
Abstract
Introduction
Pedometers are considered desirable devices by the medical community, due to their affordability and because they can be used to easily assess the level of personal physical activity (PA). 1 Many of these devices have emerged on the market during the last years, but, despite this growth, many of them do not match the expectations of physiologists. Two population groups where walking problems have been observed are patients having undergone surgery in the lower extremities, or who are otherwise weakened through disease, medical treatment or surgery procedures, 2,3 and the senior population with slow walking speeds. 4 As for the first group, it is desirable to check the patient's adherence to the prescribed recovery activities, which sometimes are provided by public or private health organizations after hospital discharge. 5 For some conditions, like patients having undergone surgery for extremity sarcoma, the rehabilitation process requires a combination of physiotherapy with the patient's self-training efforts performed in an unsupervised environment. 6 As for the second group, it is well known that the number of senior citizens in the general population is increasing 5,7 and that PA can improve their life quality.
For both populations any speed below 0.9 m/s (around 3.24 km/h) is considered a slow walking speed. 4,8 –11 These speeds can be observed, according to Chandra and Bharti, 12 in about 2% of the population, specifically in children, seniors, 11,13 and persons with some sort of disability or condition. 14,15 In seniors and persons with some sort of condition, slow speeds are observed because degradation of the muscles occurs, either by physiological and neuromuscular degradation or by medical intervention. A recent review 16 on gait speed in ambulant older people in long-term care reported gait speed between 0.5 and 3.3 km/h. Studenski et al. 17 reviewed nine studies with mean gait speed between 2 km/h to 4.3 km/h that had participants with a mean age of 73.5 years who were followed up for 6–21 years. In the elderly, it was observed that reductions in the hip range of motion and plantar flexor kinetics are the main causes for the slow speed, 18 which may indicate a reduction on the acceleration on the upper extremities of the limbs, making a step detection based only on acceleration more complex. Park et al. 10 suggested that for slow speeds there might not be enough vertical acceleration (0.30 g) to exceed the minimum acceleration threshold of most piezoelectric accelerometers. As most of the accelerometers available on the market are of this type, this may represent a general issue with most pedometers based on this technology. Another challenge in designing accelerometer-based devices is how to differentiate a step from other activities of daily living such as sitting, climbing stairs, or involuntary movements.
The majority of the available pedometers and research algorithms are based only on accelerometer data, with very few studies focusing on algorithms based on other sensors, like gyroscopes, 19 or on sensor fusion (e.g., combining several sensor types to increase precision and accuracy). On the commercial devices, we believe that some of the reasons for only using accelerometers are mainly related with the economic and energetic costs of having multiple sensors, as for normal speeds an accelerometer-based pedometer appears to have a good performance. Limited research efforts have been reported on sensor fusion, but interest may start to rise due to the availability of a range of sensors in small devices, like the Shimmer3 (SHIMMER Research, Dublin, Ireland) and on smartphones. Regarding the latter, there has also been a growth on software-based algorithm development. 19 –24 This may be due to two reasons: first, due to their wide availability and usage, and, second, it is quick and easy to develop applications due to the presence of many sensors and the associated application program interface (API) in most contemporary smartphones.
There has been a consistent number of studies on pedometer accuracy and usages, especially the ones done by Bassett and his co-workers 25 –28 and, for slow walking speed, most of them report problems. 10,11,25,29 Two of the reasons pointed out are (a) the type of sensor used, with some publications focusing on the discussion between the use of piezoelectric accelerometers or microelectromechanical systems accelerometers, 30 and (b) the use of techniques to filter false-positive steps, which in some cases might incorrectly filter not so well-defined steps. Usually, step detection is done in gait analysis studies by identifying different stages of a step (i.e., toe-off, heel-strike, and/or midswing 31 ) using adaptive or static threshold-based methods, based on the acceleration or frequency content of the signal. 32 These methods detect the gait events when the induced acceleration crosses the threshold values defined for these gait events.
There are also studies that focus on how pedometers can be used to assess PA. These studies are usually based on step counting and on an estimate of the distance that a person walked. Also, the number of studies that have used these populations is limited. From the selected bibliography for this study, only three studies 4,11,33 used a senior population to assess the performance of pedometers. Other limitations that are pointed out in these studies are (a) the necessity to assess the accuracy of the available pedometers (i.e., what is the error rate of the devices when counting steps), which can be directly related to the calculation of other metrics, such as the distance walked, (b) the participants of the study usually go for a free walk, and the selected speeds are subjective to what that person considers a slow, normal, or fast pace, and (c) the participants usually are young and do not have any physical disabilities.
