
Abstract
Introduction
The rapidly growing population of older adults (≥65 years of age) in the United States is expected to double by 2050. 1 These individuals use acute illness care heavily, with 19.4 million emergency department (ED) and 94.8 million office visits for acute illnesses in 2010. 2,3 Providing timely acute illness care to this population is challenging and will only become more difficult unless innovative approaches for care are developed. 4 –9
Older adults experience barriers to obtaining acute illness care from their primary care physicians (PCPs), including difficulty obtaining timely appointments and convenient transportation. 4,10 –14 These barriers are particularly challenging for older adults who reside in senior living communities (SLCs), defined as independent and assisted living facilities, as their medical problems and functional limitations further impede access. 15 –18 Resulting delays may have serious consequences for time-dependent conditions, such as pneumonia. Delayed interventions may necessitate more intensive therapy or lead to increased morbidity or mortality. Access barriers may result in ambulance and ED use, which may be unnecessary or inefficient, especially for this population. 4,6,14
Health planners are increasingly searching for efficient ways to deliver acute illness care to vulnerable populations in a timely manner. 19 Telemedicine has been promoted as a mechanism to deliver acute illness care while reducing barriers associated with traditional care. Studies have shown that telemedicine decreases ED use and hospitalizations among other vulnerable populations, such as children and residents of nursing homes. 20 –23 No studies, however, have evaluated the effect of acute care telemedicine for community-dwelling older adults.
In this study, we evaluated the effect of our Health-e-Access, older-adult, high-intensity telemedicine program for SLC residents on the rate of ED use. 24 We hypothesized that access to these services for acutely ill SLC residents would decrease the rate of ED use, compared with a control cohort.
Materials and Methods
Study Design
We performed a prospective cohort study to compare the rate of ED use between subjects with the opportunity to use high-intensity telemedicine for acute illness care (intervention) and those who did not (control). This study was approved by the University's Research Subjects Review Board.
Study Population and Setting
We enrolled patients of a geriatrics practice that provides primary care to residents of 22 SLCs. The physicians and advanced practice providers typically provide in-person primary care services at each SLC twice a week. The practice has a separate administrative office staffed by nurses and advanced practice providers to handle administrative and clinical issues, including requests for assistance with acute illness care.
We selected seven SLCs to receive the intervention (access to the telemedicine program) to ensure a spectrum of participants and facilities as well as overall similarity in characteristics between the groups. Ownership at one facility subsequently declined to participate, so this facility was excluded from the analyses, leaving six active intervention sites.
Individuals were eligible for the intervention group if they were geriatrics practice patients and lived in an intervention facility. Patients were generally enrolled independent of emergency visits, such as during PCP visits. For patients without decisional capacity to provide informed consent, we approached the designated proxy for consent. The control group included all practice patients at the control facilities, as well as those patients at intervention facilities for whom we did not obtain consent.
We began following study subjects on May 1, 2010, allowing for at least 6 months of data collection at each intervention facility prior to program implementation. We used a staggered start approach, introducing the program at one facility at a time, which allowed for an interim qualitative evaluation to optimize processes. 25 The first facility started the program in December 2010, and the last facility began in August 2011. The study ended on November 30, 2013, but subjects left the study earlier if they became ineligible or died. We tracked exit from the study through billing data and medical records.
Potential sources of bias were managed through a variety of means. All subjects at intervention facilities were approached to participate using an established protocol, and, for those who initially declined, later enrollment remained an option. Subject enrollment was facilitated through an extensive educational and marketing process, so all subjects or proxies were equally aware of the program and their eligibility to participate, thereby minimizing selection bias. The primary outcome measure, ED use, was provided through medical and billing records and not subject to bias.
The Intervention
Intervention group subjects could use telemedicine for acute illness care. The Health-e-Access, older adult, high-intensity telemedicine program has been described in detail elsewhere. 24 In brief, we provided patient-to-provider, real-time, or store-and-forward telemedicine services. We consider this a “high-intensity” model because it (1) is assisted by a technician at the patient's side and (2) captures much more clinical detail than simple videoconferencing (Table 1). Telemedicine assistants were clinical technicians, similar to nurse's aides, who were provided supplemental telemedicine and geriatrics training and were employed by the program.
