
Abstract
Introduction
Cancer is a serious health problem worldwide, and 70% of cancer patients require radiation therapy. Active communication between a patient and doctors is essential to evaluate the therapeutic effects and adverse events resulting from radiation therapy and to ensure a successful outcome.
An interactive computer system (SISGRAD) capable of conducting computerized dosimetry has been established in the Department of Radiation Therapy at the Antoine-Lacassagne Cancer Center in Nice, France. 1 This center has been fully integrated with the institution's central Internet system and is responsible for managing radiation therapy provided at the center. A radiotherapy information system (START) has become integrated with the functions of other hospital departments to improve organizational efficiency when providing radiation therapy and to assist in statistical evaluation of clinical data. The START information flow identifies four major phases: admission, visit of admission, planning, and therapy. The system is managed by authorizing permissions. The system administrator can log-on to the information management system using the correct account name and password and then assign related permissions to other personnel, including permissions for allowing access, planning, and therapy, which helps ensure the security and confidentiality of patient data. 2
Telemedicine, which combines various aspects of the Internet, computer technology, and medical expertise, has become an important means of providing high-quality medical services and ensuring that patients receive appropriate health information with a minimum expenditure of money and resources. Such advances in healthcare communications and information technology can help provide long-distance clinical healthcare, health education, and health management services to patients. 3
Treatment of simple esophageal cancer with radical radiotherapy usually requires 42–49 days, 4 and proper follow-up is essential for patients who are discharged after completing the first round of radiotherapy. When treating esophageal cancer, the main reasons for treatment failure are lymph node metastases and local recurrence 5 ; hence, long-term follow-up is required to identify problems and to provide timely treatment. Furthermore, the efficacy of a treatment depends on proper patient compliance. In this study, we compared the results of using remote Internet follow-up with the results of routine follow-up among patients with esophageal cancer after they had received treatment with radiotherapy, with the purpose of providing evidence for improvements in patient compliance and treatment effects.
Patients and Methods
General Information
In total, 128 patients with esophageal squamous cell carcinoma after prior treatment with radiotherapy at the First Affiliated Hospital of Anhui Medical University of China (Hefei, China) were recruited for this study between January 1 and August 1, 2013. All study procedures were conducted according to a protocol approved by the Anhui Medical University Biomedical Ethics Committee (Ethical Committee protocol number 201311A). These patients were randomly assigned to either an observation group or a control group (64 patients per group) according to their discharge sequence, using a random number method.
The study inclusion criteria stipulated that the patients must have been diagnosed and pathologically confirmed as having esophageal squamous cell cancer according to the Standardized Guidelines on Esophageal Cancer developed by the Professional Committee on Esophageal Cancer of the Chinese Anti-Cancer Association in 2011. 6 All enrolled patients were adults with a junior high school or higher education, normal hearing, and normal comprehension ability. Patients in the observation group were required to have Internet access. Pregnant or lactating women and patients with a history of serious heart, liver, or kidney disease or other diseases were excluded from the study. Patients with cognitive impairment, hearing impairment, communication barriers, and those who refused the remote Internet follow-up were also excluded.
The study protocol was approved by the Ethics Committee of Anhui Medical University, and informed consent was obtained from each participant prior to enrollment.
Clinical Treatment
All esophageal cancer patients received treatment with intensity-modulated radiation therapy (DT60GY-66GY) and also received a chemotherapy regimen consisting of two courses of cisplatin (20 mg/day for 5 days) and 5-fluorouracil (0.5 mg/day for 5 days), administered both before and after radiotherapy.
Follow-Up Equipment
Hardware used in the study included two desktop computers (Dell [Round Rock, TX] Inspiron™ 660s series), one 23-inch full high-definition light-emitting diode display screen, and a SPEED-X300 computer sharing device (Kingroad Technology Co., Ltd., Shenzhen, China) used for purposes of connection. Software included a Windows™ (Microsoft, Redmond, WA) XP operating system (Chinese version) and an Internet Explorer™ (Microsoft) browser. Internet technology focused on developing systems for follow-up of cancer patients was used to provide a practical interface with a remote medical system. The final interface had a three-layer structure consisting of a data collection service layer, a data communication transfer layer, and a diagnosis and treatment management layer, respectively (Fig. 1).

The three-layer structure for remote Internet follow-up.
Follow-Up Content
The control group received routine discharge instructions and outpatient follow-up consisting of routine blood examinations, tests for liver and kidney function, chest radiography, esophageal barium meal radiography, etc. The observation group received the same routine follow-up testing, with the addition of follow-up using the Internet.
