
Abstract
Introduction
Telemedicine, literally “medicine from afar,” enables doctor–patient encounters that would otherwise be inconvenient or impossible due to travel requirements. As the applications of this field broaden, telemedicine is being applied to visits that would have otherwise occurred in person, with the hope that cost savings and improvements in convenience for patients will be realized.
Although comprehensive economic analyses of telemedicine programs are challenging, 1,2 there are often measurable benefits to patients such as time saved traveling. 3 –7 On the provider side, telemedicine has been shown to reduce specialty referrals, 8 –10 but its effect on clinical volume in general is not well understood and most likely varies depending on the specific telemedicine application and healthcare setting.
The Veterans Affairs (VA) healthcare system has been actively engaged in broadening the applications of telemedicine, in part to increase access to services for its aging and often rural patient population. 11,12 Lack of reimbursement—a common barrier to entry into telemedicine—does not apply in the integrated VA health system. The VA system is also unique in that it provides beneficiary travel reimbursement (“travel pay”) to qualifying patients as compensation for time and money spent traveling to appointments. VA travel pay is projected to cost taxpayers nearly $1 billion in 2015. 13 Telemedicine has the potential to reduce VA travel pay reimbursements, but to our knowledge this potential savings has not been previously examined in the literature.
In this study, we analyze whether telemedicine has resulted in reduction in patient travel and reduction in VA travel payments over an 8-year period. In addition, we report trends in numbers of telemedicine and face-to-face visits over time to assist healthcare organizations in understanding how telemedicine program activity and face-to-face practice volumes relate.
Materials and Methods
Inclusion Criteria
All telemedicine visits conducted from the VA hospital in White River Junction, VT between 2005 and 2013 were reviewed. To be included, the visit had to involve live-interactive videoconferencing, with the exception of teledermatology encounters, which consisted of remote review of still images and recorded patient history (store-and-forward modality). Telemedicine encounters that involved only review of lab or test data (e.g., remote review of electrocardiograms or radiology images) were excluded.
Telemedicine Setup and Equipment
During live-interactive video telemedicine encounters at our center, the consulting healthcare provider uses a TelePresence® System EX90 (Cisco Systems, San Jose, CA), which is a high-definition system dedicated to telemedicine. A separate computer is used simultaneously to access the electronic medical record. The provider is located in a private office at the VA Medical Center, and signs are placed on the outside of the closed door to prevent others from entering during the encounter.
A health technician on the patient side coordinates the encounter, orients the patient to the telemedicine experience, performs the steps of the physical examination, and provides technical support. The qualifications of a health technician are analogous to those of a medical assistant. Patients are placed in private exam rooms within a community-based outpatient clinic. These rooms are equipped with i8500™ Mobile Telemedicine Stations (GlobalMed, Scottsdale, AZ), which contain video teleconferencing equipment as well as examination cameras and scopes. Telemedicine encounters are performed over dedicated lines with a connection speed of 384 kilobits/s.
Variables Collected
Demographics including age, sex, and military service-connected disabilities were collected. Characteristics of the telemedicine encounters were also collected, including the date of the encounter, the medical department administering the encounter, and the location of the encounter.
Key Variables and Their Definitions
Telemedicine travel distance was defined as the distance between the community-based outpatient clinic the patient attended for the telemedicine encounter and the patient's home zip code using the recommended driving directions from Microsoft Bing Maps (Microsoft Corp., Redmond, WA). Hypothetical face-to-face visit travel distance was defined as the distance between the White River Junction VA Hospital and the patient's home zip code. Travel times were estimated using the same software program, which provided route-specific travel time estimates.
Eligibility for travel payments was determined by applying the standard VA criteria to the study population. The VA criteria for the receipt of travel pay include having qualifying service-connected medical conditions, receiving a VA pension, or having a low-income status. 14 For eligible patients, the amount of travel pay that would have been received for face-to-face visits (i.e., travel from home to the VA hospital) was calculated using the standard Department of Veterans Affairs rate of $0.415/mile minus a $6 roundtrip deductible. The total White River Junction VA travel pay disbursement was also obtained from the business office for the years in which data were available (2012 and 2013).
