
Abstract
Introduction
Obstructive sleep apnea (OSA) is common in the veteran population with an estimated prevalence of 27–44%. 1 –5 The American Academy of Sleep Medicine recommends positive airway pressure (PAP) as an effective first-line therapy for treatment of OSA. 6 Treatment with PAP has been shown to improve cardiovascular outcomes, 7 –9 cognitive function, 10 quality of life, 10,11 and mood 11 and to reduce rate of hospitalization 12 and mortality. 13 However, management of OSA is often delayed due to lack of access to sleep medicine services. This is due to paucity of sleep specialists as well as of sleep laboratories worldwide. 14
The veteran population faces significant challenges in the delivery of sleep specialty care. In 2001 there were only 55 sleep laboratories in the Veteran Affairs (VA) Health System (VAHS), allowing only 160 studies per 100,000 population. 14 VAHS sleep programs have reported that patients wait 8–9 months from laboratory referral to sleep clinic evaluation. 14 In addition, sleep specialty care is often available only in acute care VA facilities, requiring significant travel away from a veteran's home.
Typically, sleep consultation involves evaluation of the veteran in the clinic before delivery of specialty care. Because of the paucity of sleep specialists this approach is fraught with problems, including delayed evaluation and delay in treatment. Patient satisfaction is adversely affected by long wait time, scheduling conflict, long travel time, and parking issues. 15
During recent years VAHS has implemented telemedicine technologies to improve care coordination and access to specialty care. 16 Telemedicine options include interactive video clinic visits as well as store-and-forward transmission of data/images for review by a specialist and electronic consult (e-consult). An e-consult allows secure information sharing between referring providers and the specialist, using the existing electronic medical record (EMR). The specialist answers the referring provider's questions on patients by performing a chart review. This approach improves access to specialist-directed care while decreasing response time to consult.
This study summarizes impact of telemedicine protocol on access to sleep apnea–related interventions at the Clement J. Zablocki Veterans Administration Medical Center (VAMC), Milwaukee, WI. In 2008 58,988 veterans enrolled for care at this VAMC. Based on an estimated 27–44% prevalence 1 –4 of sleep apnea, 15,927–25,955 patients needed access to sleep apnea–related care. The conventional protocol was to evaluate patients in the specialty clinic before providing any intervention. There were two part-time sleep physicians at the Milwaukee VAMC, and average wait time for clinic evaluation was ≥60 days. Thus, there were significant delays in diagnosis and treatment of sleep disorders. As sleep apnea is the commonest reason for referral to sleep clinics, a sleep telemedicine protocol was implemented in July 2008 to improve the timeliness to diagnosis and treatment of sleep apnea.
Materials and Methods
This is a retrospective system efficiency study. The differences between conventional (in-person clinic evaluation for every consult) and telemedicine protocols are shown in Figure 1. Per telemedicine protocol an American Academy of Sleep Medicine board-certified sleep specialist reviews the patient's EMR within 7 days of consult request. Based on a comprehensive chart review one of the following actions is taken: 1. PAP is prescribed for patients with confirmed sleep apnea based on documented results of portable or in-lab-attended sleep study. The consult is completed as an e-consult, and 30-day data download is scheduled to determine need for further intervention. • Patients are scheduled for a clinic visit for inability to achieve good PAP compliance on the 30-day download. (Good PAP compliance was defined as usage of PAP for ≥4 h/night on ≥70% of days on a 30-day download.) • Patients are scheduled for a clinic visit for complaints of persistent symptoms after initiation of PAP treatment. 2. Portable or in-lab-attended sleep study is recommended for suspected sleep apnea based on documented sleep symptoms, comorbidities, most recent body mass index, and blood pressure. The consult is completed as an e-consult. Negative or nondiagnostic portable sleep studies are followed by in-lab-attended sleep studies and/or sleep clinic evaluation. 3. Sleep clinic visit evaluation is scheduled for management of sleep disorders other than sleep apnea.

Comparison of workflow in conventional and sleep telemedicine protocols. 1 Sleep clinic wait time ≥60 days in 2008–2012. e-Consult, electronic consult; OSA, obstructive sleep apnea; PAP, positive airway pressure.
The VAMC EMR was interrogated to determine the trends in delivery of sleep specialty from 2008 to 2012 (a 5-year period) to determine the impact of implementation of the sleep telemedicine protocol. International Classification of Diseases, Ninth Revision, Clinical Modification codes were used to determine institution-wide rates of diagnosis of sleep-related disorders. Information regarding clinic wait time from 2008 to 2012 was obtained from the scheduling office at the Milwaukee VAMC.
