
Abstract
Introduction
Improvements in the healthcare system will require greater engagement of patients and their caregivers with the system. Shared decision-making involves participation by both patients and clinicians to share treatment preferences, to set goals, and to make joint determination of the treatment plan. 1
One of the engagement modalities is the patient portal. Patient portal is a general term used to describe a variety of health information access modalities, including Internet sites, interactive Internet-based programs, and sites to enter personal health data. 2,3 The term patient portal is not used uniformly to indicate that it is integrated with the electronic health record (EHR). For the purposes of this study, patient portal will refer specifically to a secure Web site, integrated with the EHR, through which patients can complete forms, communicate electronically with healthcare providers, access personal health information such as progress notes, problem lists, current medications, immunization history, laboratory data, and radiology reports, schedule appointments, request prescription refills, and pay bills. 4,5 The American Medical Informatics Association's College of Medical Informatics concluded that integrated personal health records offer more benefits. 6
Development of the patient portal has been driven in part by the belief that systems will enhance patient satisfaction, improve care, and make care more efficient. 7 Cross-sectional studies have demonstrated that people pay more attention and become more engaged in their health and medical care when they have easy access to their health information online and become participating members of the healthcare team rather than passive recipients of care. 4,8
Although patient portals are increasingly more common, there is little information regarding their use as a communication tool to connect patients, caregivers, and the healthcare team as partners, especially in the pediatric population. 4,7,9 The communication functionality is of concern because the EHR was not specifically designed and programmed initially to be a patient educational or patient involvement tool, and there are concerns that patients will see something in their record that providers never anticipated, or they might become anxious when seeing unfiltered data. Within the pediatric population there is an additional challenge of children maturing and of constructing the correct data feeds that ensure easy and appropriate access while maintaining confidentiality and privacy for both adolescent patients and their parents. 5,6,10
Parents of children with chronic conditions, who use multiple healthcare systems and providers, have identified the underutilization of the patient portal within the pediatric population. Parents expressed their desire to have one point of contact to manage their child's health condition and a one-stop electronic location for scheduling, calendars, and communication with providers. They have suggested that increased use of the portal for chronically ill children might be a tool to help alleviate some of their caregiver stresses, as well as a potential modality that helps teenagers manage chronic illness. 11 Additionally, adolescents with chronic disease must develop independent disease self-management and learn to communicate with their healthcare team to transition from pediatric to adult-oriented healthcare systems. 12
As health information exchanges help facilitate data sharing such as test results and clinical notes across healthcare systems through the use of data meeting nationally recognized standards for interoperability, privacy, and data security, they may work in concert with patient portals. Such broad data sharing could be very beneficial not only as pediatric patients age into adults, but also when they receive care within multiple healthcare systems, and improve the quality and efficacy of healthcare. 13,14
The purpose of this systematic review is to understand the state of the science of pediatric patient portal utilization, including to describe the ways in which authors have described the implementation of the patient portal, the ways in which it is integrated in the EHR, and the methodology adopted to measure the impact of the portal. These findings will help to identify gaps in the literature and to develop recommendations for future research.
Materials and Methods
The approaches used in this systematic review were informed by guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). 15
Search Strategy
We conducted a comprehensive search of four online databases (PubMed, CINAHL Plus, PsycINFO, and Academic Search Premier) for peer-reviewed literature published between 1992 and August 2014 (see Table 1 for search queries). Assisted by a librarian, we searched for literature on both electronic patient portals and electronic personal health records, including both terms because they are often used interchangeably in the literature.
