
Abstract
Introduction
Apple (Cupertino, CA) introduced HealthKit and the Apple Health application (app) in 2014. HealthKit is an aggregator of personal medical information, and the Apple Health app facilitates data transfer into HealthKit. The Health app allows users to manually enter medical information such as weight, blood pressure (BP), glucose, sleep time, and steps, or the app can pull the same information wirelessly from multiple self-monitoring devices.
The Apple Health app combined with the iPhone® (Apple) appears to offer some advantages that may be hard to duplicate with other platforms. One of Apple's advantages is that its Health app is pre-installed with iOS 8 updates and is compatible with iPhones 4S and higher. 1 HealthKit can also acquire medical information from electronic medical records. Mayo Clinic and other healthcare institutions have partnered with Apple in the use of the HealthKit platform. 2,3 For iPhones with the Mayo Clinic Patient App loaded, the Apple Health app can automatically load the Mayo Clinic as a data “source” just like it does for self-monitoring apps. However, the “source” data are BP, weight, heart rate, and other data extracted from the Mayo Clinic electronic medical record.
Because Apple's Health app comes pre-installed on a major mobile platform, the iPhone with HealthKit and Health app may be a telemedicine disruptor as predicted by Doarn and Merrell. 4 With the potential for out of the box telemonitoring available to all iPhone users, Apple can disrupt an existing middle layer of telemonitoring services, hubs, and servers.
Apple's software may fill an existing gap between unstable patients who require dedicated telemonitoring services and those interested in a “quantified self.” Quantified self-users can be very healthy people who use telemonitoring to track their steps, flights of stairs climbed, sleep time, and calories. 5 At the other end of the spectrum are patients with difficult-to-manage chronic disease who need dedicated telemonitoring services to provide a steady stream of data to their healthcare providers; these patients often benefit from telemonitoring. 6 –9 In between these extremes are the large numbers of patients who are taking medications for milder forms of hypertension, diabetes, asthma, and depression and who only need intermittent follow-ups and medication adjustments for their BP, glucose, peak flows, and mood. These are patients well suited for HealthKit: they do not need continuous telemonitoring, but they do require more than just self-monitoring for motivational feedback.
The objective of this study is to determine how many patients have and are willing to connect Apple's HealthKit with their electronic medical record and, of those, who might benefit from intermittent follow-up for milder forms of chronic conditions. In addition, we examine continued barriers to the use of this technology.
Materials and Methods
We used a primary care database of the Mayo Clinic, Rochester, MN, to identify patients with hypertension, diabetes, depression, and asthma. Patients who had registered with HealthKit were matched to the primary care database. We also used Mayo Clinic electronic medical record information about the patients' last BP, glucose, cholesterol, hemoglobin A1C, and statin use. Data collection concluded in February 2015, just a few months after Apple's introduction of HealthKit in 2014; there was no organized effort to have primary care patients register with HealthKit. We used JMP version 11.0 software (SAS Institute, Cary, NC) for statistical analysis.
Patients join HealthKit by signing in to their Mayo Clinic Patient App and responding to the HealthKit invitation (Fig. 1). Patients give permission to share data by individual parameters (Figs. 2 and 3).

Mayo Clinic Patient Application with invitation to share data with Apple HealthKit.
