
Abstract
Introduction
Store and forward (S&F) teledermatology (TD) has been shown to be a safe and effective method for delivering dermatology care. 1 –3 Economic analyses have shown modest cost benefits depending on underlying assumptions made. 4 TD offers improvement of access for patients with sometimes dramatic reductions in wait time for care 3,5 and in face-to-face (FTF) dermatology visits avoided. 3,6,7
In 2009, we implemented a S&F TD program in Veterans Integrated Service Network (VISN) 20, focusing initially on rural underserved clinics and centers. At inception, the dermatology needs of approximately 250,000 veterans in VISN 20 were served by about 3.6 full-time equivalent board-certified dermatologists. The volume of consultation requests grew rapidly to about 700 per month; the volume of cases managed by S&F TD would have overwhelmed the clinic capacity of the dermatologists. TD implementation revealed an enormous unmet latent demand for dermatology services in rural areas. Given that the Veterans Health Administration (VHA) has recently come under scrutiny for problems in access to specialty care, 8,9 we wanted to know whether TD implementation in the presence of an unmet latent demand for dermatology services actually translated into improved access to FTF dermatology care. It has been suggested that TD may allow more patients to be evaluated and treated by dermatology. 10 However, the impact of a TD implementation on access to FTF dermatology has not been well documented.
In this communication we report on the effect of the TD intervention on access to FTF dermatology care for veterans in a secondary treatment facility with a full-time dermatologist.
Materials and Methods
Facility Description
The Mann-Grandstaff Spokane Veterans Administration (VA) Medical Center is a secondary treatment facility offering inpatient and outpatient medical, surgical, and psychiatric care. The facility also provides primary care at two community-based outpatient clinics in Wenatchee, WA and Coeur d'Alene, ID, at rural health clinics serving the Washington communities of Colville, WA, Tonasket, WA, Republic, WA, Sandpoint, ID, and Libby, MT, and through a mobile medical unit serving the communities of Moses Lake, WA, Moscow, ID, and Osburn, ID. The main facility in Spokane serves 30,090 enrolled veterans (J. Waters, VISN 20, personal communication), of whom 16,143 are assigned to 16.5 full-time equivalent primary care clinicians (information provided by the VHA Support Service Center). Dermatology is a specialty of the surgical service line at this facility with 1.0 full-time equivalent board-certified dermatologist. The community-based outpatient clinics were incorporated into the initial roll-out of TD and will not be considered further in this discussion.
VISN 20
VISN 20 encompasses nearly 1,000,000 square miles and 23% of the land mass of the United States. Of the 490,122 veterans currently enrolled in VA care in this area, 58.5%, 36.3%, and 5.1% are classified as residing in “urban,” “rural,” and “highly rural” areas, respectively (J. Waters, VISN 20, personal communication). They are served by eight “parent” facilities and at least 45 community-based outpatient clinics, outreach clinics, contract clinics, and mobile clinics.
TD Implementation
Two primary care clinicians (“primary care dermatology providers”) were selected and trained to perform cryosurgery, electrosurgery, intralesional injection of corticosteroids, shave and punch biopsy, and simple elliptical excision of benign and malignant neoplasms in July 2012. With the support of facility management, primary care clinicians were directed to start requesting TD consultation on veterans with skin conditions instead of traditional FTF consultations in August 2012, and carved-out time from primary care clinics was provided for the primary care dermatology providers to perform the procedures.
Pathway to Care
When a skin condition is identified at a primary care visit, an imager is summoned to take pictures and upload to the electronic medical record. The consultation request is transmitted to the Seattle Teledermatology Reading Center and assigned to a reader. The completed request is transmitted back to the requesting provider. The requesting provider is responsible for issuing prescriptions and providing instruction to the patient. If a procedure is required, it is scheduled with one of the primary care dermatology providers.
Data Sources
Data were extracted from the Corporate Data Warehouse by SQL query, VistA, the Computerized Patient Record System, and the VHA Support Service Center.
Inclusion and Exclusion Criteria
All completed requests for dermatology and TD consultation originating from the Spokane main facility from January 1, 2012 through June 30, 2013 were included. “TEST” patients were excluded. Patients whose consultation completion date occurred before the request date were also excluded.
Institutional Review Board
The VA Puget Sound Health Care System Research and Development Service Line deemed this “quality improvement research” exempt from institutional review board oversight.