Search Terms
The selection of articles is outlined in Figure 1. Each search provided citations and abstracts that were downloaded and subsequently imported into an Access® (Microsoft, Redmond, WA) database. After duplicated citations were removed, we identified a total of 138 unique references. One reviewer (R.A.B.) scanned the title and abstract (if available) of each unique reference for inclusion using the following criteria: human subjects only; peer-reviewed; published journal articles (no posters, conference proceedings, or dissertation); printed in the English language; and included some original research and data analysis (no review articles or commentary) on patient portals with some use in the 0–18-year-old age group. During our initial search we did not have any publication date restrictions for a more comprehensive search. In the second round four reviewers reviewed the full text of the 31 documents (seven or eight per reviewer) to determine final eligibility based on inclusion criteria. One discrepancy was resolved through discussion, and exclusion reasons were documented. While screening the articles, one additional article was identified using the reference lists in the articles. Overall, the review of the selected databases and articles, based on our inclusion criteria, resulted in the compilation of 11 studies. Ten articles were eliminated because they described a pediatric patient portal that was strictly Web-based and did not interact with an EHR.
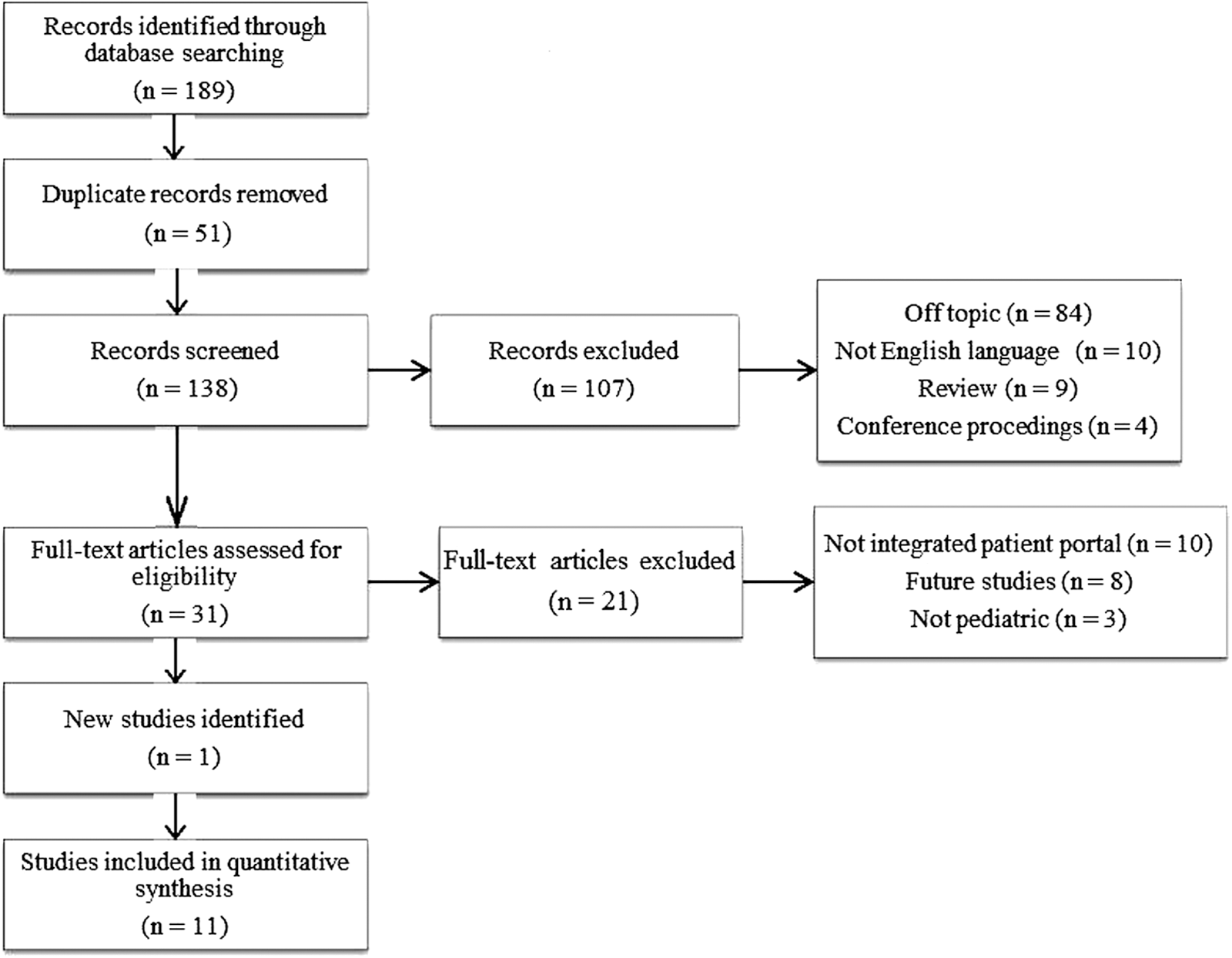
Search results.