The aim of this study is to evaluate three commercially available pedometers—the Fitbit (San Francisco, CA) Zip (FB), the Omron (Kyoto, Japan) HJ-720 (OM), and the Yamax (Tokyo, Japan) Digi-Walker® SW-200 (YM)—at slow walking speeds, specifically 1, 2, and 3 km/h (respectively, 0.28, 0.56, and 0.83 m/s). The main contributions of this article are (a) an analysis of the step count accuracy of three pedometers focusing on slow walking speeds, (b) an analysis of the FB step count accuracy, as there is little existing research on the usage of this device, and (c) to raise awareness for the necessity of focusing research and development on new devices and algorithms for the populations where slow walking speeds are common, as they can be a feasible solution to monitor PA and improve life quality.
Materials and Methods
Participants
The participants in the present study were 14 young people (9 males and 5 females) 29.93 ± 4.93 years of age, without any known physical disabilities. All the participants were either students or employees at the Department of Engineering at Aarhus University, Aarhus, Denmark.
Instruments
The instruments evaluated were mechanical (YM) and piezoelectric accelerometer (OM and FB)-based pedometers that were bought through online retailers. The instruments used are described below. We chose the YM and OM pedometers because they have been widely used in previous studies and the FB because the amount of research is more limited and no significant results for slow walking speeds could be found. The price of each of the devices was less than $100.
YM
The Yamax International Company presents a range of step counters branded as Digi-Walker that can provide metrics such as activity time, distance, and calorie consumption, based on step counting. The devices differ on the number of features they provide, but all of them share the same spring mechanical system. The Digi-Walker used on this test, the Digi-Walker SW-200, is the simplest one, which can be used only for step counting. The device has a spring-suspended mechanism that counts a step when a lever arm closes an electrical circuit. The arm needs a minimal force of 0.35 g to move. Compared with a piezoelectric accelerometer, this resembles the behavior of a simple threshold algorithm, where an acceleration value is either above or below a threshold.
OM
Omron provides a series of devices based on digital accelerometers that can be used to track many parameters based on the step counting. This specific device can provide feedback on the number of consumed calories and the walking distance. It can be worn on the waist or shirt pocket, around the neck, or in a bag, and it has Omron-proprietary Dual-axis technology that allows the device to work either vertically or horizontally. The device allows introducing the user's weight and stride length; the device's manual indicates the user should perform a 10-step walk to get the average stride length. It is not clear if these metrics are part of a calibration process. The pedometer's data can be downloaded to a companion application through an USB cable that provides extra feedback besides the step counting.
FB
Fitbit Inc. provides a series of wireless activity monitors that can be used to track PA (exercise and walk), sleep, and food habits. The sensors are provided in two formats: bracelets (Fitbit Flex, Fitbit Charge, and Fitbit Surge) and small dongles (Fitbit Zip and Fitbit One). They all share the same electronic architecture 34 –36 (i.e., an ARM Cortex M3 and an unidentified accelerometer); some of the more advanced devices provide extra sensors besides the accelerometer, which may be used for more advanced vital measurements. The Zip is the simplest of all devices offered by Fitbit and provides feedback on the steps, calories, and traveled distance. It can be worn on the waist, pants pocket, or chest. The acquired vital signs can be downloaded through Bluetooth® (Bluetooth SIG, Kirkland, WA) Low Energy to a computer and be synchronized to a Web service provided by Fitbit that reflects the PA habits. Third-party applications can access a Fitbit user's data using Fitbit's API.
Protocol
Each participant was measured for weight, height, and stride length. The participants wore the pedometers on the waist belt according to the manufacturer's instructions, and they walked on a treadmill wearing their own usual walking shoes. One hundred steps were walked four times at each of the walking speeds of 1 km/h, 2 km/h, and 3 km/h. At each of these walking speeds, in the first set of four trials the participants wore the YM and FB, and in the second set of four trials the participants wore the OM.