Method of Procedure
TD was implemented at the Mann-Grandstaff Spokane VA Medical Center with facility leadership approval to train two primary care providers to perform basic dermatologic procedures in July 2012. Upon the return of these individuals to Spokane, carved-out time (a total of 3 half-days per 2-week period) for the providers from primary care was allocated to TD, taking effect in 1 month.
For the purpose of this analysis, we chose the date of training to be the start date of TD implementation. We refer to the 6-month period before TD implementation as the “baseline” period, the 6-month period after implementation start date as the “transition” period, and the subsequent 6-month period as the “intervention” period.
For each month of the study period, we obtained the number of FTF dermatology consultation requests, the number of TD consultation requests, and the number of requests for dermatology consultation (S&F TD and FTF dermatology). The total numbers of consultation requests in each category (FTF dermatology, TD, and overall dermatology) during the baseline period in each category (FTF dermatology, TD, and overall dermatology) were then compared with those of the transition and intervention periods in the same category.
Next, we compared the interval from consult request to completion date in each of the three categories (combined dermatology, TD, and FTF dermatology) with the interval from consult request to completion date in the same category during the transition and intervention periods.
The number of total dermatology requests (FTF plus TD) and the number of requests directed to TD from primary care and non–primary care clinics were obtained from the Corporate Data Warehouse. Uptake was calculated as the percentage of the total dermatology requests directed to TD.
The number of available clinic appointments during the baseline, transition, and intervention periods was obtained from the Computerized Patient Record System. The number of canceled or denied consultation requests during the baseline, transition, and intervention periods was obtained from the Corporate Data Warehouse. We obtained the number of approved requests for fee-basis care from Arthur Wisen at the Spokane facility.