We extracted data from the 11 articles and created a table including the following: study objectives; study design; setting; participants; intervention (where applicable); outcomes measures; and results. Where a study was not labeled with a particular design type, two reviewers assessed the study design and established consensus or the best categorization of the study methodology within the said hierarchy. In cases of disagreement, resolution was achieved through discussion between the reviewers or further review by a third author. The data were subsequently compiled and are presented in this article. Conclusions were drawn based on an aggregate synthesis of results with a narrative review of the evidence to further identify themes. Given the preliminary nature of most of the reported results, the wide variation of methodology used in the studies, and the absence of summary measures, we were unable to conduct an outcome-level assessment evaluating the reliability and validity of the data for each important outcomes by determining the methods used to assess them in each individual study as suggested by the Grading of Recommendations Assessment Development and Evaluation (GRADE) Working Group. 16
Results
Key findings of this systematic review include profiles and characterization of pediatric portal users and nonusers, frequency and type of portal utilization, end-user testing, development of targeted pediatric patient portals for patients with a chronic condition, and issues of proxy and total access to personal health information for teenagers. Highlights of each study are presented in Table 2.
Summary of Study Design and Key Findings of Publications on Pediatric Patient Portals
CF, cystic fibrosis; DM, diabetes mellitus; JIA, juvenile idiopathic arthritis.
Characteristics of the Studies
Seven studies (64%) assessed the use of portals and described characteristics of portal registrants and users. Two studies (18%) focused on usability testing, including portal utility and ease of navigation. One study (9%) explored how the portal might be used specifically to help manage healthcare for a child with a chronic disease. The final study (9%) targeted issues of the transition from partial to complete access to their own personal health information by teenagers. Patient or caregiver satisfaction with the portal was measured in nine studies. Study design included focused interviews (n=4), cross-sectional surveys (n=3), retrospective observational analysis (n=4), and usability testing (n=1). One study combined both cross-sectional surveys and focused interviews. The studies were conducted primarily in academic settings (n=8), with a focus on children with a chronic disease or ongoing medical condition (n=8), and relied on parental rather than patient input (n=8). The size of the study sample ranged from 7 parents to 84,015 patient records, but almost half (n=5) of the studies had fewer than 100 participants.
Most were focused entirely on pediatric delivery; two of the studies examined children as part of a multi-aged cross-sectional analysis. None was prospective, and none was a randomized controlled trial. Ten studies were from the United States, and one was from the United Kingdom. Three articles were published in 2010 or earlier and eight in 2011 or later, indicating a recent, substantial increase in the evaluation of the patient portal in the pediatric environment. (See Table 2 for article information and excerpts from the data about study objectives, settings, methods, participants, and outcomes.)
The patient portals varied considerably in the services that they provided. Many provided access to test results, secure messaging, and access to notes or visit summaries, whereas others were still the prototype phase. A few studies had additional applications that had been specially created by the healthcare institutions, such as additional attributes for pediatric asthma patients. 1 The portals were part of different types of EHRs, including Epic (Verona, WI) and Cerner (Kansas City, MO), as well as the United Kingdom computerized system.
Studies addressed utilization rates (n=4), satisfaction (n=6), barriers (n=6), patient characteristics (n=4), and chronic illness (n=6). Some studies addressed more than one item.
