
Abstract
Introduction
Telehealth interventions have become widely accepted as a means for assessment, education, and disease management in healthcare systems around the world. Such interventions overcome geographical challenges while providing convenient, immediate responses to patients and caregivers. Much has been published related to the value of telehealth interventions, and new journals have emerged devoted totally to telehealth and telemedicine. However, there are few studies evaluating palliative telehealth interventions for palliative care patients or their caregivers.
The vast majority of telehealth interventions have been directed toward chronic diseases such as diabetes, 1,2 heart failure, 3,4 and chronic obstructive pulmonary disease, 5 and the telehealth strategy is most often focused on preventing, managing, or improving the condition. Although one might argue that managing a chronic condition is palliative care, palliation has not been the stated goal in most telehealth interventions. Therefore, little is known about the value of telehealth that is directed toward the provision of palliative care.
When the patient is seriously ill or dying, the caregiver assumes the responsibility for managing care, receiving information, and communicating with professional clinicians and support staff. 6,7 Because the family caregiver is central to the patient's care and assumes major responsibility for the day-to-day management, it is recommended that supportive interventions be directed toward the caregiver when palliative care is the focus. 8
In order to develop a comprehensive perspective on the impact of palliative telehealth interventions on caregivers, we conducted a systematic review of the literature.
Materials and Methods
Search Strategy
The literature search was performed using the following electronic databases: Academic Search Premier, Ageline, CINAHL, Medline, Psychology and Behavioral Science Collection, Psych INFO, Sociological Collection, and TOPIC Search. Search terms used were telehealth and palliative care, telehealth and advanced cancer, telehealth and hospice, and telehealth and chronic illness. The term telemedicine was intentionally not used as this generally refers to telehealth education and communication among healthcare providers; however, telehealth and telemedicine are used by some interchangeably, and 32 telemedicine articles were included in the search results.
Inclusion Criteria
To be included in this review, an article had to meet the following criteria: 1. The intervention was focused on patients receiving palliative or end-of-life care for a serious condition (i.e., advanced disease, end-stage disease). 2. The study reported caregiver outcomes using either qualitative or quantitative measures. 3. The study was published in English between January 2003 and January 2015.
Reports that described an intervention or evaluated the feasibility of an intervention but did not report caregiver outcomes were excluded, as were single case studies. Studies focused on chronic conditions not considered to be advanced or end stage without a stated purpose of providing palliative or end-of-life care were also excluded.
Study Quality Evaluation
The Cochrane Collaboration's tool for assessing risk of bias in randomized trials was used to evaluate study rigor and quality. This tool evaluates study performance on six domains of bias: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other bias. 9 Developed by the Cochrane Collaboration's methods groups in 2005, this tool is used to identify flaws in design, conduct, analysis, and reporting that can cause the effect of an intervention to be underestimated or overestimated.
All three authors reviewed each article to be included and participated in extracting descriptive information for Table 1. Each also evaluated risk of bias independently. The authors then consulted to develop consensus regarding Table 1 and study quality evaluation. The PRISMA Statement for reporting systematic reviews 10 was used to structure our analysis.
Systematic Review Data Extraction Form
AHTSS, after-hours telephone support service; BFS, Benefit Finding Scale; CAI, Communication Anxiety Inventory; CBI, Caregiver Burden Inventory; CES-D, Center for Epidemiological Studies Depression Scale; CHESS, Comprehensive Health Enhancement Support; CPMQ, Caregiver Perception of Pain Medicine Questionnaire; CQLI-R, Caregiver Quality of Life Index-Revised; CR, Clinician Report; ESSI, ENRICHD Social Support Instrument; FFFS, Feetham Family Functioning Survey; HQLI, Hospice Quality of Life Index; MOS SF-36, Medical Outcome 36-Item Short-Form Health Survey; MSS, Mastery of Stress Scale; PSS, Perceived Stress Scale; PST, problem-solving therapy; QOL, quality of life; QOLLTI-F, Quality of Life in Life Threatening Illness-Family instrument; STAI, State-Trait Anxiety Inventory; SV-POMS, Shortened Version of the Profiles of the Mood Status.
Results
Study Inclusion
One hundred eighty-six articles were identified using the search criteria described above. Another 35 were identified through supplemental searches, including review of references cited in each relevant article. Of the 221 considered articles, 212 were excluded for various reasons (Fig. 1). Twenty-four articles and several of the systematic reviews included in the search results were directed toward chronic disease management without a documented focus on advanced disease, palliative care, or end of life and were excluded from the final results. Fifty-six of the articles described interventions but did not report outcomes. Table 1 displays the nine studies included and describes the design, population, intervention, outcome measurement, significant results of each, and study quality rating.