Results
Three hundred nine requests (51.5±8.2 per month) for dermatology consultation (S&F TD and FTF dermatology) were received in the 6-month baseline period. The monthly number of requests increased steadily during the transition period. Four hundred thirty-three requests (72.2±9.6 per month) were received in the “implementation” period (Fig. 1), revealing a previously unmet latent demand for dermatology care of about 20 consultations per month (40% increase). Although the number of total and TD consultation requests increased, the monthly number of requests for FTF dermatology care decreased from 49±8 to 34±3 per month (p<0.01).
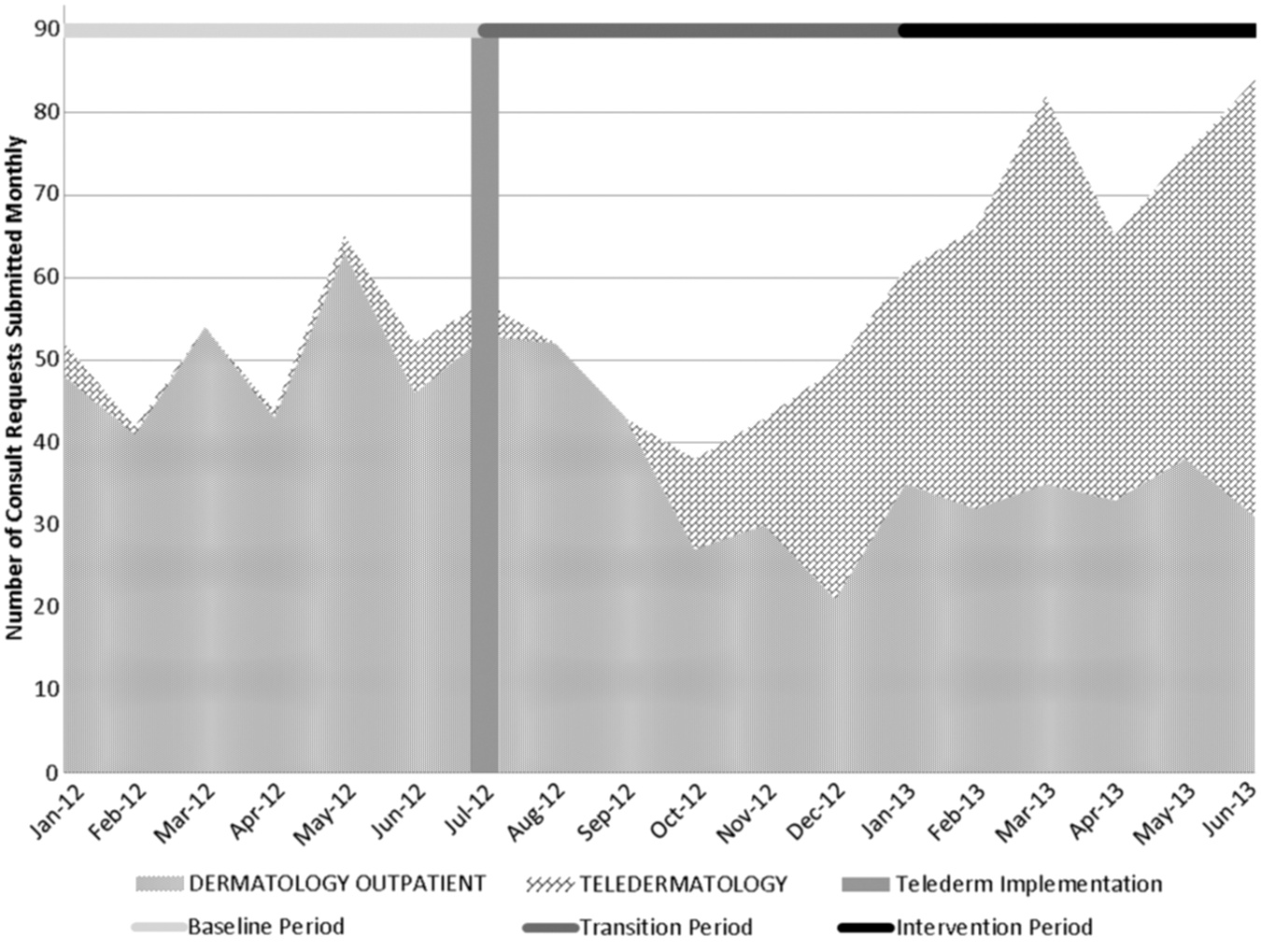
Number of consultation requests for dermatology care. The 6-month period from January through June 2012 is taken as the baseline (light gray horizontal line), the 6-month period from July 2012 through December 2012 is taken as the transition period (medium gray horizontal line), and the 6-month period from January 2013 through June 2013 is taken as the intervention period (black horizontal line). The solid vertical line indicates the point at which teledermatology was implemented (July 2012). The gray-scale fill pattern area indicates the number of face-to-face dermatology consultation requests; the diagonal brick pattern area indicates the number of teledermatology consultation requests.
Figure 2 shows the effect of TD implementation on wait time for dermatology care. Despite the increase in demand for dermatology care associated with TD implementation at the Spokane facility, the duration of the interval between consultation request and consultation completion for all dermatology (FTF and TD) declined from 61.2±29.4 days to 10.3±15.1 days (p<0.01). The interval duration for FTF dermatology consultation completion declined from 64.2±26.8 days to 20.3±18.6 days (p<0.01). TD consultation requests were completed in 2.8±2.6 days.
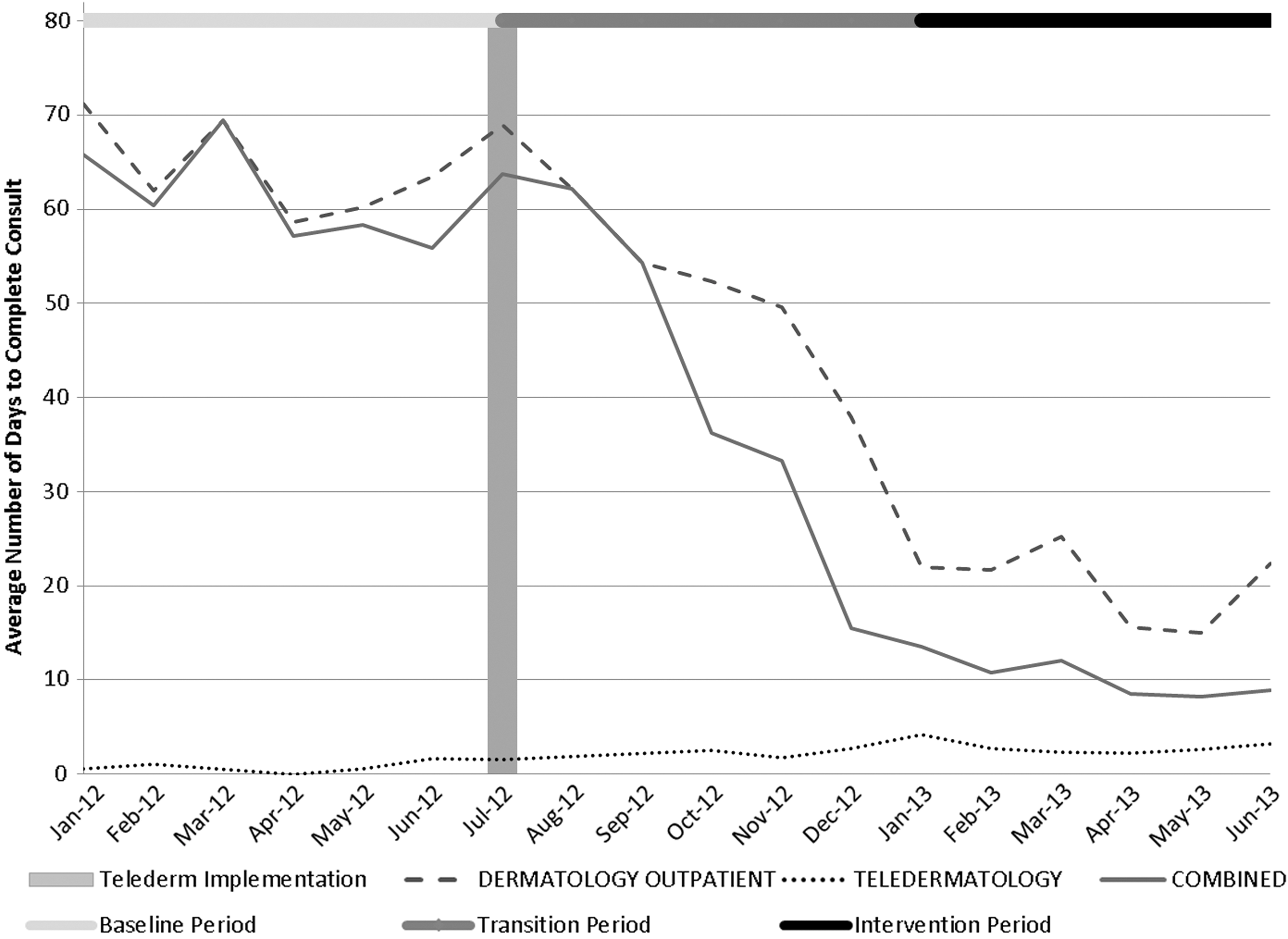