Services Provided by the High-Intensity Telemedicine Program
When an intervention subject felt ill, the subject or caregiver called the geriatrics practice for assistance. Services were available only during weekdays between 8 a.m. and 6 p.m. because most of the requests for care occurred during that period. Weekend services were pilot-tested but discontinued due to a lack of use. The responsible provider had the option of managing the concerns through traditional means (telephone, immediate outpatient visit, or ED referral) or through telemedicine. To support this decision, providers were given an orientation to the telemedicine program.
If the provider ordered a telemedicine visit, a telemedicine assistant went to the subject's residence and gathered illness history and specific clinical data based on established protocols. The telemedicine assistant then uploaded information to the electronic medical record (TeleAtrics, Allentown, PA) and contacted the designated telemedicine provider, generally from the geriatrics practice. The telemedicine provider reviewed the information collected by the assistant, communicated the assessment and plan with the subject and/or caregivers via telephone or videoconference, ordered testing or medications, and wrote discharge instructions. Testing could include imaging studies (e.g., radiographs and ultrasounds), which were performed by an independent company that provides such services to SLCs in the community.
Measures
The primary outcomes were rates of ED visits overall and ED visits categorized by disposition. We obtained records of ED visits and hospitalizations through a query of local hospitals' clinical and billing records. We also reviewed the geriatrics practice's clinical records for ED and hospital discharge reports.
Information on potential confounders was collected from medical chart reviews conducted when the subject entered and left the geriatrics practice and annually. We included six patient-level characteristics in the multivariable analyses: age, gender, race, SLC type (assisted or independent), advance directive choices, and Charlson score. Charlson scores, which are used to measure and adjust for the burden of disease among patients, were calculated using a self-report metric and dichotomized at the median (0). 26 Advance directives were categorized into “limited care” (yes or no) based on medical record documentation identifying patients who chose to receive limited interventions or comfort care or to not be hospitalized. Multivariable analyses also included two dichotomous facility-level characteristics: profit status and specialization in dual-diagnosis (medical and psychiatric) patients.
Statistical Analyses
Baseline patient and facility characteristics were summarized with descriptive statistics and compared between study groups using two-sample t tests or chi-squared/Fisher's exact tests. We used person-month as the unit of analysis, defined as the observation of a single subject during a given 28-day period. With each subject contributing multiple person-months, our analysis accounted for the clustered data structure within subject and SLC. Generalized estimating equations (GEEs) were used to estimate the effect of telemedicine on ED use rates by fitting marginal Poisson models. Telemedicine availability (intervention versus control), time from study enrollment (months), and the interaction of the two were included in the model as independent variables. The interaction assessed whether ED use rates changed differently with respect to time between the intervention and control groups. Stratified analyses were further performed to investigate how the ED use rates changed over time within each group.
Confounding variables at both the patient level and the facility level were controlled as covariates in the regression model. Person-months with missing data for covariates were excluded from the multivariable analyses. Sandwich estimators were calculated to provide robust estimation of standard errors. The advantage of the GEE method is that it provides consistent estimation even with a misspecified correlation structure. 27,28 To address the occasions that a subject entered or left the study in the middle of a month, analyses adjusted for actual days of the months when the subject was in the study. The analysis was limited to subjects who stayed in either the intervention or control group for at least 1 month. We also performed sensitivity analyses that excluded subjects who had the opportunity to, but did not, consent to the intervention. Results were converted to reflect reductions in use per year for ease of interpretation. Other ED use rates were analyzed similarly.
Results
We approached 705 subjects or proxies to consent for the opportunity to use telemedicine. Among these, 494 (70.1%) agreed, and 81 (11.5%) explicitly refused; the remainder did not provide consent because they lacked decisional capacity and no proxy could be reached. There were no differences in subject characteristics between these individuals and control subjects at the control facilities. After subjects who were followed up for less than 1 month were removed, 479 subjects were considered intervention subjects. They contributed 8,194 person-months to the analysis, whereas control subjects contributed 21,313 person-months. The groups were similar (Table 2) except a greater proportion of the intervention group resided in independent living facilities, which we controlled for in the multivariable models. The characteristics of the intervention facilities and control facilities were also similar (Table 3).
Characteristics of Subjects at Enrollment
Data are number (%) unless indicated otherwise.
For ADL deficiencies n=430 in intervention group and n=351 in control group (781 overall).