Analysis
The number of telemedicine visits in each of the clinical departments participating in the telemedicine program was recorded for each of the study years. Trends over time in telemedicine participation were examined. Mental Health was the only department engaged in the telemedicine program over the entire study period, and thus clinical volumes in this department were further analyzed to determine how that particular telemedicine program changed over time. The number of telemedicine visits per year in this department was compared with the number of face-to-face visits, and the number of return visits was compared with the number of “unique” visits. The “unique” classification includes return patients on their first or only visit of the year, but also includes all new patients. Thus, this category was used as a proxy for the new patient volume, which itself was not available.
Results
In total, 5,695 telemedicine encounters were performed for 1,859 patients. The average number of telemedicine visits per patient was 3.1, although this ranged widely—from 1 visit to 63 visits. The average patient age was 63.1 years, and 94.2% were male (Table 1).
Patient Demographics and Characteristics of Telemedicine Visits at the White River Junction Veterans Affairs Medical Center, White River Junction, VT, Between 2005 and 2013
Other included dermatology (n=91), speech therapy (n=62), geriatrics (n=27), otolaryngology (n=5), and enterostomal treatment (n=3).
Telemedicine visits, compared with face-to-face visits, resulted in average travel savings of 145 miles and 142 min per patient per visit (Table 2 and Fig. 1). This resulted in a total reduction of travel of 824,724 miles over the study period and 13,400 h of driving. Among the study patients, 47.1% were eligible for travel payments, yielding a total travel pay savings of $164,394 over the study period, or an average of $18,555 per year or $28.86 per telemedicine visit (Table 2). However, due to the large increase in telemedicine participation toward the end of the study period, the yearly savings also increased. For 2013, this savings was $63,804, or about 3.5% of the total travel pay disbursement that year at the VA Hospital where the study was performed.
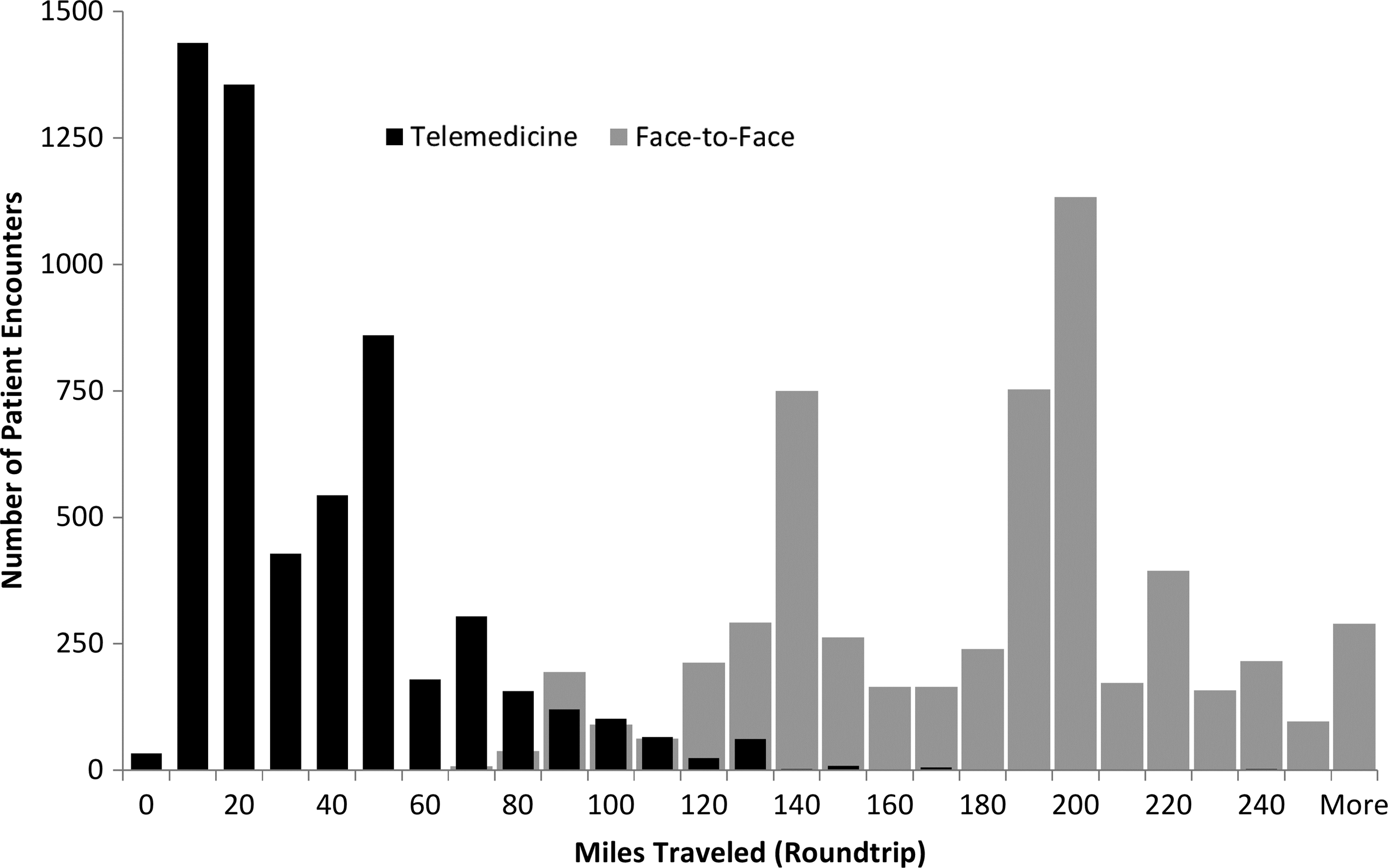
Roundtrip distances traveled during telemedicine visits versus face-to-face visits as part of the White River Junction Veterans Affairs Medical Center telemedicine program, White River Junction, VT, between 2005 and 2013.
Distance and Time Savings Observed for the Telemedicine Participants at the White River Junction Veterans Affairs Medical Center, White River Junction, VT, Between 2005 and 2013
Due to the rural location of this VA Medical Center, some patients would have had to travel 260 miles roundtrip or more to attend a face-to-face visit (Fig. 1); with the use of telemedicine the average travel distance was only 35.2 miles roundtrip in the telemedicine group (Table 2).
The largest number of telemedicine visits was performed in the Mental Health Department (46%), which was the only department engaged in telemedicine prior to a hospital-wide initiative to increase the use of telemedicine in 2011 (Table 1). There was an overall trend toward increasing telemedicine volumes in the Mental Health Department until the final year of the study, at which time a sudden loss of staffing led to an approximately 