The Internet remote follow-up was performed using a data interface that permitted collection of information on various physiological parameters of esophageal cancer patients. After processing, the collected data were uploaded via the Internet to a medical information management system terminal, which then uploaded the data based on the query criteria. Each patient received a follow-up registration form and was assigned a network identification (ID) number or QQ number. By using the assigned ID or QQ number, the patient could register his or her hospital follow-up visit using the online management system with a log-in password of his or her own choosing. The follow-up was performed via a remote network and a short message service (SMS).
The system was managed using follow-up templates, roles, and permissions, and nonmanagerial staff members were denied access to patient medical records. This helped ensure the online security of the records. Patients were able to log into the diagnosis and treatment management interface through the Internet and to communicate with medical staff through the Bulletin Board System (BBS), Internet QQ (a popular social network software used for communication in China, and similar to MSN), or an Internet telephone (e.g., Skype, etc.), e-mail system or SMS, using a cell phone prepared for online remote follow-up.
The SMS platform consisted of two parts: an SMS-related business needs part and an SMS scheduling demon, of which the SMS-related business needs part included the follow-up of patients, discharge greetings, thank you notices for all types of blessings, queries to the SMS, and SMS statistics. Any user could send plain text messages, and administrators of the follow-up center could send customized messages, query the SMS, view SMS statistics, and record follow-up times. Furthermore, the administrators could send appointment reminders and tables with scheduled follow-up times to the patients and ask the patients for replies and confirmation.
The follow-up doctors were able to obtain a patient's medical information from a specific Internet Web page and to provide patients with treatment guidance according to the relevant medical records that had been provided by the diagnosis and treatment management interface (Fig. 2). All remote Internet follow-up was conducted by trained physicians, and a telephone follow-up was used for verification purposes.
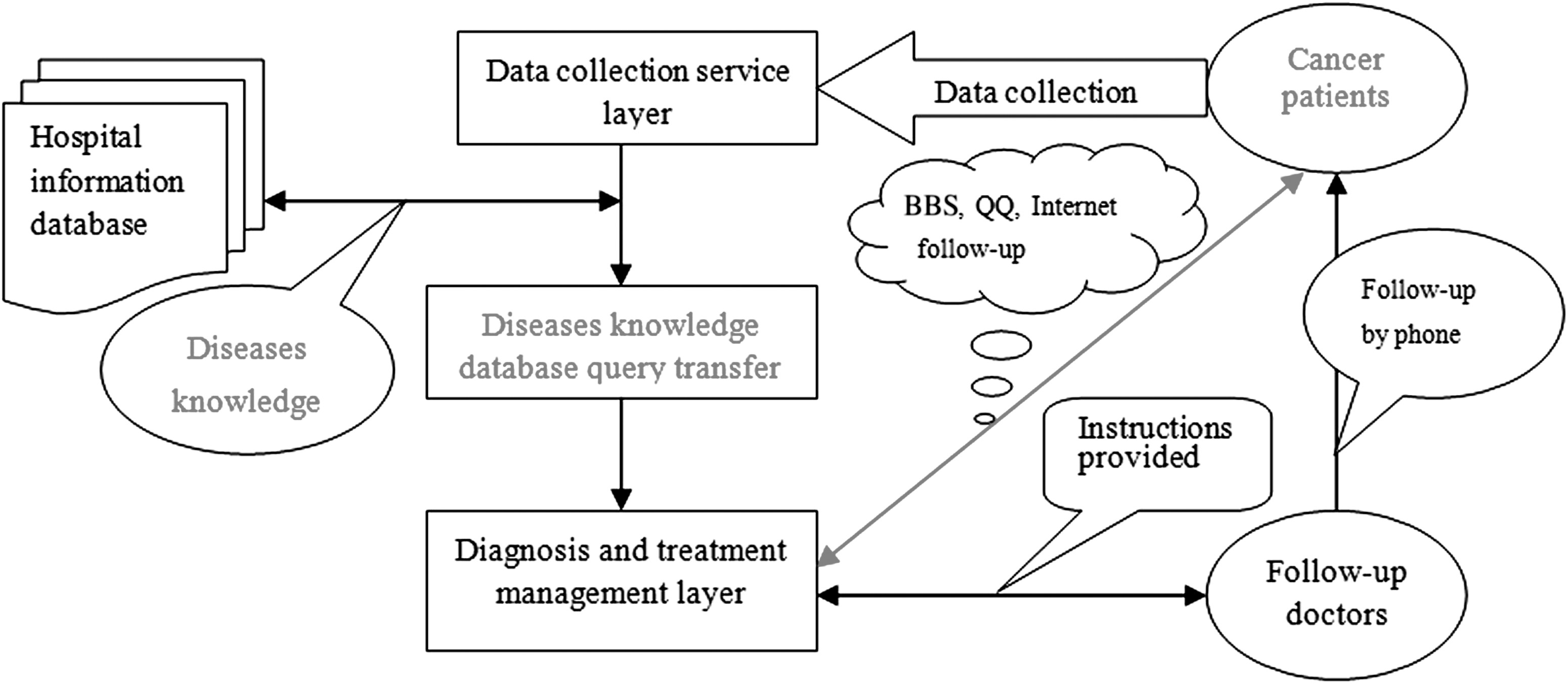
Flowchart showing follow-up methods. BBS, Bulletin Board System.