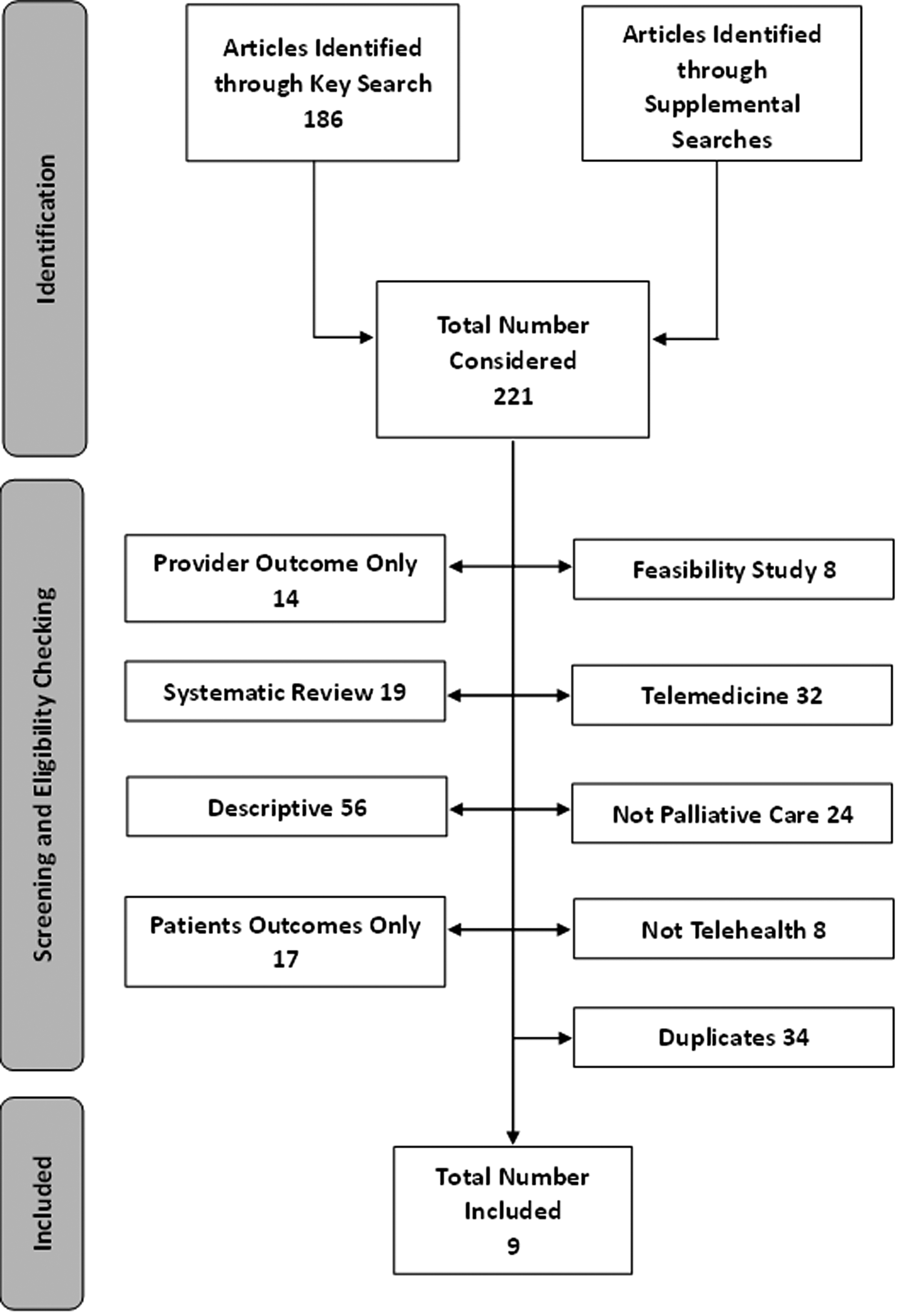
Flowchart of literature search procedure for eligible studies.
Study Quality/Rigor
Using the Cochrane Collaboration's tool for assessing risk of bias, the nine studies were categorized into three quality/rigor levels: high, moderate, and low, with low risk of bias indicating high quality/rigor (Fig. 2). A study was considered high quality/rigor when it met at least five of the seven criteria for low risk of bias (>75%), a study was determined as moderate quality/rigor if it met between one and four of the seven criteria for low risk of bias (25–75%), and a study was determined to be a low quality/rigor study if it met none of the seven criteria for low risk of bias (<25%). Of the nine studies, the majority (77.8%) scored as moderate. Only two of the nine studies reported a randomized process of participant recruitment and allocation, and none reported using a process of blinding participants. However, all of them described the completeness of their outcome data reporting for main outcome measures.

 ; and unknown risk of bias,
; and unknown risk of bias,  .