The participants climbed on the treadmill while the treadmill was stopped wearing the YM and FB on the left and right side of the waist belt, respectively, spaced symmetrically about 4–5 cm on either side of the navel. The participant started the treadmill, set the walking speed to the desired one, and then walked 100 steps that were manually counted by the participant and the facilitator. When the 100 steps were completed the participant stepped on to the sides of the walking belt of the treadmill and had a break. Meanwhile the step counts were recorded on paper and spreadsheet by the facilitator. After the break the participant stepped on the walking belt and repeated the 100-step walking trial three more times following the procedure described above for the first trial. Once the set of four walking trials at a particular walking speed was completed, the participant stopped the treadmill, the YM and FB were removed from the waist belt, and the participant wore the OM on the right side of the waist. The participant again started the treadmill, set the speed to the desired one, and repeated the 100-step walking procedure described above, always stopping after 100 steps in order to record the number of steps indicated by the pedometer. After the participant completed four trials of 100 steps each with the OM at a particular speed, the treadmill was switched off, and the participant removed the OM. This 100-step procedure wearing the YM, FB, and OM was done for the desired walking speeds of 1 km/h, 2 km/h, and 3 km/h.
We chose speeds below 0.9 m/s (around 3.24 km/h) as any speed below this is considered a slow walking speed, 4,8 –11 with the first be an extreme case, but still observed in some situations, 16 and the others being more common, namely for populations with gait problems.
Statistical Analysis