Portal Utilization
Reported utilization of the patient portal was generally low, especially in light of the cross-sectional nature of most of the studies, which did not follow adherence over time. Registration was as low as 4% (110/2,747) of 0–16 year olds in a United Kingdom general practice study and as high as 65% (256/166) of eligible responders to a survey of parent of children 0–5 years of age with at least one chronic disease. 17,18 Three studies reported account activation of 26–29% (8,409/31,765, 5,937/14,085, and 530/1,900) of children. 8,19,20 Of note, in the only longitudinal analysis, Byczkowski et al. 20 reported that only 16% (79/498) of children in their initial focus population comprising children with chronic diseases were still using the portal 3–6 months after registration. One study enumerated why the portal is used; parents with chronically ill children enrolled in a large health organization most frequently used immunization records, secured messaging, and scheduling appointments. 18
Patient Satisfaction
Parents of both healthy and chronically ill children like the concept of the patient portal. Following a demonstration of the portal to parents in an academic practice waiting room, 92% (59/64) thought the patient portal was easy to use, and they planned to view medical records and laboratory results in the future. 21 Parents who were part of a prototype demonstration felt that a good system will sustain communication and ensure patient safety. 1 Parents of chronically ill children (diabetes mellitus, cystic fibrosis, and juvenile idiopathic arthritis) reported that the portal was accurate and timely, helping them to communicate with their children's care providers. Additionally, the portal helped to manage and understand the child's condition, reducing anxiety and offering reassurance. 6,11 The portal has not replaced telephone calls. Eighty percent of parents in one study used the portal at least once a month but reported that it had not replaced calling the healthcare provider. 6 Teenagers felt enthusiastic about contacting their providers, seeking health information, and making appointments. 22
Reported Barriers
There were several reported reasons for not using an integrated personal health record, and they varied by study. Two studies that surveyed chronically ill children reported that drawbacks included difficulty in graphing and interpreting data, the need for more explanation of test results, and understanding medical terminology. 6,23 Other barriers included dislike of having separate accounts for each child and the lack of a symptom checker. 21 Logistical reasons included being too busy and forgetting the login/password for the system. 18 Concerns about confidentiality, especially among teenagers and their parents, are also seen as a barrier to use. 17,22
Racial and Socioeconomic Disparities
Among the study groups, portal users have a different profile than nonusers. Several studies reported that individuals of color and those with Medicaid or who were low income were less likely to obtain a portal account. 19,20 Although Tom et al. 18 reported no significant difference as measured by the Consumer Healthcare Providers and Systems composite measure, subanalysis demonstrated that users were likely to have more education and commercial insurance versus nonusers. Adolescents were also less likely to activate the patient portal. 19
Chronic Disease
Four of the 11 studies were working with parents of children with diabetes mellitus, juvenile idiopathic arthritis, and cystic fibrosis at a large academic hospital. 6,11,20,23 Additionally, Tom et al. 18 studied parents of children with at least one reported chronic disease, and Ketterer et al. 19 found that use of the portal was higher for children with autism and those who had more conditions listed on the medical report problem list.
Clinical Outcomes
The one study that looked at a clinical outcome found that among the entire study population 10–99 years of age, portal use was a statistically significant predictor of glycosylated hemoglobin level but not of low-density lipoprotein and total cholesterol levels. 8
Discussion
Principal Results
The 11 studies included in this systematic review each contributed results relevant to the understanding of factors associated with use of the electronic patient portal within pediatric patient populations. In spite of the variations in methodology used to capture implementation, acceptance, and use relative to each study, the reviewed studies consistently demonstrated that parents are interested in using the patient portal. The highly descriptive nature of the studies reflects that incorporation of the patient portal within workflows is still often in the implementation stage and that it has yet to be used by the majority of patient–parent dyads. The primary findings were those of short-term, patient-level measures to help clinicians document how successful they are at implementing a patient portal. Long-term measures to help document the impact on clinical outcomes and operational efficiency have yet to be reported. The studies did not consider the implications of the portal and for patient data sharing that will be enhanced by the health information exchange. For example, the health information exchange may enhance patient–provider communication and function as a personal health record comprising electronic data gathered from various sources, including the EHR. 14
More than half of the pediatric patient portal research to date has been focused on chronic disease patients and their parents, including management of diabetes mellitus, juvenile idiopathic arthritis, cystic fibrosis, asthma, and chronic disease not specified. 1,6,8,11,18,20,23 The research has focused on whether parents have registered to use the portal, are using the portal, and barriers to use of the portal. One study among a disparate age group examined health outcomes and found a benefit among portal users. 8 Further investigation of the role, if any, of the portal in supporting parents and patients in addressing pediatric chronic disease outcomes, promoting partnerships between patients and providers, supporting self-care, and enabling informed decision-making has yet to be reported. Although the technology did seem to be overwhelming, medical terminology is still perceived as a barrier. 6,23
Only one study had a longitudinal component, and there are still unanswered questions and metrics to gather regarding frequency of use, adherence to use, effect on work patterns for clinicians, and whether there are changes in outcomes among the effected patients. There remain gaps in the literature about pediatric clinical outcomes, healthcare utilization, and the utility of patient–provider communication.