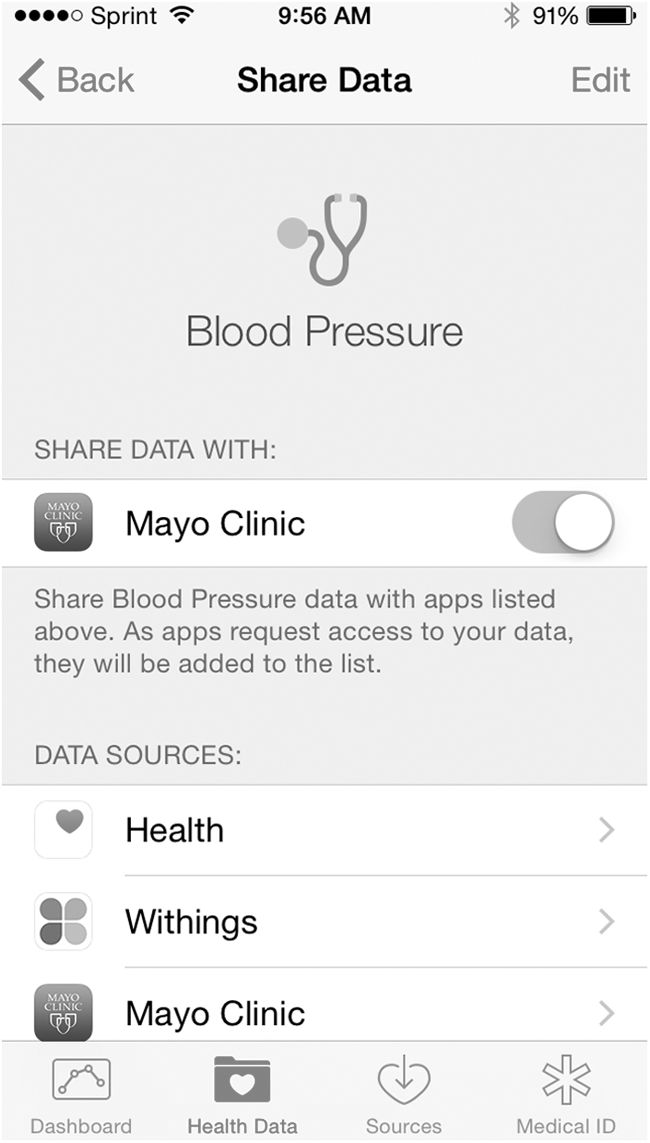
Share Data screen of the Apple Health application.
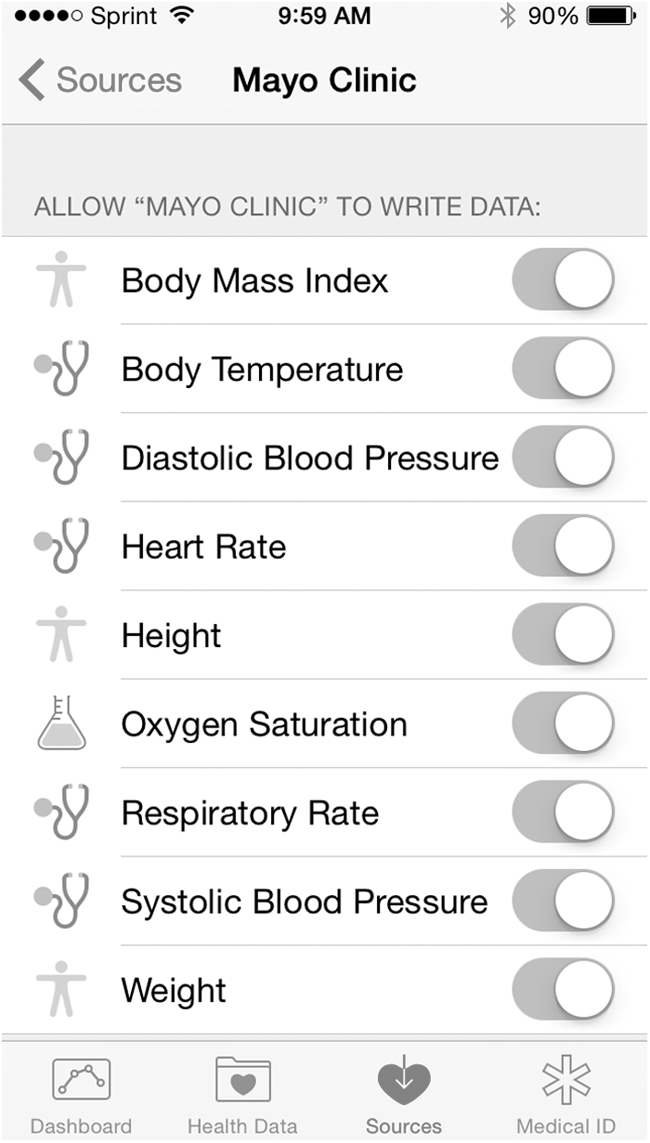
Apple Health application screen to allow Mayo Clinic medical record data transfer to HealthKit.
This study was approved by the Mayo Clinic Institutional Review Board.
Results
After 7,048 of the 105,199 adult patients in our primary care registry who did not give universal research authorization were excluded, 98,151 patients remained for our analysis. Of those 98,151, there were 503 who had registered with HealthKit.