Descriptive statistics of each sample were calculated using Matlab (version R2013a; The MathWorks, Natick, MA) and Microsoft (Redmond, WA) Excel®. The pedometer-measured step counts were tested for normality using a Kolmogorov–Smirnov test. As the data were not normally distributed, a chi-squared test was performed to compare counts among the pedometers, as well as to compare observed counts with the expected manual ground truth counts. Bland–Altman plots were used to show the agreement differences among the devices in more detail.
Results
The results of the evaluation are presented in Table 1. For each pedometer the average of counted steps by the device, its standard deviation, and the error percentage (i.e., the percentage of missed steps) are presented. The manual counting disagreement between each of the participants and the facilitator was 1% (disagreement of 1 step in 100). In cases where a higher disagreement was verified, the counting was discarded, and the walk was repeated.
Step Counting Results for the Three Devices, at Different Speeds
The results are presented as average of steps counted (AVG), standard deviation (SD), and error rate (ERR).
FB, Fitbit Zip; OM, Omron HJ-720; YM, Yamax Digi-Walker SW-200.
The error percentage [ERR (%)] was calculated with Eq. 1:
where ES is the number of expected steps (100 in this study) and CS is the average number of counted steps by the pedometer.
A graphical representation of the results is depicted in the box plot of Figure 1. The length of the whiskers is in the original interquartile range. Figures 2 and 3 depict the degree of agreement between FB and OM measurements at 1 km/h and 3 km/h, in order to clarify the differences between these two devices, which is not totally perceivable from Figure 1.
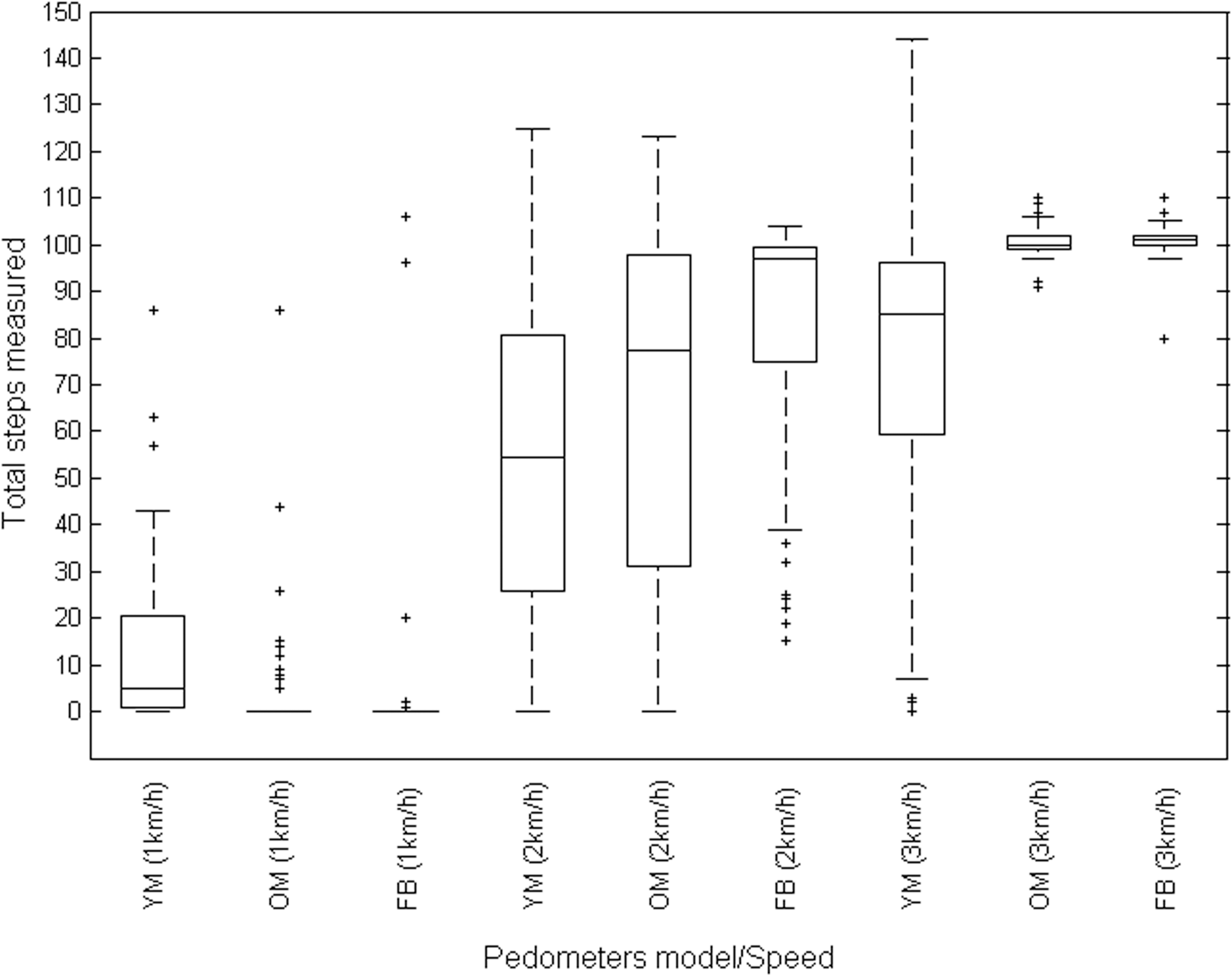
Box plot of the step measurements recorded by the Yamax Digi-Walker SW-200 (YM), the Omron HJ-720 (OM), and the Fitbit Zip (FB) at treadmill walking speeds of 1, 2, and 3 km/h.
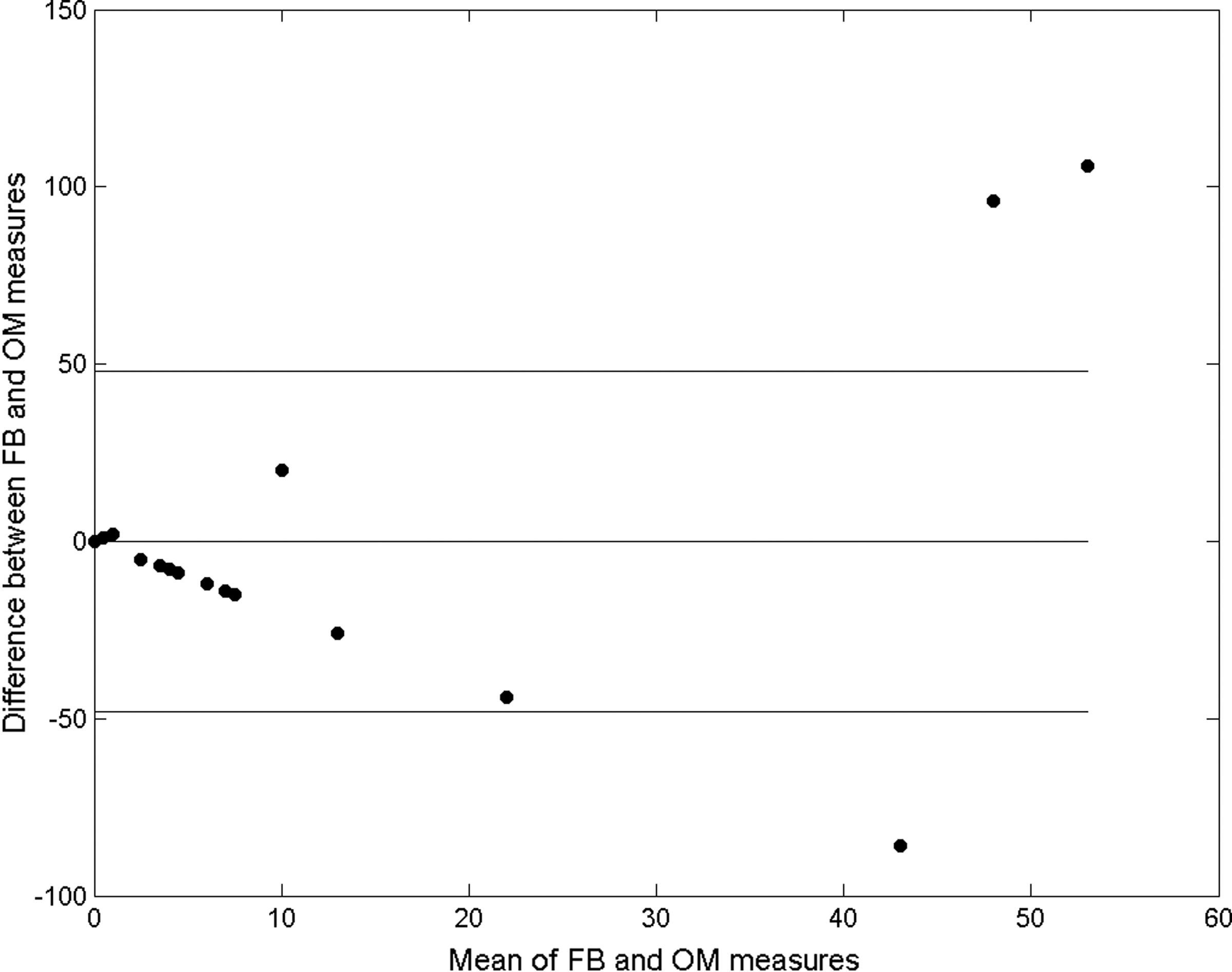