.Patient Characteristics
Of the nine studies, four recruited patients from local hospice programs, 11 –14 whereas two recruited from palliative care programs. 15,16 Patients in one study were from a pediatric palliative care program. 17 One study recruited patients with heart failure from cardiac care programs, 18 and one recruited patients from cancer centers. 19
Caregiver Characteristics
The caregiver samples ranged from 815 to 21719 participants. All of the participants were adult caregivers over 18 years of age. Caregivers' relationships to the patient included spouses/partners, parents, children, and others (siblings, grandchildren, daughters-in-law) to the patients, although three studies did not report the type of relationship. 12,13,15 The caregivers were from various locations, including both urban and rural areas. Five studies took place in the United States, 11 –14,19 two in Australia, 15,17 one in Taiwan, 18 and one in Canada. 16
Measurements and Data Collection Methods
Of the nine studies, five measured the caregiver quality of life using various scales, including Caregiver Quality of Life Index-Revised, 11 –13 Quality of Life in Life Threatening Illness-Family instrument, 17 and the Medical Outcome 36-Item Short-Form Health Survey. 14 Three measured caregiver anxiety: two of them using the State-Trait Anxiety Inventory and one using Communication Anxiety Inventory. Two measured caregiver burden using the Caregiver Burden Inventory, one used the Chinese translated version Caregiver Burden Inventory, and one used only a subscale of the Caregiver Burden Inventory. Other instruments used in the nine studies included the Caregiver Perception of Pain Medicine Questionnaire, Mastery of Stress Scale, the Feetham Family Functioning Survey, the Shortened Version of the Profiles of the Mood Status, the Center for Epidemiological Studies Depression Scale, the Perceived Stress Scale, the ENRICHD Social Support Instrument, and the Benefit Finding Scale.
Seven out of the nine studies used quantitative measures and analysis. The other two studies 15,16 used predominately qualitative methods (interviews and analysis of documentation) coupled with utilization data.
Telehealth Technology
Of the nine studies, four used videophones to simulate face-to-face communication with medical professionals. 11 –13,16 Two used regular phones for the purpose of counseling. 14,15 Two used Internet-based interventions. 18,19 One study did not report the details of the telehealth device used in the intervention. 17
Findings
Telehealth and caregiver quality of life
All five of the studies measuring caregiver quality of life 11 –13,17 showed no significant difference between the experimental and control groups (or between pretest and posttest). Caregivers in the single-group feasibility study showed decreased physical quality of life over time. 14
Telehealth and caregiver anxiety
The anxiety score significantly decreased after the intervention in two studies. 12,13 One study did not show significant improvement in caregiver anxiety. 11
Telehealth and caregiver burden
Of the two studies testing caregiver burden, one reported that the intervention group experienced significantly reduced caregiver burden, 18 and the other showed no significant difference on the caregiver burden measurement. 19
Other measured outcomes
Besides the findings listed above, there were other outcome measures used in the nine studies. One study 18 found that the intervention group experienced significantly improved family functioning by reporting patients' physical data through the telehealth device and accessing 24-h telehealth support. Chih et al. 19 found an online symptom reporting system helped caregivers to reduce negative mood. Kilbourn et al. 14 found caregivers who received the telehealth intervention showed decreased depression and perceived stress and increased social support and benefit finding over time. Another study 11 found no significant difference in anxiety between baseline and follow-up.
Feasibility/Satisfaction
Although feasibility of or satisfaction with the telehealth intervention was not a focus of this review, many studies reported such findings. Of the nine studies, four concluded that the telehealth intervention was feasible. 11,12,14,16 Five found overall caregivers' satisfaction with the intervention. 12,14 –17
Discussion
This systematic review sought to assess the effectiveness of telehealth interventions for caregivers of patients in home-based palliative care across multiple studies. Overall, this systematic review suggests there is evidence of overall satisfaction in caregivers who undergo a telehealth intervention; studies reported that the interventions were well received, and few technological issues were reported.
Of the nine studies identified, the majority (66.7%) reported improvement of quality of life and decreased level of caregiver burden, anxiety, depression, and/or stress as a result of the telehealth intervention. There was little duplication of measures across the studies, making it difficult to assess the impact of telehealth interventions across studies, but there is at least weak evidence to support the use of telehealth as an efficient and effective strategy in improving a variety of quality of life indicators and alleviating psychological distress of caregivers for palliative care patients, especially for those living in underserved rural areas.
Based on the Cochrane Collaboration's tool for risk analysis, the quality of the studies was predominantly moderate. Methodological limitations in study designs and/or small sample sizes contributed to lower quality. As is common when conducting research in palliative and hospice populations, recruitment and attrition due to mortality challenged some of the researchers. Only two of the nine studies used an experimental design. More scientifically rigorous research is needed both in palliative care and in the evaluation of telehealth interventions.
This review has several strengths. It utilized an extensive, comprehensive, and reproducible search strategy. It utilized a rigorous and transparent study quality assessment and applied strict inclusion and exclusion criteria. The authors reviewed all procedures and developed consensus as to content of the extraction form and study quality evaluation.
Limitations of this review should be addressed as well. The number of studies in this systematic review was lower than might be expected. Chi and Demiris 20 found 52 experimental studies reporting telehealth tools and interventions to support family caregivers. However, there are few studies that specify a focus on palliative, hospice, or advanced disease patients only. Our findings include only English-speaking populations.
Telehealth interventions have the potential to improve the experience of caregiving for those who care for palliative patients, but more rigorous research to test and evaluate such interventions is needed to justify telehealth approaches in palliative care.
Footnotes
Disclosure Statement
No competing financial interests exist.