Follow-Up Documents
A follow-up file was created for each patient and included a follow-up registration form and an assigned Internet ID or QQ number that was used to record the patient's name, age, gender, telephone number (at least two phone numbers, one of which was a relative's number), radiotherapy registration number, the name of the administering physician, the patient's marital status, general patient information and health status of the spouse, patient medication status, and any psychological problems. Following receipt of this information, the follow-up dates were established, and the name of the follow-up physician was recorded.
Timing of Remote Internet Follow-Up
Patients in the observation group were required to log-in to the specified Internet diagnosis and treatment management Web page for relevant information on medical services. Follow-ups were conducted through an Internet QQ or video service on a weekly basis during the first and second months after patient discharge, every 2 weeks during the third and fourth months after discharge, and once a month during the fifth and sixth months after discharge.
Evaluation Indicators
After a patient had used the remote follow-up system for 6 months, a questionnaire was used to investigate patient compliance (use of prescribed medications and adherence to recommendations for periodic tests of blood, liver, and kidney function, as well as evaluations by chest radiography and esophageal barium meal radiography) and the short-term effects of radiotherapy. The Karnofsky Performance Status Scale 7 was used to measure levels of patient activity and to determine medical care requirements. Additionally, a demand questionnaire was also provided on the main interface of the remote follow-up page. Within the category of “treatment effect,” improvement was defined as a gradually reduced difficulty in eating and the absence of pain; effective treatment was defined as the lesion's length being reduced to one-third of its original length, as determined by esophageal barium meal radiography; and disease-free survival was defined as the tumor having completely disappeared and the absence of distant metastases at the time of follow-up.
In the current study, the term “lost to follow-up” refers to participants who at one point were active study participants but later could not be contacted and did not complete the follow-up portion of the trial. The term “missing to follow-up” refers to participants who were ignored by the medical staff during follow-up and became lost for further examination during the follow-up period. The term “available for follow-up” refers to the participants who maintained their regularly scheduled follow-up visits. The term “initiative consultation” refers to participants who consulted with medical staff for reasons of discomfort or to obtain medical knowledge. The term “periodic re-examination” refers to participants periodically entering the hospital for an examination according to regulations. The term “disease-free survival” refers to the tumor having disappeared and the patient remaining alive. The term “therapeutically effective intervention” refers to the tumor being reduced to a specified size following treatment. The term “reduction of symptoms” refers to the patient's subjective perception of feeling better.
Statistical Analysis Methods
SPSS version 17.0 software (IBM, Armonk, NY) was used for statistical analysis, and the chi-squared test was used to compare differences between groups. A p value of <0.05 was considered statistically significant.
Results
In total, 150 patients were screened for their eligibility to participate in this study. After 22 patients were excluded, 128 esophageal cancer patients (106 males and 22 females; 32–72 years of age) treated with radiotherapy were enrolled in the study (Fig. 3). The patients were randomly assigned to either a control group (n=64) or an observation group (n=64). There were 28 patients of T2 N0 M0 and 36 patients of T3 N0 M0 in the observation group, versus 31 patients of T2 N0 M0, 32 patients of T3 N0 M0, and 1 patient of T2 N1 M0 in the control group. No significant differences existed between the two groups regarding gender, age, pathological type, or Karnofsky Performance Status Scale score of the esophageal cancer (all p values>0.05) (Table 1).

Study flowchart.
General Characteristics of Study Participants
KPS, Karnofsky Performance Status Scale.
The median patient follow-up times were 187 days, with an interquartile range of 8 days, for the observation group and 64 days, with an interquartile range of 53 days, for the control group. One month after discharge from the hospital, no significant differences were found between the two groups regarding patient loss to follow-up, availability for follow-up, successful follow-up, need for re-examination, or lack of re-examination (all p values>0.05). However, follow-up examinations conducted at 3 and 6 months after discharge found statistically significant differences for all indicators (all p values<0.01) (Table 2).
General Characteristics of Study Participants at Various Times After Hospital Discharge
Data are number of patients.
Compliance with recommendations for medical consultation and periodic examinations was significantly higher in the observation group compared with the control group (p values<0.05) (Table 3). The observation group also showed higher levels of clinical improvement, effective treatment, and disease-free survival than the control group, which showed higher treatment efficacy (p<0.001) (Table 4).