Bland–Altman plot of limits of agreement in measurement between the Fitbit Zip (FB) and the Omron HJ-720 (OM) at 1 km/h.
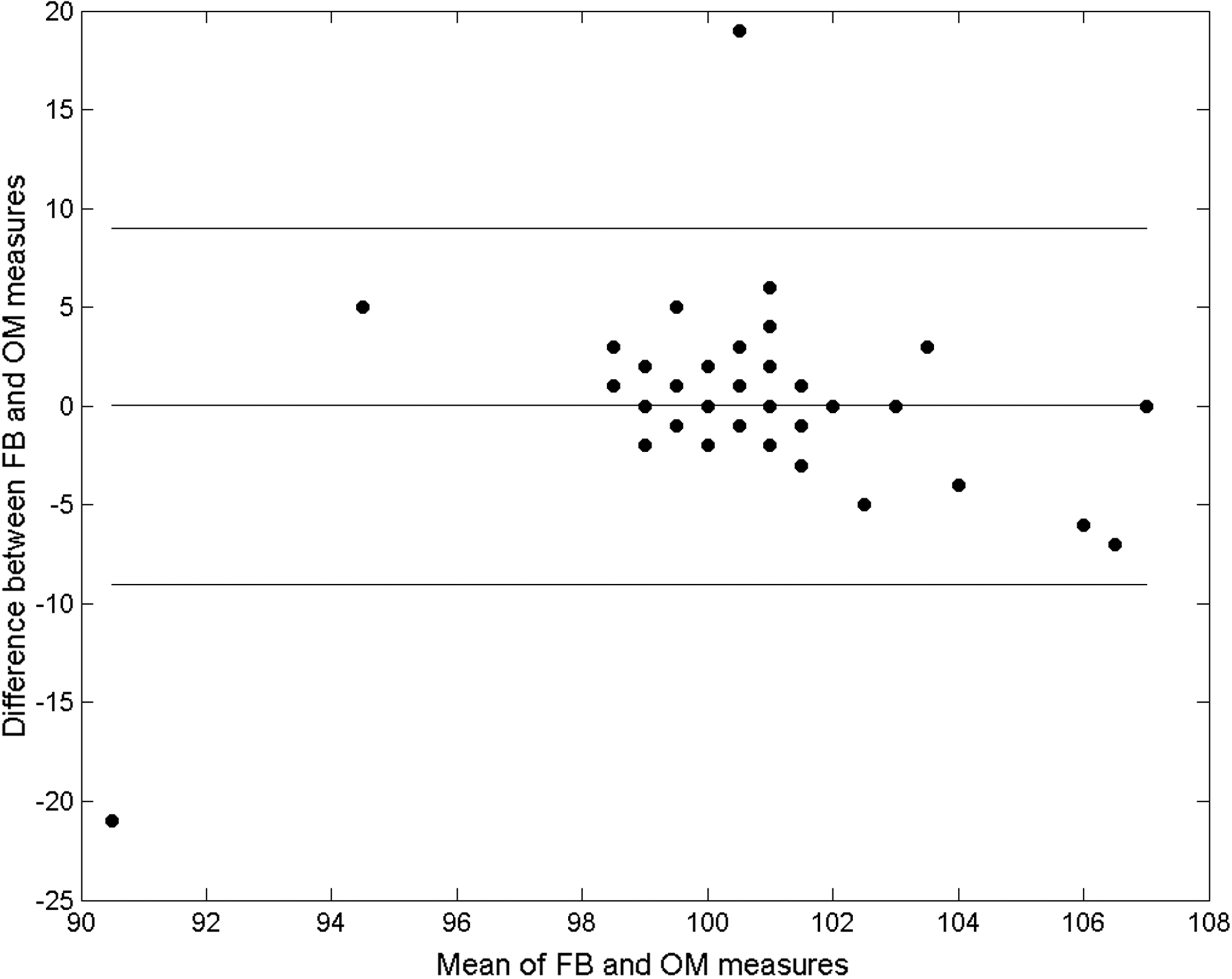
Bland–Altman plot of limits of agreement in measurement between the Fitbit Zip (FB) and the Omron HJ-720 (OM) at 3 km/h.
A statistical analysis on the count similarities between the devices was performed. For that a chi-squared test was used. Usually, an analysis of variance test is used on these kinds of studies to analyze the agreement between the measurements. But, the results of the Kolmogorov–Smirnov test showed that none of the step count sample sets is normally distributed, which is a requirement for analysis of variance. Because the sample size in this study is small (i.e., 14 persons), we cannot assess confidently whether the sample is normally distributed.
We started by testing two hypotheses between all three devices: • H01: All devices count steps with the same accuracy. • H02. All devices count with an accuracy of 100% (ground truth of 5,600 steps).
(This ground truth value is the number of steps of all participants for a single speed [i.e., 14 participants walked for a total of 400 steps at each speed].)
For a confidence level of 99.99%, the null hypotheses H01 and H02 were rejected at all speeds. In order to clarify why, the same chi-squared test was performed by pairing the devices. Two new null hypotheses were formulated: • H03: Both devices count steps with the same accuracy. • H04: Both devices count steps with an accuracy of 100% (ground truth of 5,600 steps).
At the same confidence level of 99.99%, H03 was accepted for OM and FB at walking speeds of 1 and 2 km/h. Hypothesis H04 was only accepted for OM and FB at 3 km/h; for all other pairs it was rejected.