Interval (in days) between request for dermatology consultation and consultation completion. The 6-month period from January through June 2012 is taken as the baseline (light gray horizontal line), the 6-month period from July 2012 through December 2012 is taken as the transition period (medium gray horizontal line), and the 6-month period from January 2013 through June 2013 is taken as the intervention effect period (black horizontal line). The vertical line indicates the point at which teledermatology was implemented (July 2012). The dashed, dotted, and solid lines show the interval between consultation request and consultation completion for face-to-face dermatology care, teledermatology care, and combined dermatology care, respectively.
To gain confidence that it was the TD intervention that caused the decrease in FTF dermatology consultation requests and the improvement in the interval between consultation request and consultation completion, we sought to discover other factors that could have played a confounding role.
We compared the number of new consultation clinic appointments the dermatologist offered per month in the baseline period and in the intervention period: 51.8±8.3 appointments per month were offered in the baseline period and 51.8±9.7 appointments per month in the implementation period.
We ascertained the number of requests canceled or denied and found that there was actually a significant decrease in the monthly number of requests canceled or denied, from 20±4 per month in the baseline period to 7±2 per month, in the implementation period (p<0.01). Accordingly, the improvement in dermatology access was not due to increasing the number of requests canceled or denied.
When clinic capacity is exceeded or the facility does not offer the services required for care of the veteran, the veteran may be referred to a qualified provider in the community for fee-basis care. It follows that approving a large number of fee-basis requests would improve access to FTF dermatology care. In the baseline and implementation periods 25.2±21.5 and 5.2±5.0 fee-basis requests, respectively, were approved monthly, a significant decrease (p<0.01).
