
Abstract
Introduction
Mental Health and Depression
Depression is a mood disorder that negatively alters the lives of people, their families, and their social environment, while also causing significant economic losses to society. 1 In a 2011 Chilean National Health Survey, 17% of the population reported symptoms of depression during the past year, and 22% reported a diagnosis of depression at least once in their life. 2 Between 25 and 64 years of age, the prevalence of depression is 19.4%. 2 In Chile, depression diagnoses have been among the main causes of sick leave for mental disorders. 3 According to health insurance provider data, the percentage of sick leave days due to mental disorders increased from 15% in 2005 to 20% in 2008. 4
There is abundant evidence that psychotherapy and pharmacotherapy, especially when used together, are effective in the temporary relief of depression. 5 However, it is also known that for a large group of affected individuals such treatments in their current form do not lead to a permanent remission of depression. There is evidence that this disorder is recurrent and that each episode increases depression risk by 16%. 5 –8 The probability of relapse is higher if there has not been a complete remission of symptoms during treatment, which is common. 6 –8 Interventions aimed at reducing the risk of relapse have been implemented effectively. 6,9,10 At present, maintenance antidepressant medication is one of the most common preventive strategies, but this has some limitations (e.g., lack of compliance or contraindications). 6 Overall, there is a need for innovative strategies to provide medium- and long-term assistance to patients with depression.
Information Technologies for Depression Treatment
Organizations that promote mental health policies have recognized the potential of new information technologies for the prevention and treatment of mental disorders. 11,12 Computerized intervention programs for depression show positive results in terms of efficacy, effectiveness, and cost-effectiveness. 13 –15 Such programs often include interactivity, self-monitoring, information materials (sometimes in multimedia format), and exercises on problem solving, recognition and challenging of dysfunctional thoughts, scheduling of activities, behavioral experiments, and other psycho-educational activities. 16
Given the recursive nature of depression, Web-based interventions have also been suggested to prevent relapse in patients who have completed traditional psychotherapy. 17 –19 A major advantage in this context is that computer-based programs delivered online can be deployed in a cost-efficient manner for long periods, adjusting interventions to the needs of patients and encouraging them to ask for help when symptoms increase.
Based on this background, the Internet-based program SUMMIT was developed for patients with recurrent depression. 17 The effectiveness of the tool is currently being evaluated through a clinical trial in Germany. SUMMIT's strategy is based on previous interventions that have shown positive results. For example, follow-up individual or group treatments via the Internet have been shown to be feasible, safe, and effective in discharged patients, half of whom had been treated for depressive disorders. 18 Given the positive results observed, this type of posthospital care has become a routine clinical practice and has shown to be similarly effective. 18 The purpose of SUMMIT is to extend the symptom-free period and reduce the recurrence of crises through timely intervention. 17 It provides information and education about mental health, aims to generate self-care skills in patients, and offers support for the detection and management of crises and risk behaviors; in addition, when necessary, it fosters access to the regular health system in order to decrease the time between the onset of symptoms and the moment when the person receives professional help.
According to statistics compiled in 2014 by the Ministry of Transport and Telecommunications of Chile, Internet access has reached 56%, considering both stationary and mobile devices, with an average annual growth of 39% over the last 4 years. 20 This indicates that Internet coverage in Chile is extensive, and so the adaptation and implementation of online interventions may now be an option for reducing the difficulties encountered by patients when receiving treatment at primary healthcare centers.
The aim of the present study was to evaluate the capabilities and acceptability of the Chilean version of the program, which is called Apoyo, Seguimiento y Cuidado de Enfermedades a partir de Sistemas Operativos (ASCENSO).
Materials and Methods
Study Design
Data for this acceptability study were collected between January and September 2014 in an outpatient clinic context. Thirty-five patients who had received care for depression as guaranteed by the Chilean health system were recruited. The patients received 8–12 outpatient psychotherapy sessions.