Comparison of Postradiotherapy Compliance Between the Two Groups
Comparison of Effects of Treatment for Postradiotherapy Symptoms
Discussion
Our results show that compared with traditional follow-up techniques, use of remote Internet follow-up can reduce the numbers of patients lost to follow-up and improve postradiotherapy compliance and treatment results among patients with esophageal cancer. When using traditional follow-up methods, treatment compliance decreases over time due to patient relocation, economic problems, low awareness or knowledge of esophageal cancer, failure to seek a follow-up appointment for various symptoms, etc. Furthermore, hospital medical staff might also fail to follow up patients due to heavy workloads. Follow-up by remote Internet access is convenient and can be used to remind patients to receive further follow-up and provide guidance regarding treatment and lifestyle. Case and Simkus 8 reported that application of telemedicine produced benefits for patients with complex wounds and that nursing specialists could use the technology to remotely check a patient's condition using the Internet. Gfirtner and Kropf 9 used interactive technology to build a complete radiotherapy information system that could simultaneously manage diagnostic reports and radiotherapy protocols using queries or browsing functions. In the current study, patient data were entered into a computer data storage system to obtain a complete disease management plan for treatment through follow-up. This plan provided reliable data that could be used for disease diagnosis, treatment, queries, clinician consultations, and medical research. Today, with the development of telemedicine, several small-scale flexible remote Internet systems have been built throughout China, and these systems will support remote consultation, case discussion, and remote training.
In our study, the observation group showed a higher rate of patient compliance compared with the control group, and this might be related to the esophagitis that occurs after radiotherapy. The symptoms of esophagitis are similar to those for esophageal cancer and include pain during eating and feelings of obstruction. These symptoms result from local inflammation and edema of the esophagus following radiotherapy. When a patient communicated with a doctor via the Internet and received proper and timely treatment, the symptoms could be quickly alleviated. Such results prove that remote Internet follow-up is a convenient and efficient method for updating patient status and providing information to patients on how to receive treatment for adverse reactions. 10,11 A remote Internet system can help patients establish and enhance a sense of personal responsibility for maintenance of their own health, avoid transition lag that occurs when transferred from the hospital to home, and receive assistance in solving issues such as inadequate nursing care after discharge. Assistance in solving such problems is highly significant for improving patient compliance behavior and quality of life following discharge from the hospital. 12,13
Remote Internet connections can be used for reminding patients to receive follow-up and not miss appointments and also for providing medical guidance and services. Buller et al. 14 achieved good results by using remote telemedicine to disseminate dietary anticancer health information among multi-ethnic residents, guiding them to change their unhealthy eating habits. Telemedicine is a convenient method for providing health education, such as nutrition recommendations, to community residents, 15 and many patients with chronic diseases actively incorporate use of telemedicine into their daily lives. 16
Our study found that health information can be provided through Internet diagnosis and treatment management platforms and then be personalized for use by postradiotherapy patients with esophageal cancer. This information can be used to facilitate disease awareness, adoption of a healthy life style, and patient adherence to treatment regimens to help prevent recurrence and metastasis of esophageal cancer. The management aspects of the remote Internet program included posting of medical health information on BBS and providing self-care knowledge to patients with esophageal cancer after radiotherapy. Additionally, the Internet-based management program was also used to provide “one on one” guidance services, SMS reminders for re-examination and other services, psychological counseling, dietary guidance, information on adverse reactions after radiotherapy, online consultation, and quizzes concerning oncological diseases. Medical staff members were able to assess a patient's condition through the remote follow-up, provide healthcare services to the patient's home, and conduct posttreatment follow-ups and interventions. 17 –19 Therefore, use of remote Internet follow-up was effective for managing the posttreatment effects of radiotherapy in esophageal cancer patients and encouraging patients to respond to various posttreatment symptoms and improve their quality of life.
Conclusions
In summary, follow-up by remote Internet connection can be used to provide timely and personalized health education information to patients with esophageal cancer, and especially to patients who are moving and have Internet access. Remote follow-up changes patients from being passive in their behavior to being actively cooperative with treatment regimens, improves their quality of life, and reduces the recurrence of esophageal cancer. 20 –23
In conclusion, remote Internet follow-up is superior to conventional outpatient follow-up and has a positive role in providing medical guidance to postradiotherapy patients with esophageal cancer. Remote follow-up enhances patient adherence to treatment regimens and is worthy of recommendation and promotion.
Footnotes
Disclosure Statement
No competing financial interests exist.
P.W. participated in designing the study, carried out the molecular genetic studies, participated in the sequence alignment, performed the statistical analyses, and drafted the manuscript. L.Y. conceived of the study, participated in its design and coordination, carried out the immunoassays, and helped to draft the manuscript. Z.H. participated in the sequence alignment. All authors read and approved the final manuscript.