Although the improvement in access to FTF dermatology associated with TD implementation was expected and significant, we were somewhat surprised that the improvement was not even greater. To gain insight into the barriers, we analyzed the uptake of TD by clinical section in the Spokane facility. Figure 3 shows the uptake of TD, defined as the percentage of total dermatology consultation requests diverted to TD. The data show that uptake was substantially better in primary care than in other departments.
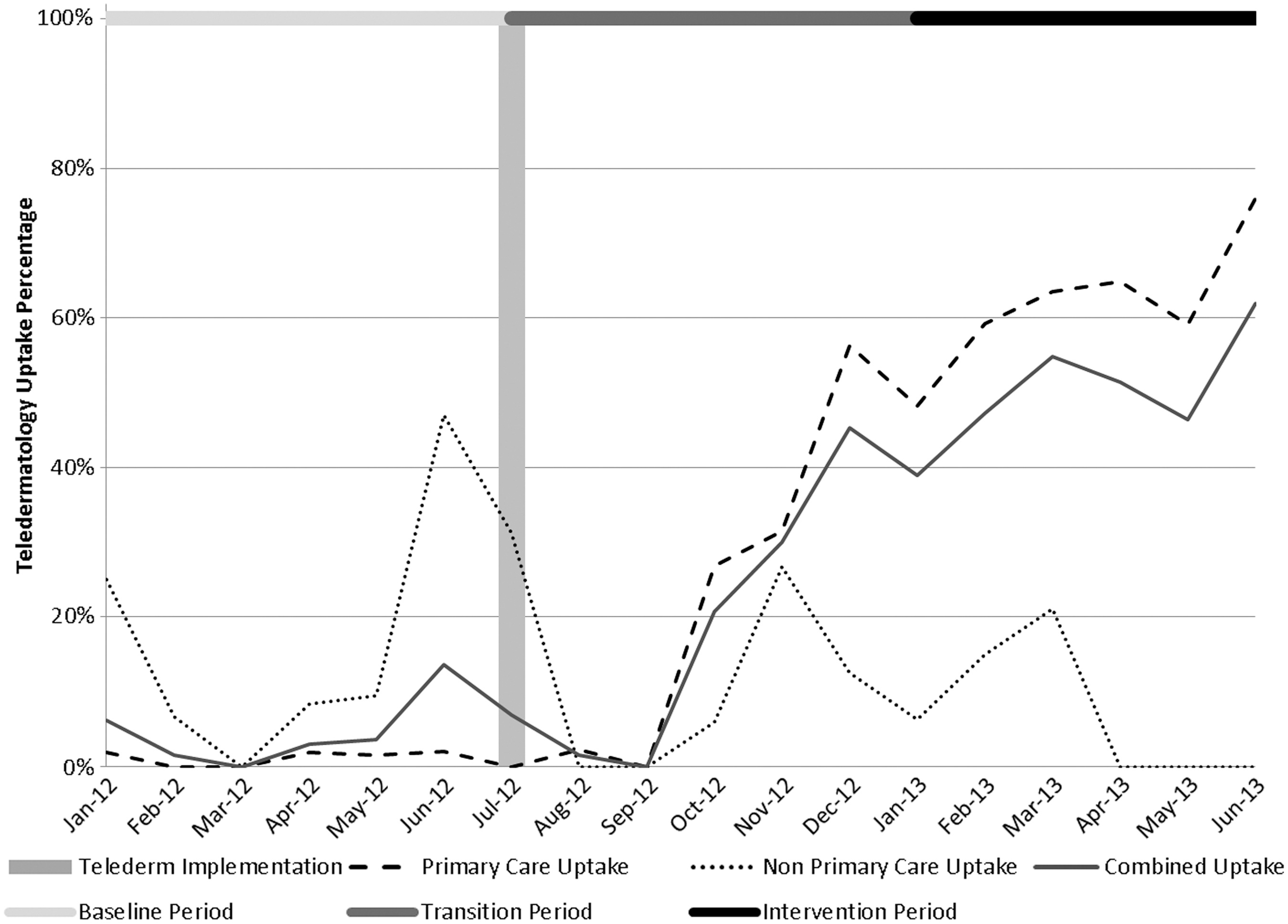
Uptake of teledermatology invention in primary care and non–primary care clinics. The 6-month period from January through June 2012 is taken as the baseline (light gray horizontal line), the 6-month period from July 2012 through December 2012 is taken as the transition period (medium gray horizontal line), and the 6-month period from January 2013 through June 2013 is taken as the intervention effect period (black horizontal line). The vertical line indicates the point at which teledermatology was implemented (July 2012). The lines represent overall uptake (solid), primary care (dashed), and non–primary care (dotted).