The patients had the following characteristics. Inclusion criteria included men and women between 18 and 65 years of age, with Internet access, who had completed a psychiatric and/or psychological treatment for major depression at a treatment center (PSICOMEDICA) in Santiago de Chile. Exclusion criteria included a Brief Patient Health Questionnaire (PHQ-9) 21 score of ≥15, suicide risk, a history of psychotic symptoms, bipolar disorder, or organic cerebral disorders, severe substance abuse or dependency, and/or personality disorder. Patients with elevated symptom levels were excluded because the intervention aims at stabilizing treatment gains, preventing relapses, and allows early detection of deteriorations. ASCENSO does not provide treatment to fully symptomatic patients.
A quantitative–qualitative methodology was used that included the following assessments: • The patients who refused to participate in the study completed a brief survey that shed light on their reasons for their rejection and their general perception of support programs following therapy. • The PHQ-9 was used for the baseline and biweekly monitoring of the patients who agreed to participate in the study, in order to measure the level of their depressive symptoms. In the final assessment, all participants completed an acceptability and satisfaction questionnaire, and semistructured interviews were conducted in a subgroup to evaluate the users' experience.
Recruitment Procedure
The treatment center was contacted for information about discharged patients. Discharged patients were contacted by phone, they were invited to join the program, and if they were interested in participating, an appointment for a recruitment and introduction session was made at the same treatment center. Patients provided written informed consent prior to their inclusion in the study. During the personal interview, a self-care plan (see below) was constructed with each patient, and the program was explained to them.
Intervention
ASCENSO is an online intervention to provide support to patients after they finish their treatment. Patients interact with the program via a monitoring e-mail that they receive every 2 weeks and a Web site that allows them to access several modules. ASCENSO consists of the following modules:
Monitoring
This module includes the following: (a) online assessment of symptoms every 2 weeks with the PHQ-9 and (b) feedback. Every time data are entered, the program evaluates the state of the patient's symptoms with a predefined algorithm and provides a response that matches his or her current pattern of symptoms, considering his or her depression level and the development of the symptoms over time. In case a participant reports severe impairment during the monitoring (PHQ >19 and/or suicidal ideation), the ASCENSO team automatically receives a notification (“alarm”) and then contacts the patient to explore the need for further professional support.
Self-care plan
In case the monitoring indicates moderate depressive impairment (PHQ-9 = 10–19), the patient receives the recommendation to access his or her personalized self-care plan on the Web site, which reminds him or her to use medication adequately, exercise, approach his or her social contacts, set realistic goals, avoid negative thoughts, and take care of him- or herself.
Online counseling
Participants can book an online appointment for a 30-min real-time session with a psychologist, which is conducted via Internet chat. The patients can access this module at any time. When the monitoring displays severe symptomatology (PHQ-9 > 19), the feedback reminds patients that they can use this service.
Psycho-educational information
The program presents general information about depression (what it is, symptoms, and causes), its treatment (effectiveness, consequences, and likelihood of relapse), and opportunities for prevention.
News
There is a space where news about general mental health topics is posted.
Emergency
This section provides emergency information about what to do and who to contact in a crisis situation.
Contact
The patient can contact the ASCENSO professionals via e-mail with doubts or comments about his or her current state or the functioning of the program.
Data Analysis
Descriptive frequency analyses were conducted with the quantitative data about the use and acceptability of the intervention. At the qualitative level, the positive, negative, and improvable aspects of the participants' experiences were descriptively coded.
Results
A majority (68 out of 93 patients [73%]) were interested in participation. Twenty-five patients were not interested in participation (17 refused participation, and 8 did not attend the initial appointment). Twenty-seven (29%) were excluded because their results in the PHQ-9 showed a moderate or high level of depression, and 6 patients did not have Internet access. Figure 1 shows the flow of participants. The final sample included 35 patients (14 men and 21 women; mean age, 45.8 years [standard deviation = 11.7]).