Results
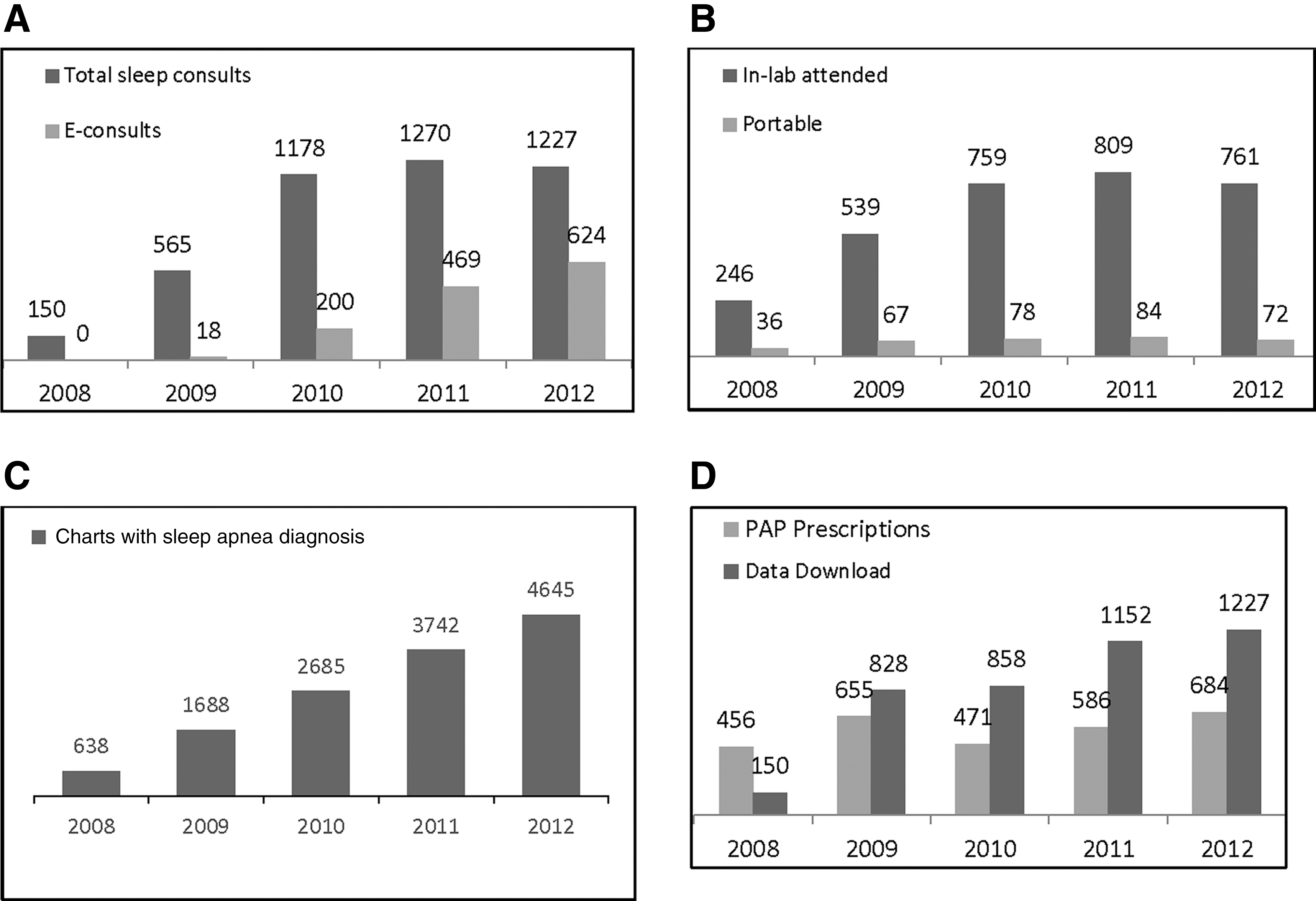
The sleep telemedicine protocol was implemented in 2008. Between 2008 and 2012, the total number of patients enrolled at the Milwaukee VAMC increased 4%, from 58,988 to 61,287. Of these patients 17–44% are estimated to have sleep apnea based on historical data. 1 –4 The number of sleep consults/year increased by 820% from 150 to 1,851 (Fig. 2A). The number of sleep studies/year increased by 330% from 282 to 833 (Fig. 2B). Diagnosis of OSA increased at a steady rate (Fig. 2C). PAP prescriptions increased by 150% (Fig. 2D). Follow-up as measured by total data card downloads/year increased by 820% (Fig. 2D).
The interval between consult to PAP prescription for confirmed sleep apnea decreased by ≥53 days (Table 1).