35% drop in telemedicine volume (Fig. 2). The Physical Therapy Department displayed an ability to both start and grow a telemedicine program rapidly, increasing its telemedicine volume nearly 10-fold over the last year of the study to become the department with the busiest telemedicine program (Fig. 2).
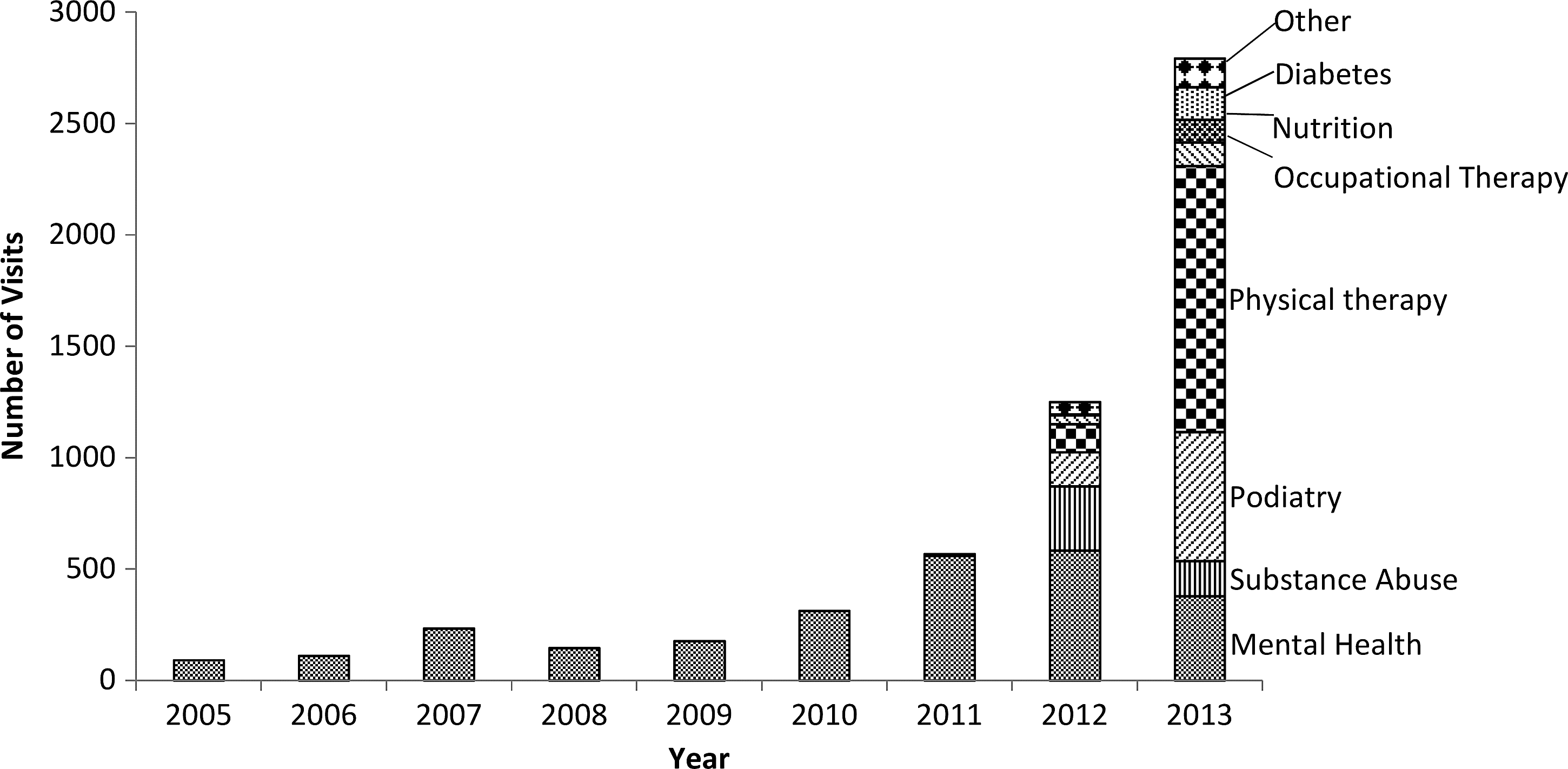
Total number of telemedicine visits per year by specialty at the White River Junction Veterans Affairs Medical Center, White River Junction, VT, between 2005 and 2013.
In the Mental Health Department, where the largest number of telemedicine visits was performed, the volume of telemedicine rose over the study period with fluctuations that mirrored the much larger face-to-face volume in the department (Fig. 3). Telemedicine accounted for a higher percentage of the Mental Health Department's unique visits (first or only visit of the year by a given patient) than it did of the return visits (Fig. 4).
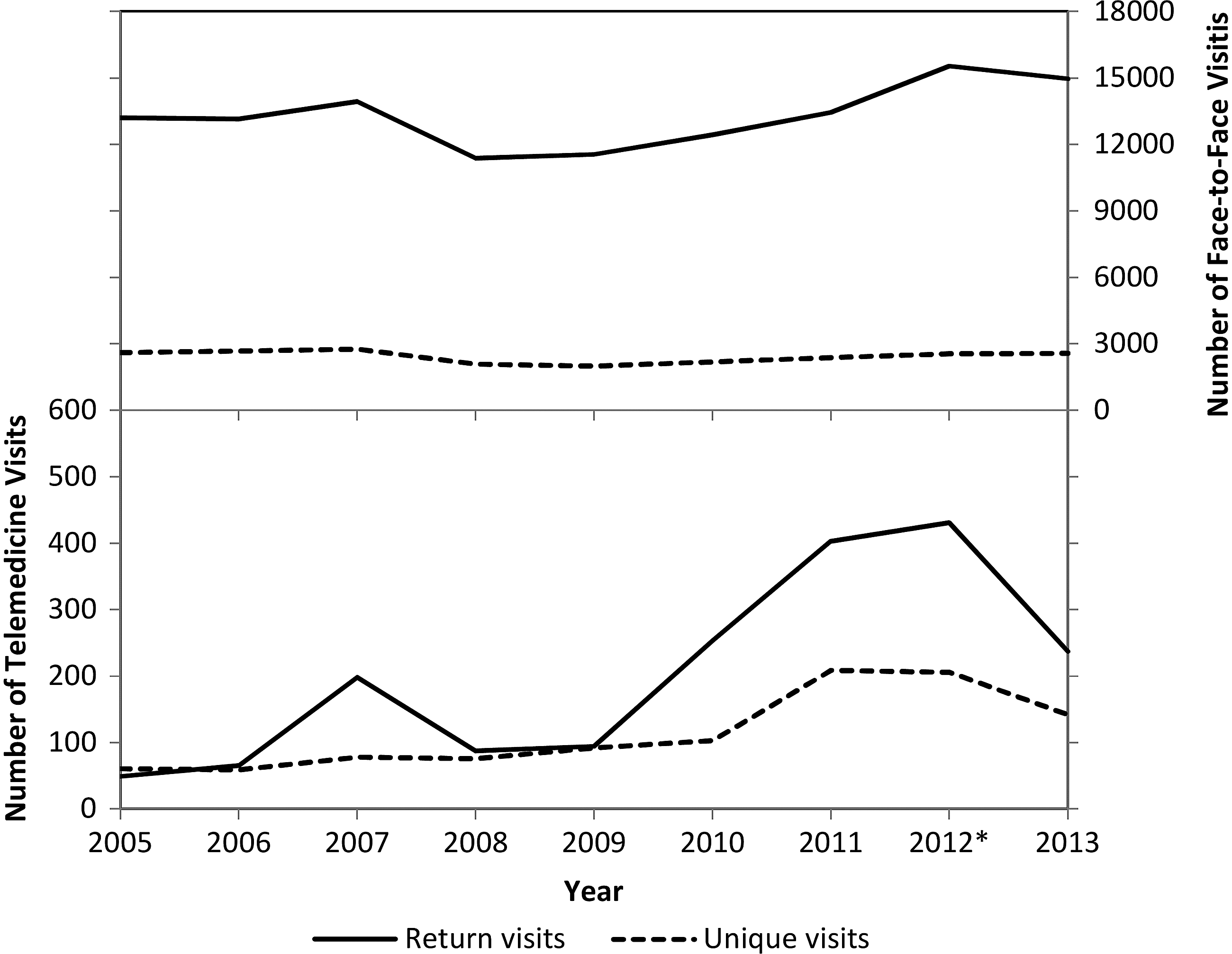
Number of mental health visits per year in the telemedicine program compared with face-to-face visits at the White River Junction Veterans Affairs Medical Center, White River Junction, VT, between 2005 and 2013. A unique visit is defined as first or only visit in a year and thus includes all new patients.

Percentage of mental health visits per year that are telemedicine at the White River Junction Veterans Affairs Medical Center, White River Junction, VT, between 2005 and 2013. A unique visit is defined as first or only visit in a year and thus includes all new patients.
Discussion
