russell McCann, PhD, Lisa Thomas, LPN, CCRC, Katherine Stanfill, PhD, Karyna Boykin, CCRC, Michael Audas, MA, Mark Reger, PhD, Gregory Gahm, PhD, and Matthew Jakupcak, PhD. We are also grateful for the support of the Department of Behavioral Health and the Post Deployment Health Re-Assessment Clinic of the Department of Operational Medicine and Deployment Health at Madigan Army Medical Center.
Disclosure Statement
No competing financial interests exist.