ADL, activities of daily living; AIDS, acquired immunodeficiency syndrome; DNI, do not intubate; DNR, do not resuscitate; HIV, human immunodeficiency virus.
Facility Characteristics
Data are number (%) unless indicated otherwise.
ED, emergency department.
During the study, 517 telemedicine visits were initiated (0.063 visits/person-month). Among these, the information collected allowed providers to make a definitive treatment decision for 503 (97.3%), and visits were completed by telemedicine (i.e., no immediate PCP or ED care was required) for 465 (89.9%). Of the 52 visits that were not completed by telemedicine, 19 (36.5%) resulted in immediate transfer to the ED. The remainder required in-person PCP follow-up within 24 h.
Control subjects visited the ED 2,238 times overall, with 1,058 (47.3%) resulting in discharge home, whereas intervention subjects visited the ED 725 times overall, with 315 (43.4%) resulting in discharge home. Overall ED use rates for intervention and control subjects were 0.089 and 0.105 visits/person-month, respectively (Table 4). GEE models that did not adjust for covariates showed that overall ED use was 16% less for intervention subjects than for controls (rate ratio [RR]=0.84; 95% confidence interval [CI], 0.73–0.97). The use for ED visits resulting in discharge home was 23% lower among intervention than control subjects (RR=0.77; 95% CI, 0.63–0.94).
Healthcare Utilization Rates Per Person-Month for Intervention Versus Control
Calculated using generalized estimating equations accounting for autocorrelation. No covariates were adjusted.
ED, emergency department; PCP, primary care provider.
Neither the rate of PCP visits (0.67/person-month for intervention versus 0.68/person-month for control subjects (Table 4) nor the mortality rate (0.65 deaths/100 person-months for intervention versus 0.68 deaths/100 person-months for control subjects) was significantly different between intervention and control subjects.
Table 5 shows the change in rate of ED use over time, stratified by intervention status, after adjusting for subject and facility characteristics. Among intervention subjects, ED use decreased at a monthly rate of 1.5% (RR=0.985; 95% CI, 0.973–0.996), which corresponded to an annual rate of 18% (RR=0.82; 95% CI, 0.70–0.95), whereas in the control group there was no statistically significant change in ED use over time (RR=1.01; 95% CI, 0.95–1.07). This between-group difference was statistically significant (p=0.009 for the interaction between intervention and time). Figure 1 further depicts this change over time in ED use. For ED visits resulting in discharge home, intervention group visits decreased