As the use of telemedicine continues to increase, issues of finances come to the forefront. The financial effect of a telemedicine program is complex, and determining whether there is savings associated with these programs is challenging. 1 Multiple studies have attempted to evaluate various aspects of cost savings associated with telemedicine, but comprehensive cost–benefit analyses remain elusive. 2,15 –18 Because telemedicine programs exist within a diverse range of healthcare systems, it has been argued that economic analysis of telemedicine in aggregate is futile and that each program needs to be evaluated individually in the context of its specific setting. 2
Thus, in this study, we attempted to analyze one of the economic factors that is unique to the VA healthcare setting and that had not yet been evaluated in the literature: the impact that telemedicine has on beneficiary travel pay. When considering the VA system as a whole, travel pay amounts to a large yearly cost. 13 We hypothesized that telemedicine would reduce travel payments by reducing the distances required to travel to appointments.
A significant reduction in travel distance on the part of patients with an average of 145 miles saved per telemedicine visit was observed. This savings reflects the rural nature of our medical center, located on the border of Vermont and New Hampshire, with some patients having to travel more than 260 miles roundtrip to come to the medical center. A smaller travel savings might be expected for a telemedicine program in a more urban setting. This reduction in patient travel would be expected to lead to additional benefits that were not directly measured in this study, such as savings on gas and vehicle maintenance, decreased absenteeism from work, and decreased risk of motor vehicle injury.