At 1 km/h, referencing Figure 1, YM counted very few steps (mean = 12.89 steps, median = 5 steps), which indicates a low accuracy, whereas OM (mean = 4.04 steps, median = 0 steps) and FB (mean = 4.02 steps, median = 0 steps) did not count the majority of the steps, indicating poor accuracy. For the last two devices it is worth noting that on some occasions the devices may count some steps, although no reasoning about it could be made. We hypothesize that a reason for the different counts among devices may be due to the different physical constructions of the devices: the YM is a mechanical spring-based mechanism, whereas the OM and FB are piezoelectric based. This is also evidenced by assessing the similarity of the counting accuracy between device pairs where the digital accelerometers agree between them (p > 0.01), but the YM does not agree with either the OM or FB (p < 0.01). In order to make the comparison between the OM and FB clearer, the Bland–Altman plots in Figures 2 and 3 show that the level of agreement between the devices is low.
At 2 km/h the error rate of all three devices decreased, especially with regard to the FB; its error rate decreased from 95.98% to 17.27% (mean = 82.73 steps, median = 97 steps, error = 17.27%). Despite that, there is a big difference on the counts among the three devices, with none of them agreeing (p < 0.001). Also, the OM (mean = 65.66 steps, median = 79, error = 34.34%) and FB do not agree on their counts (p < 0.01), making the hypothesis that digital-based devices count in a similar way questionable. We hypothesize that this is not related with the accelerometer itself, but with the device's algorithms and the filter techniques that might be used. The OM starts counting after 4 s, as indicated on the device's manual, but for the FB it is unknown if any technique of this kind is used. Our evaluation has a small population, and it is difficult to conclude how the pedometers would perform in the long term (i.e., if the step counting values would improve at longer ranges [e.g., 1,000 steps or more]).