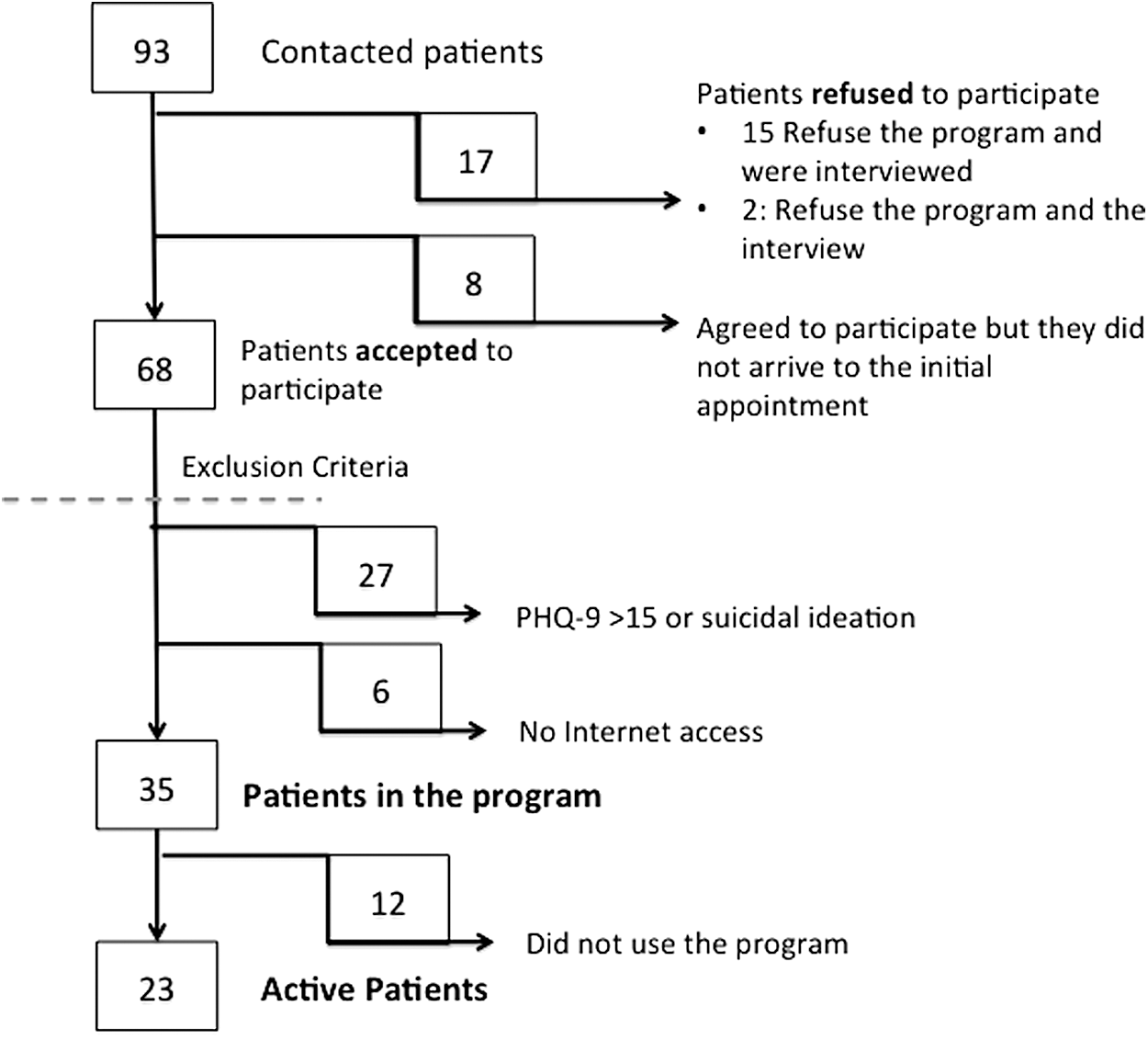
Participant flowchart. PHQ-9, Brief Patient Health Questionnaire.