Surprisingly, we found the actual financial savings in travel pay on the part of the VA hospital to be relatively modest, reaching a peak of 3.5% of the total travel pay budget in 2013, when telemedicine participation was the highest. This is likely because telemedicine participation remained very small relative to face-to-face volume and because less than half of telemedicine participants in the study met qualifications to receive travel payments. However, this savings did increase as telemedicine volumes grew, and thus larger savings would be expected with even broader telemedicine adoption. Travel pay savings is also only one of many factors that contribute to the overall cost of a face-to-face visit. For example, telemedicine has been shown to reduce unnecessary specialty consultations by over 20% in several studies, and this may provide financial justification for its use in certain healthcare organizations. 8 –10
Total telemedicine volumes in the Mental Health Department—the longest telemedicine participant at our institution—steadily increased until the final study year, when they dropped off significantly. Querying the department leaders revealed that this drop in participation corresponded to a sudden loss of almost two-thirds of the mental health providers. However, it was also felt that there had been a saturation of both providers and patients who were willing to participate in telemedicine, that some patients and providers found the format “off-putting” even if the alternative required driving greater distances, and that technical difficulties (e.g., problems with cameras) had prevented more robust provider interest. These comments underscore the need for adequate technological and administrative support, as well as research into both the number of patients appropriate for telemedicine and their willingness to participate in the format, prior to initiating a telemedicine program in order to ensure long-term, sustainable success of such a program.
It is interesting to note that within the Mental Health Department, a unique patient visit (first or only visit of the year for a given patient) was more likely to be a telemedicine visit than was a follow-up visit (Fig. 4). In other words, more of the volume of new patient visits was shunted to telemedicine than was the volume of follow-up visits. This suggests that telemedicine in this context is useful for triage, after which patients are either redirected to further face-to-face visits or no follow-up is needed. Although the average number of telemedicine encounters in our study was 3.1 per patient, the number of visits did range up to 63, indicating that telemedicine was a viable long-term care strategy for at least certain individuals.
Some of the patients seen only once via telemedicine in our study may represent “unnecessary” consults, which telemedicine has been shown to reduce. 3,8 –10 It is also possible that some patients were dissatisfied with the telemedicine experience and requested future encounters be performed face to face, although this would run contrary to the generally high patient satisfaction that has been demonstrated in other telemedicine studies. 16 In fact, although not specifically examined in this study, telemedicine satisfaction is known to be high in the VA system, and average satisfaction for clinical video encounters was reported as 94% according to a 2014 VA report. 19
In the VA system, patient suitability for telemedicine varies by specialty and is determined by the consulting healthcare provider after reviewing the reason for the visit as well as the patient's distance from the medical center. If either the patient or the provider rejects telemedicine, the patient is seen in-person. This may differ from other institutions where patients are routinely seen first by a face-to-face visit, after which follow-ups can be performed over telemedicine if appropriate. This difference may have an effect on the number of patients who continue with telemedicine and on patient satisfaction scores.
This study was performed within the VA healthcare system, which is uniquely positioned to engage in telemedicine in that it is not constrained by interstate licensing requirements or traditional models of physician reimbursement—often cited as one of the barriers to broad adoption of telemedicine. 17 Within this context, reducing unnecessary consultations and minimizing face-to-face volume by the use of telemedicine are beneficial, whereas these outcomes may not be desired in practice settings with fee-for-service reimbursement structures. We thus acknowledge that the study setting limits the generalizability of our results. The VA is also unique in terms of its travel pay program, and the savings in travel pay associated with telemedicine demonstrated in this study would not apply to other health systems. There is also evidence that travel pay incentivizes veterans to seek medical care, 20,21 and it is not clear how travel pay reduction may impact utilization of healthcare resources.
In this study, we demonstrated that, at least in a rural setting, telemedicine is able to reduce patient travel significantly with corresponding savings in time. Within the VA system, this results in a reduction in travel payment disbursements, although this savings is currently modest and thus is unlikely to justify the use of telemedicine alone. We also showed that telemedicine volume is susceptible to changes in staffing and equipment issues and that visits are more commonly used for new patient evaluations. These findings provide some insight into the impact of an evolving telemedicine program, but further studies are needed to better understand the often complex costs and benefits of telemedicine to ensure that new telemedicine programs remain in the best interest of both patients and providers.
Footnotes
Acknowledgments
The source of funding is from the Department of Veterans Affairs, Dartmouth-Hitchcock Medical Center, Lebanon, NH.
Disclosure Statement
No competing financial interests exist.
J.E.R. is responsible for conception and design, data acquisition, analysis, interpretation of the data, and drafting of the manuscript. R.R.M. is responsible for conception and design, interpretation of data, and critical revision of the manuscript. L.D. is responsible for conception and design, interpretation of data, critical revision of the manuscript, and supervision.