Discussion
In 2009, we implemented an S&F TD project in rural VISN 20, where access to dermatologists was severely constrained by the numbers of dermatologists and the distances to the centers with them. A needs assessment we conducted in 2009 revealed a substantial unmet need for dermatology services (authors' unpublished data) in rural areas, which was subsequently verified by a large number of requests for TD consultation.
When Office of Rural Health funding for our program expired in September 2012, we were directed to expand the service network to include the major urban centers, including those with dermatologists on staff. This provided us with an opportunity to ascertain whether there was a latent demand for dermatology care in a center with a full-time staff dermatologist and to determine whether TD implementation improved access to FTF dermatology care.
We discovered that TD implementation unmasked a significant unmet need for dermatology services, even in a facility with a full-time dermatologist. This issue has not been addressed in the TD literature and should become part of the resource planning when a TD intervention is proposed.
TD implementation has been demonstrated to improve dermatology access by its effect on the timeline of care of skin conditions. Of notable interest is the difference in wait time from request to consultation completion date between TD and FTF dermatology. A 2004 study found that the average consult request to completion date for TD was 7 days, with the longest interval around 16 days; in contrast, the average wait time to see a dermatologist in-person was 1 month from request date. 3 In a 2008 study comparing TD with FTF dermatology, TD was observed to require an average of 4 days from consult request date to completion date, versus a FTF consult request to completion date of approximately 48 days. 5 The decreased wait time may have been due in part to the number of clinic visits prevented by the use of TD.
A visit avoided is a commonly used metric for evaluating TD interventions. White 6 observed that TD use allowed one in four in-person clinic appointments to be avoided. Shapiro et al. 3 showed that TD implementation avoided 51% of FTF dermatology appointments. Other studies to date summarized by Warshaw et al. 7 have documented the percentage of visits avoided to range from 12.8% to 72%, depending on the percentage of cases requiring surgery. This metric assumes that patients seen in TD would all endure the expense and inconvenience of travel to see a dermatologist for their condition and therefore is probably an overestimate of the actual benefit to FTF dermatology access. In our analysis we directly ascertained the length of the interval between consultation request and consultation completion before and after TD implementation in a FTF dermatology clinic and found it to be greatly reduced. Although establishing causality may be not entirely possible, ruling out other possibly confounding factors, such as increases in the number of available consultation appointments, increases in the number consultation requests canceled or denied, and increases in the number of fee-basis authorizations, gives us greater confidence that TD implementation is the proximate cause for improved FTF access.
Our TD program completes requests in an average of less than 3 calendar days. When combined with the improved access to FTF dermatology care, the average wait for a patient to have his or her dermatology condition addressed was 10.3 days, down from 60.6 days in the baseline period.
This analysis was conducted on one VA facility. It is not known how generalizable these results are even within VISN 20 and the VHA, or in the private sector. During the preparation of this manuscript, colleagues at another VA facility published similar results. 11 Our metrics and those used by Bezalel et al. 11 for assessing access to FTF dermatology are direct and are likely an improvement over the inferential metric of “visits avoided.” Assessing confounding factors that may, of themselves, improve access should be an essential part of future analyses of this type.
The results presented in this communication show that even in a VA center with a full-time staff dermatologist, there is latent unmet demand for dermatology care and that an S&F TD implementation not only can meet the latent demand, but can significantly improve access to FTF dermatologist care with a very small investment of primary care provider time for training and performing directed procedures. The barriers to even greater improvement in access to FTF dermatology care may be solved by increasing access to imaging technicians for non–primary care providers.
Footnotes
Acknowledgments
The authors would like to thank Josephine Waters for making available the number of enrolled patients at the Spokane facility and the rurality designation of veterans enrolled in VISN 20. We would also like to thank Arthur Wisen for making available the number of fee-basis requests during the study period.
Disclosure Statement
No competing financial interests exist.