at an annualized rate of 22% (RR=0.78; 95% CI, 0.63–0.97), whereas the rate of control group visits did not change significantly (RR=0.94; 95% CI, 0.88–1.02). The interaction effect between group and time was not statistically significant (p=0.130), however. The sensitivity analyses that excluded subjects who had the opportunity to, but did not consent, to the intervention yielded similar results (data not shown).
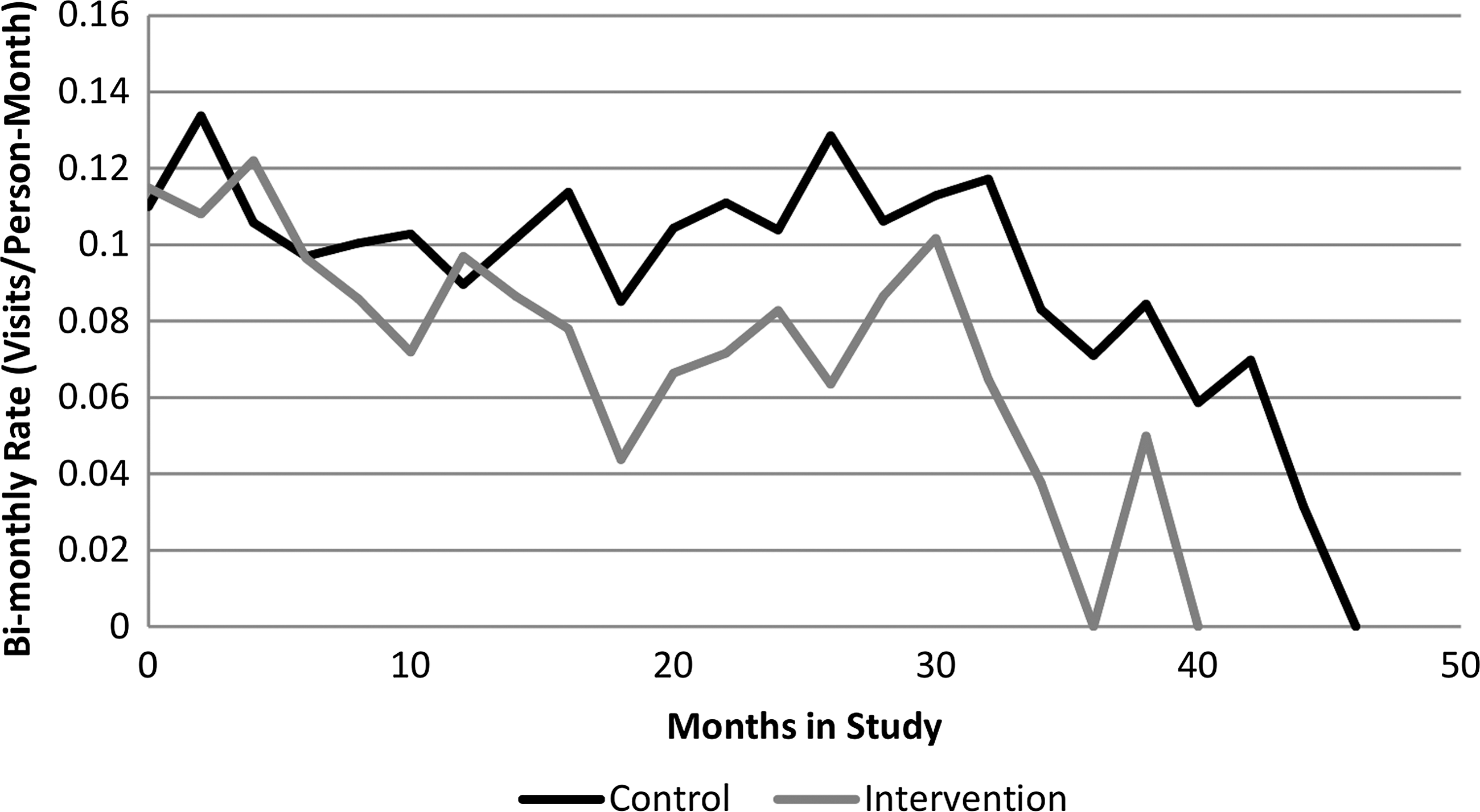
Rate of emergency department utilization over time.
Annualized Change in Healthcare Utilization
Estimations were based on generalized estimating equations to account for the clustering data structure. Adjustment factors were subject age, race, gender, Charlson score, residence type, care status, facility profit status (not-for-profit/for profit), and specialization in dual-diagnosis (medical and psychiatric) patients.
CI, confidence interval; ED, emergency department.
Discussion
This study is the first to demonstrate effectiveness of an acute care telemedicine program for SLC residents. Individuals with access to the program experienced a substantial decrease in the rate of ED use (18% over the course of a year), whereas those without access to our program experienced no change in the rate of ED use. Moreover, compared with controls, intervention group patients showed no difference in PCP visits or mortality.
Decreasing the rate of ED use may have important implications for quality of care for older adults. ED-based care can have negative consequences, particularly for nonemergency conditions. 29 –31 EDs exist outside patients' medical homes, thus creating discontinuity in care that can be problematic for medically and psychosocially complex older adults. 32,33 ED providers often lack complete patient histories, and patients frequently cannot contribute necessary missing information. 34 The typical ED environment is suboptimal, with excessive ambient noise and disruptions. 35 –37 ED care is also expensive, with the average payment of $1,062 for an ED visit for a discharged older patient, with an additional $429 payment for ambulance transport. 38,39 As provider organizations and health insurance organizations in the United States move to managing the health of populations and sharing financial risk, efficient strategies for providing timely acute illness care are increasingly recognized as important. 19 The financial status of these dominant health system stakeholders will be especially sensitive to costs of serving older adults, given the rapid growth and high morbidity rates of this population. Telemedicine models may enhance access to care while being cost-efficient.