At 3 km/h we start seeing that the performance of the devices increases in accuracy, as seen in previous research. Again, a big difference among the YM (mean = 77.54, median = 85, error = 22.46), OM (mean = 100.63, median = 100, error = −0.63), and FB (mean = 100.70, median = 101, error =−0.70) is indicated. Despite the differences, OM and FB have again a high agreement level (p > 0.01), although counting agreement among the three devices is again not observed (p < 0.01). At this speed, the digital devices overcount rather than undercount steps, but this could be a result of the manual count agreements having a difference of 1%, as previously discussed.
Discussion
Comparison with Previous Studies
A survey on previous research in step counting evaluation was carried out as part of this study. Of the three selected devices, the YM is the most evaluated device, with nine studies, 4,11,13,28,29,33,37 –39 whereas the OM is present in three studies 28,29,38 and the FB in seven studies. 37,40 –45 In the previous research, only a few studies 4,11,13,29,33,38,40 evaluated pedometers at slow walking speeds. In some of them 4,11,13,33 the evaluation was made using a senior population; others 29,38 used a younger population, and only the walking speed of 3.24 km/h can be used for comparison, despite being slightly higher than the limit velocity of our study. Giannini 40 used two populations, one of children and the other of adults, with slow walking speeds observed in both groups. Six other studies 28,37,39,41,43,46 either did not provide enough data about the population used, or the walking speeds do not match the ones of the present study (i.e., they are above 3 km/h), making a comparison unfeasible. We also found some lack of standardization of the presentation of the results; therefore we opted to compare the results from these studies based on the error rate of the devices, which we believe is a better comparison-metric across studies.
The accuracy of spring-based accelerometers, like the YM, has been highly researched, 4,13,25,29,33,38,47,48 with most studies pointing out that these type of sensors are not reliable for all types of situations and users and are especially faulty at slow walking speeds, usually undercounting steps, in accordance with our findings. Due to the amount of available literature with step counting data with the YM, a comparison can be made, despite the different conditions and where the tests were performed. The trend for a higher accuracy with the increase of speed was observed, and the error rates are also similar, based on the differences given by the standard deviation. As an example, for 2 km/h our error rate was 46.46 ± 32.37%, whereas Cyarto et al. 4 reported the error rate for a walking speed of 2.3 km/h (0.64 m/s) as 55.10 ± 37.80%. The confidence intervals for these error rates would be (14.05; 78.83) and (17.30; 92.90), respectively. The two intervals meet for most of the values, which shows that different populations and different conditions may be comparable. It is important to note that the devices, in both studies, are worn on the waist belt, which is not affected by physical limitations as the lower limbs. We suggest focus on comparing devices between different populations because other studies show that there are physical differences among the populations, which might affect the counting accuracy.
Previous studies evaluating OM's accuracy for slow speeds were hard to find, with only three studies 25,29,38 offering results on the speed of 3.24 km/h. A comparison among these studies does not offer many conclusions, and our study does not provide sufficiently clear results that this device is reliable at slow walking speeds. Also, the statistical analysis does not permit us to do comparisons with any of the three devices at 2 km/h, as the counting among them does not agree (p < 0.01). We suggest that more research on the OM device must be conducted if it is intended to be used by the studies' target populations.
To our knowledge this is the first study where the FB step counting accuracy is evaluated at slow walking speeds. The majority of the referenced studies where the FB was used tend to focus on the PA and energy expenditure validity. Tully et al. 44 compared the FB with the Actigraph (Pensacola, FL) GT3X to count the steps as a measure of free-living PA and found that the FB appeared to count significantly more steps compared with the Actigraph. A direct comparison between our study and the remaining ones is unfeasible because part of the data used for comparison is missing or the device was assessed for different speeds than the ones used in our study. Despite that, it is important to note that our results can provide some insight into other studies because the step counting is the metric used to calculate the PA and energy expenditure parameters.