With the exception of Tom et al., 18 the studies did not drill down into what defined convenience for the parent or the patient, such as being able to contact the doctor out of hours 24 or specific ease of test results accessibility. 25 Similarly, although the benefits of improved communication between patient and provider were cited as benefits of the portal, the research did not report or describe the mechanics behind the improved communication. Although parents in one study mentioned that they felt that the portal reduced their anxiety, 11 there was no evidence in this qualitative study that the parent-caregivers would describe this access as empowerment.
Although this point was not a primary point of analysis for the many qualitative studies, several of the cross-sectional studies indicated that income, race, and educational level are predictive of portal adoption. Individuals of color, those with Medicaid, and those with low income were less likely to obtain a portal account. Those with more education and greater income were more likely to use the portal. This is somewhat different than the adult literature, in which somewhat lower adoption among African Americans but reasonable adoption across all racial groups has been found. 8 Security and privacy were not overwhelming issues, unless it was in the context of adolescent access to a patient portal and what they and their parents might see. Although also not the primary topic of interest of the majority of the studies to date, the issue regarding access of adolescents to their medical records is still to be resolved.
Limitations
This systematic review approach is affected by several limitations. Larger institutions were among the early adopters for EHRs and are more likely to have data to report at this point. Pediatric academic institutions are over-represented in this review. There is not a variety of methodological approaches to support the conclusions presented. Half of the studies are qualitative in nature and designed to test a prototype or to be hypothesis generating for a larger research study. Most data gathering was cross-sectional, and longitudinal measure of adherence, tracking of those lost to follow-up, or capture of the effect of time on a health condition was not assessed. An additional limitation was that none of the studies measured if the consumption of services changed or other measurements of utilization. It is noteworthy that providers and their role in patient adoption of the patient portal and the impact of the patient portal are only tangentially mentioned.
Quantitative data including frequency of use over time, phone and Web-messaging volume, the impact on types of patient contact following portal adoption, provider productivity, and potential cost saving estimates are needed. Additionally, the issue of access of an adolescent to his or her medical record versus parent and guardian information access and the effect of such access or lack thereof needs to be undertaken so that the patient portal as a potential means of supporting the transition from pediatric to adult healthcare may be assessed. Is the patient portal a tool for greater focus on patient- and family-centered care?
Conclusions
The review sought to examine the use of the patient portal in pediatric populations. There is a limited body of research that has addressed the integrated pediatric patient portal. The majority of studies have been conducted in academic settings among parents of children with chronic conditions. Studies in more varied settings, using a variety of methodologies including prospective approaches with more participants, including providers and adolescent patients are needed to study the longitudinal impact of the patient portal on pediatric patient care and clinical outcomes. The initial results from the studies in this review do not yet provide implications for clinical practice but do indicate that there is great potential for pediatric consumer informatics studies and patient empowerment.
Footnotes
Acknowledgments
The authors thank Patricia Calero, MS, for her assistance and contributions to the structure of this manuscript. R.A.B.'s work was supported by grant K99 HS022404 from the Agency for Healthcare Research and Quality.
Disclosure Statement
No competing financial interests exist.