Fifteen of the 17 patients who refused to participate responded to a rejection survey. The reasons for rejection were lack of time (n = 8, 53%), not knowing how to use a computer (n = 6, 40%), and not wishing to commit to using the program (n = 1, 7%). Of these patients, 9 (60%) mentioned having no problems using the Internet or computers, and all of them considered follow-up programs after therapy to be important. When asked about what the program should include, five individuals (33%) mentioned that they prefer in-person checkup appointments, three (20%) proposed psycho-educational programs, two (13%) stated that the therapist in charge of the treatment should be part of the program, one (6.6%) recommended creating group modules to socialize (e.g., forums or workshops), and four (26%) said they know nothing about the topic.
Use of the Program
The 23 patients who actively used the program were sent a total of 330 messages asking them to complete the PHQ-9 monitoring assessment. Of these messages, 231 (70%) were responded to (Fig. 2).

Monitoring response rate.
Alarm notifications were sent to the ASCENSO team following 11 of the monitoring assessments (4.8%). Five different patients activated these alarms. Three patients activated the alarm once, reporting low symptomatology levels but indicating suicidal ideation in the PHQ-9. As a precaution measure, these patients were contacted by e-mail asking them about their situations and offering them a chat session. Only 2 patients activated the alarm more than once (three and five times) with a PHQ-9 score of >10. These patients were called by the treatment center to resume their treatment. Only 2 patients scheduled an online session with a therapist; however, none of them took place, one due to technical problems that were later solved and the other because of personal problems of the patient.
Of the 12 patients who did not use the program, 6 (50%) blamed technical issues, 4 (33%) referred to a lack of time, and 2 (17%) could not be reached to determine their motives.
Acceptability of the Program
Patients who actively used the program were surveyed about their acceptance of the program and their satisfaction with the support that ASCENSO offered to them (n = 23). Overall, the patients evaluated ASCENSO positively. Patients were asked about their satisfaction with the program in general, and the results are shown in Table 1.
Acceptability and Satisfaction
Concerning the effects of participating in the program, 10 (43%) patients said it was very beneficial, 11 (48%) that it was slightly beneficial, and 2 (9%) that it was neither beneficial nor harmful. None of them stated that participation was harmful. Regarding technical aspects and their usage of the Web site, 14 (61%) participants expressed that it was easy to use, 3 (13%) found it difficult, 3 (13%) required the help of another person, and 3 (13%) could not learn how to use the Web site.
As to the services offered by the program, the participants were asked which modules had been useful to them. Twenty (87%) patients mentioned the monitoring, 6 (26%) referred to information about depression, 2 (9%) brought up the chat system, 1 (4%) mentioned the news, and 1 (4%) did not refer to any module. With respect to the monitoring module, 11 patients (48%) considered that the number of messages received had been low, 12 (52%) thought it had been sufficient, and no one stated that he or she had been sent too many. Patients' evaluations of the feedback messages they received after completing the monitoring questionnaire are given in Table 2.
Patients' Evaluation of the Feedback Messages
Qualitative Evaluation of the Intervention
Ten patients were asked (6 patients who used and 4 did not use the program) to participate in a semistructured qualitative interview about ASCENSO. In it, the patients mentioned positive, negative, and improvable aspects.
Positive aspects
The participants noted that the program was valuable because they regarded it as a form of company and a source of help that complements the treatment without involving additional expenses: I've felt accompanied. With depression you feel alone, being sure that you can count on someone, that they're going to understand you is really helpful. (P2) I'm thankful because it's helpful. Because it's free. (P4)
They also mentioned that it allowed them to understand their mood better and learn about depression: I gradually realized that my state did not persist only because of what I thought… I started noticing the cycles. (P8) I liked the messages…I had a scale of how I'd felt during the week and I asked myself, why? (P10)
Regarding the technical side of the Web site, some patients considered that it worked well and was easy to use: It's all been quite clear and without technical jargon. The website is fine and is easy to use. (P4) I know my way around the Internet, it's not something cold or alien to me. (P6)
The patients rated the psycho-educational information as good, useful, and clear. They said that the monitoring worked well for them and allowed them to know their mood better. The chance to have online sessions was regarded as useful and “a form of support that brings peace of mind” even if they did not use it.