Limitations of this Study
As stated previously, one major difficulty, when comparing pedometer evaluation studies, is the lack of a standard protocol, making comparisons difficult and error prone. We identified three major variations in the literature on related work: (a) the conditions where the study is performed, (b) placement of the sensors on the body, and (c) the population used.
From our literature search, there are two main approaches: (1) use of a treadmill and (2) free-living walk. The first approach is mainly used to limit the speed to which a person can walk, so that the pedometer can be evaluated at a known speed, whereas the second approach is used mainly due to arguments that treadmills can affect the gait and cadence of a person, which can influence the performance of the pedometer. Some research on the effects of using a treadmill on this type of study is presented elsewhere. 49 –51 The most noted effects of a walk on a treadmill are a faster cadence and a shorter stride length when compared with a free-living walk. Most of the studies agree on these factors, but they disagree on how they can impact the counting results, with some stating that there is not a relevant difference, 50 whereas others state that a statistical significance is observed; therefore caution must be taken with the results. 49 In the case of this study, we consider the described effects not to be a major impact factor because we try to evaluate how the devices perform even when variations of gait and cadence exist. Therefore, we consider that using a treadmill is an acceptable way for these kinds of evaluations. Either way, it is unknown, with the exception of the YM, how the devices' algorithms are designed and how they manage to recognize steps when the described factors are present on the walk.
A factor that can limit the generalizability of the results is the step sample size. Previous research 28 presented evidence that with the increase of gait epochs, the step counting will be balanced; therefore many studies opted to assess the devices under free-living conditions. We acknowledge this limitation, but it will not be developed here as it falls outside the scope of this article.
Another limitation of our study is that we evaluated the pedometers only by placing them on the waist location. Other locations such as ankle, chest pocket, and neck were not considered. The placement of the sensors on the body has been studied previously. 10,38,52,53 All four referenced studies found that posterior positioning of the devices does not affect the counting. The same does not apply to lateral positioning, and significant differences occur in people with higher body mass indexes. Therefore, in our study, the placement of sensors for each trial was minimized to two, in order to minimize possible variations related with device placement. Still, when compared with most of the referenced pedometer evaluation studies, 4,11,13,28,29,33,38,41,43,44 the placement of the sensors may differ, and in some cases it might induce differences in the counting. Also, positioning the pedometer on the different sides of the waist could have caused potential bias in the results as the acceleration experienced on both the locations may not be the same because the gait patterns may not be symmetrical. Comparing the accuracy of the pedometers using the data collected from different trials can also be a limitation of this study. Finally, a common limitation of most related work is the sample of test persons used. In our study, the average age of the participants is around 30 years old and without any impairment, and thus is a population where the assessed speeds are not normally observed. Hence caution must be taken using these results. In our case, not using any of the individuals from the target groups is a weakness of the current study. Nevertheless, it is our intention to do a follow-up study, based on the knowledge gained, with the participation of senior citizens.
As a side note about the population, we described that some changes in gait and cadence may occur when walking on a treadmill. We noticed this, but mainly because the participants walked at speeds to which they are not accustomed. We collected feedback from the participants on how they felt while walking on the treadmill. Some participants noted that their walk felt different when compared with a free-living walk. Some of the reasons for that might be: • the participant is more aware of the walk due to the step counting • the constant speed of the treadmill forces the movement of the person to be rigid, while on a free walk it is more fluid.
It was also observed that, especially at 1 km/h, the participants struggled more to keep the pace. Some tried to “correct” to a pace similar to how they would walk normally, whereas others tried to adapt to the slow speed using shorter steps. In some cases the “gait correction” looked similar to a debilitated walk. We are not sure how these aspects can affect the devices analyzed and we could not find any research that focused on changes of gait.
Conclusions
This study assessed the step count accuracy of three pedometers, YM, OM, and FB, at slow speed using 14 participants. It was observed that the three evaluated devices produced high error rates at 1 km/h and mixed error rates at 2 km/h, and at 3 km/h the error rates were the smallest of the three assessed speeds, with the OM and the FB having a slight overcount. The study was performed with a sample of healthy young participants without disabilities, and therefore the results of this study must be used with care when comparing with other populations, including the elderly and disabled population groups.
As future work we would like to do a follow-up study with participants from the target population, to evaluate more pedometers, and to compare the results among different population groups in order to evaluate how the performance of the devices differ among these groups.
Footnotes
Disclosure Statement
No competing financial interests exist.