The older adult Health-e-Access telemedicine program was structured to address many of these challenges and also keep the care within the patient's medical home, precluding problems that arise from multiple, disconnected caregivers. This and previous studies indicate that this program can meet both patient and provider needs, with 97% of telemedicine visits enabling providers to make treatment decisions and 90% of them being managed solely by telemedicine. Telemedicine provided sufficient information about the current illness and patient's history to make diagnosis and treatment decisions with confidence. 25 Furthermore, we have demonstrated acceptability of this care model to patients and caregivers, with 86.7% of patients and 97.2% of their caregivers indicating that they would choose an SLC with telemedicine over one without telemedicine. 24,25 These levels of acceptability, and the acceptability of telemedicine found in other studies, confirm that older patients are not resistant to or uncomfortable with this technology and that healthcare providers are not uneasy about caring for complex patients at a distance. 40,41
We believe that the observed annualized 18% decrease in the rate of ED use among intervention subjects is a conservative estimate. We only provided telemedicine services during limited weekday hours. Thus, intervention group subjects would have to go to the ED for care during the weekends and evenings, reducing the effect on the rate of ED use compared with an always-available telemedicine model.
Our findings are consistent with literature describing telemedicine interventions in other populations. Grabowski and O'Malley 23 recently showed that telemedicine reduced nursing home resident hospitalizations by 8%. Health-e-Access high-intensity acute care telemedicine reduced ED use among children in childcare and schools. 20 –22 Like the pediatrics studies, the overall use of services (ED, PCP, and telemedicine, if available) is slightly greater among our patients with access to telemedicine than those without (Table 4). 21 However, substituting high-cost services for lower-cost services should decrease overall costs of providing care. For SLC residents, many telemedicine visits could be performed for the cost of a single ED visit associated with ambulance transport. A formal cost-effectiveness analysis of this program, beyond the scope of this analysis, is in progress.
Given these findings and their consistency with findings of similar studies, policy makers should strongly consider integrating high-intensity telemedicine services for SLC residents into population health programs. With the demonstrated feasibility, acceptability, and decreased ED use, high-intensity telemedicine will only enhance value of care delivered to this vulnerable population.
This study has multiple strengths. It is the first study of its type. We leveraged the telemedicine expertise of the developers of a previously successful telemedicine program, as one would expect for an effectively implemented program. Additionally, our program was strongly integrated into the primary care practice and closely involved the PCPs, promoting successful implementation and increasing likelihood of sustainability. This close integration also allowed for thorough follow-up of study subjects. We did not rely purely on administrative data, and the frequency and timing of our chart reviews helped to ensure the timeliness and accuracy of the data.
This study also has some limitations. We may have failed to ascertain some acute care visits because urgent care centers did not consistently send medical records to the geriatrics practice. We do not believe that complete urgent care data would change our results, however, because urgent care was not widely available when the study started, and it was available equally to both control and intervention groups. For ED use, only one area hospital failed to provide administrative records. Based on referral patterns, few subjects would have gone to this hospital, and visits likely would have been captured via review of geriatric practice charts. This study was not a randomized clinical trial; however, this was not feasible in this population and setting. With such a small number of facilities and specialization within facilities, our purposive sampling ensured balance between and diversity within groups, which group randomization could not do. Additionally, our comprehensive collection of covariates allowed for adjustment for possible confounders. Our subjects were SLC residents; thus, our findings are not generalizable to all older adults. 16,17 Finally, these findings do not imply that other types of telemedicine are necessarily associated with reduced ED use. A lower-intensity telemedicine model was not evaluated and seems unlikely to have the same impact.
Conclusions
This older adult Health-e-Access high-intensity acute care telemedicine program significantly reduced ED use among SLC residents with access to telemedicine without increasing PCP visits or mortality. This innovative alternative to traditional acute illness care can enhance access to acute illness care for this vulnerable and growing population, supporting its integration into population health programs. Further analysis is necessary to assess the benefits and cost-effectiveness of this program.
Footnotes
Acknowledgments
This study was performed at the University of Rochester School of Medicine and Dentistry, Rochester, NY. This project was supported by grant number R01HS018047 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.
Disclosure Statement
K.M.M. and N.E.W. were eligible to receive royalties while this research was active from Trifecta Technologies, which develops and maintains the software used in the study. They were no longer eligible to receive royalties as of December 31, 2013. M.N.S. was a consultant to Fortress Investment Group and one of their companies, Lifeline2Care, which was, but no longer is, developing a senior living community telemedicine model. E.B.W., H.W., S.M.G., K.N., D.N., and A.D. declare no competing financial interests exist.