Primary care HealthKit registrants compared with others in our primary care panel did not have large differences in proportions of many telemonitorable conditions even though they were generally younger (Table 1).
Adult Primary Care Telemonitorable Condition and Demographic Comparison by HealthKit Registration
Data are percentages (n).
Ho: HealthKit registration has the same result as not registering for HealthKit. By Pearson's chi-squared test.
BP, blood pressure.
Figure 4 is the Health App showing a patient's BP from Mayo Clinic records merged with patient sources (Withings [Issy-les-Moulineaux, France] BP cuff automatic entry and self-entry via the Apple Health app).

Apple Health view of blood pressure data from multiple sources including home (Withings Health Mate, Apple Health) and Mayo Clinic.
Discussion
Owners of iPhones are using HealthKit to connect to their medical record (Figs. 1 and 2), and 49% of these users have conditions or predispositions that could benefit from telemonitoring (Table 1). Table 1 shows that HealthKit registrants had a younger age distribution than others in our primary care panel, but they still had significant conditions of hypertension, asthma, diabetes, and depression. Our study demonstrates that primary care HealthKit registrants need follow-up glucose readings, BPs, mood parameters, and peak flows and that they already own a platform (iPhone) to enable telemonitoring. In addition, these registrants rarely have extremely high BPs or hemoglobin A1C levels over 9.5% (Table 1), so they may not require intensive telemonitoring.
Cost of telemonitoring devices may not be a major barrier to iPhone users. The Apple list price of the iPhone 5 and 6 lowest memory units (8 and 16 GB) are $450–$749. 10 With cellular contracts from $50 to $80 monthly, phones can be purchased for less ($100–$200). 11 Automated BP monitors range from $35 at Costco 12 to $130 (Withings) 13 with the ability to enter BPs directly to Apple HealthKit. With disposable income to support an iPhone and mobile data services, the one-time cost of a BP monitor appears to be a small cost barrier by comparison. Patient education barriers to telemonitoring are also minimized by iPhone-savvy patients who already understand their own iPhone well enough to load the Mayo Clinic Patient App and register to share information with HealthKit.
Registered HealthKit patients are connected to Mayo by a telemonitoring hub (iPhone) and patient online services (Mayo Clinic App/Portal). Similar services through a telemonitoring service would be $30–$50 monthly plus additional upfront equipment costs. 14,15
CONTINUED BARRIERS TO HEALTHKIT
HealthKit registrants literally have technology in their hands to connect data directly to their Mayo Clinic primary care providers. Their iPhone is their telemonitoring hub already activated and functioning, connecting them to Mayo Clinic data. Despite that, there are continuing barriers to this technology. Lack of reimbursement for telemonitoring continues to be a barrier, and restrictive regional quality measures can hamper telemonitoring. 16 Interoperability and governance issues also complicate transfer of telemonitored data into the medical record. 17
HealthKit does not solve the interoperability and governance issues. Figures 4 and 5 show the differences in BP-related data in HealthKit from the Mayo Clinic and from a Withings BP cuff that uploads data via the iPhone. HealthKit does not show important associated BP data such as patient position (seated/standing), and the Mayo Clinic has not yet created an interface allowing providers to see their patients' HealthKit data. Determining what data to upload into the medical record, where to put it, and what metadata to include are ongoing governance challenges. To date, patients can pull Mayo Clinic source data into their HealthKit (Fig. 4); however, they cannot yet push their HealthKit data to their Mayo Clinic provider, and governance issues are partly responsible. Adult BP readings at Mayo Clinic are obtained in a standardized way with calibrated automatic arm cuff BP monitors. However, patients at home may be using wrist or finger monitors, which may have less validity. 18 HealthKit captures the exact type of device (Fig. 5), but with so many different devices, there are continuing challenges with inserting data from these different devices in the medical record. A significant number of patients monitoring at home may be using a less valid device such as a wrist BP monitor. 19 Because of these differences in validity such as seen with the finger and wrist BP monitors, 18 data governance is needed to help differentiate incoming telemonitored data by validity and other criteria.