Wait Time for Positive Airway Pressure Prescription: Conventional vs. Telemedicine Protocol
Two board-certified part-time sleep specialists provided sleep electronic consult (e-consult) as well as sleep clinic services; there was no change in personnel between 2008 and 2012. Clinic wait time remained at ≥60 days during this period.
PAP, positive airway pressure.
Discussion
An increasing body of evidence demonstrates that telemedicine is an effective method of healthcare delivery. Improved outcomes have been reported using telemedicine in conditions like diabetes mellitus, 17 hypertension, 18 stroke, 19 and AIDS. 20 Studies have also demonstrated increased patient satisfaction and treatment adherence with use of telemedicine modalities. 15,21 Other potential benefits include improved access to healthcare, reduced waiting time for appointments, and reducing cost of care. Cost savings associated with telemedicine have been estimated at over $4 billion. 22
Telemedicine initiatives are widely deployed in the VAHS. They include store-and-forward telemedicine, remote monitoring, and real-time videoconferencing. Teleretinal imaging is an example of age-old commonly used store-and-forward technology utilized in VAHS to screen for diabetic retinopathy. 23 Real-time videoconferencing has been used in telehealth outreach clinics for mental health counseling and specialty clinics. 24
In the field of sleep medicine, telemedicine has been used for video visits, 25 home sleep testing devices, 26 and telemetric PAP titration methods. 27 Store-and-forward technology for OSA management has been used primarily for transferring polysomnograms from a remote site to larger facilities for interpretation. 28
The sleep telemedicine protocol implemented at the Milwaukee VAMC represents an innovative approach to management of sleep apnea. Our results highlight the enormous impact of this technology in addressing the issue of access to diagnosis and treatment services, thereby enhancing clinical care. After implementation of the sleep telemedicine protocol at the Milwaukee VAMC in 2008, there was a dramatic improvement in access to timely PAP therapy for patients with confirmed diagnosis of OSA. Chart review–based triaging of patients to e-consult management in partnership with the primary care physician versus sleep clinic evaluation markedly increased the efficiency of sleep care delivery.
It is interesting that the number of sleep consults and sleep studies increased rapidly during the first 2 years but slowed down subsequently (Fig. 2A). This trend suggests that there was a significant backlog in sleep care delivery that was accommodated during the first 2 years. Furthermore, although there was a significant increase in total consults and sleep studies, the number of PAP prescriptions increased only modestly (Fig. 2D), indicating that the telemedicine protocol allowed increased access to management for all sleep-related disorders and not just sleep apnea.
Before the sleep telemedicine protocol was set up, patients would often receive PAP without sleep studies due to the extreme delays in diagnostic services. As shown in Figure 2B and D, in the first 2 years after transition (2008–2009), the number of PAP prescriptions continued to exceed the number of sleep studies. From 2010 onward, the number of sleep studies exceeded the number of PAP prescriptions, suggesting careful assessment before PAP prescription. We suspect this was a result of rapid response to referring providers from sleep specialists via e-consults. Apparently, the telemedicine protocol facilitated implementation of American Academy of Sleep Medicine guidelines at the Milwaukee VAMC.
New sleep apnea diagnoses far exceeded PAP prescriptions during this period (Fig. 2C and D). This may be reflective of the fact that many patients had been started on PAP therapy without optimal documentation before 2008, and this aspect of care improved subsequently. It could also mean that many patients with mild sleep disordered breathing were not treated with PAP therapy but received other treatments instead (such as weight loss, positional therapy, mandibular advancement device, surgery).
Trends in rates of data download suggest that follow-up care for sleep apnea improved; data downloads in 2008 were <50% of PAP prescriptions but exceeded prescription rates in all subsequent years (Fig. 2D).
These results suggest that there was significant impact not only in quantity of sleep specialty care delivery but also the quality. Our results are pertinent not only to VAHS but to all health delivery systems where the EMR is used for interdisciplinary communication.
Conclusions
The advantages of telemedicine are already being realized in integrated healthcare delivery systems across the country. The telemedicine protocol highlighted in this study relied heavily on use of e-consults. Although the benefits of an e-consult in improving care coordination across various specialties and primary care physician satisfaction have been studied in prior studies, 16,29 our study is the first one that highlights the benefits of the e-consult in management of sleep apnea. The positive results demonstrated at the Milwaukee VAMC highlight the tremendous potential of this method to streamline the care of this highly prevalent chronic disease. This study supports the role of telemedicine in expediting and enhancing management of sleep apnea.
Footnotes
Acknowledgments
The authors of this article have done all the work including writing and editing without any external help. We acknowledge staff at the Sleep Department at the Clement J. Zablocki Veterans Administration Medical Center for providing us with data on the PAP prescriptions and downloads.
Disclosure Statement
No competing financial interests exist.