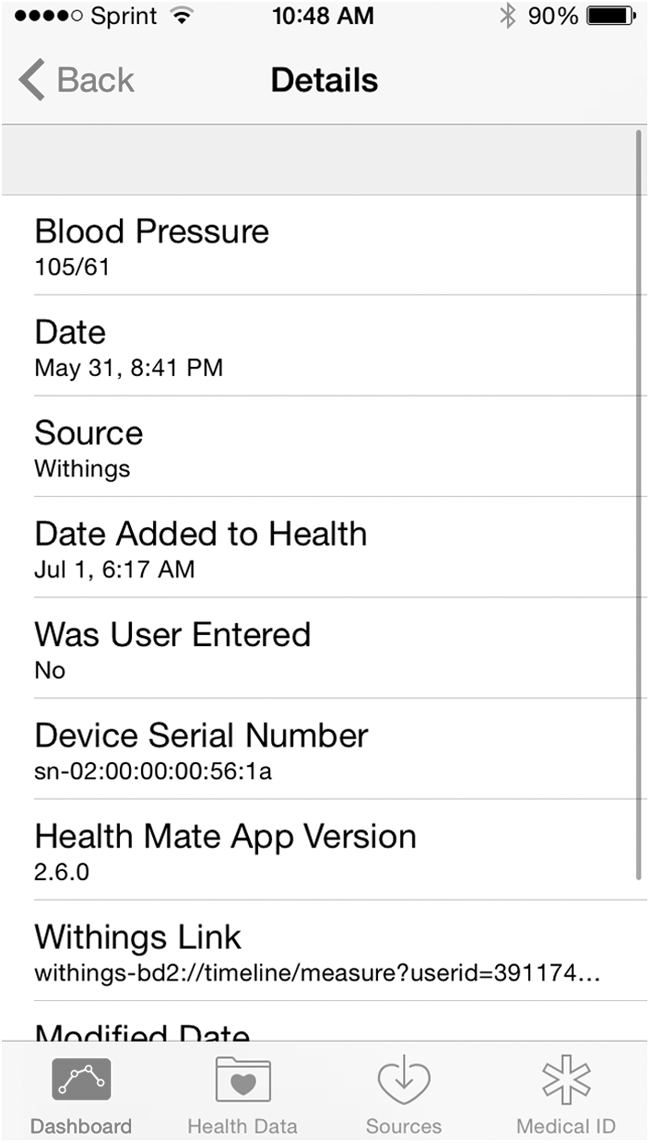
Apple Health view of a single blood pressure record pulled from the Withings Health Mate Application.
Providers also are not uniformly enthusiastic about this technology. Much like with the introduction of secure messages, 20 providers are concerned about the volume of data they will need to address. Patients are already sending dozens of BP readings in individual secure messages, 21 so providers are concerned about receiving masses of unfiltered BPs from Apple HealthKit or other mobile platforms. Filtering and summarizing BP data are being addressed in the informatics community, 22 but it may take some time for providers to reach a comfort zone in data filtering. Primary care also needs processes to change treatments based on the telemonitored data. If the telemonitored data indicate high BP that needs treatment modification, then there needs to be a process to contact the patient and change antihypertensive medication dosage or prescribe an additional antihypertensive. Nurses and pharmacists have developed processes to do this, 14,23 –25 but there will need to be more widespread integration of these processes in primary care for telemonitoring to be successful.
HEALTHKIT ADVANTAGES
The Apple HealthKit can offer significant advantages. To date, telemonitoring technology has generally been associated with monthly service fees and an upfront cost of a hub and monitoring devices. 14 The iPhone with pre-installed health app software can replace the typical expensive telemonitoring infrastructure of a hub and server. Software updates and installation are eliminated by the free, automatic install of the Apple Health app with every iOS update. Patients can also use a peripheral device of their choice such as a BP monitor that they may already own. Use of their own familiar devices can maximize patient uptake and engagement, while reducing the telemonitoring cost for the healthcare institution. Finally, for primary care providers whose patients now send them highly unstructured telemonitoring data by secure message, 21 a change to structured data from HealthKit could improve care.
Conclusions
The Apple HealthKit telemonitoring platform offers advantages over current hub-and-server technology for a segment of the primary care population. Although this easily accessible telemonitoring platform has distinct advantages in terms of widespread dissemination, as well as a population with conditions amenable to telemonitoring, there remain interoperability and data governance issues, reimbursment barriers, and provider concerns about the potential for large amounts of unfiltered telemonitoring data.
Footnotes
Disclosure Statement
Both of the authors are shareholders of Apple Inc.