Negative aspects
The users considered it negative that the monitoring questions remained the same over time, which made feedback predictable and generated the notion that the system was impersonal: I don't like the fact that the questions are always the same. One can predict the feedback. (P2) The fact that the questions are the same, I don't know if it has to be that way, I feel like it's always the same thing. Isn't there a way to make it more individual? (P6)
Some mentioned their own lack of use of the program as one of its limitations: I haven't made the most of the program. (P4) I should have checked out more of the services, but I was feeling fine. (P6)
Some participants experienced technical problems when completing the questionnaires and using the Web site: The page is not very friendly for a regular user, it's been really difficult for me to access it. I've had problems responding to the questionnaires. (P3) I got the emails but I was never able to see them well. The page didn't work well for me. (P7)
Participants' recommendations
The patients recommended diversifying the questions included in the monitoring module, detecting recurrent difficulties (specific items) in the responses to further personalize the feedback, and including novel information in the psycho-educational modules: Ask the same things using different questions. (P2) Sorting the difficulties by topic and then be contacted regarding them, in my case I was often having trouble sleeping. (P6)
They also proposed adding more personal spaces for communication, creating spaces for group interaction, and implementing the program in mobile devices: Being able to have a community to share experiences. (P2) I'd like to use it on my phone or my tablet. (P4)
Discussion
Depression is a mental disease that affects the normal development of people's lives. The clinical guide of the Chilean health system recommends that “every person treated for depression, regardless of the severity of the condition, must be followed up for at least 6 months after the total remission of the symptoms.” 22 The limitations of the health system, both logistic and economic, make it impossible to implement this recommendation. Online follow-up and support programs could give health providers and patients an accessible alternative. ASCENSO is the first such program that has been developed and evaluated in Chile.
Internet access in countries such as Chile is on the rise and currently reaches over 50% of the population. 20 Given this relatively high coverage, few people were excluded from the program due to being unable to access the Internet or not knowing how to use the program. Most of the rejections were associated with the patient's lack of time to use the program.
ASCENSO mainly aims at stabilizing treatment gains, preventing relapses, and early detection of deteriorations. Given the short initial treatments in the Chilean healthcare system (8–12 sessions) and that 27 out of 68 patients who were interested in participation had to be excluded because of elevated symptomatology, it might be worthwhile to extend the target population and adjust the intervention in order to address the need of patients who have to terminate treatment although they still suffer from elevated symptomatology.
Patients who actively used ASCENSO displayed a good level of acceptance of the program and the monitoring. They stated that the program was easy to use, helped them to learn about depression, taught them to self-monitor their mood, and involved clear and understandable monitoring, and it was generally regarded as a source of support and as beneficial.
The use of the program reveals a paradox that may be related to the high treatment dropout rates in diseases with lengthy or chronic courses. 23 Although only half of the patients invited to use it actively did so, most of them evaluated it positively. The most personalized module—online chat counseling—was not used by the participants, but it received a positive evaluation, probably because having the option to use it made them feel safe. This fact prompts some questions but also suggests being cautious with respect to the possibilities of full automation. It is probably relevant for participants to “know” that personalized contact is available if they require it. In addition, some patients mentioned that the monitoring and feedback were repetitive and lacked specificity. It is reasonable to speculate that when patients ask for a more individualized program, they refer to those elements of the intervention. In future implementations of ASCENSO, it might be promising to implement a more complex feedback algorithm to improve individualization.
Patients who did not participate stated that they did not respond to the monitoring questionnaires due to technical problems, insufficient contact for solving doubts during the initial phase, and a lack of connection with their prior treatment. This reveals the need to provide a more comprehensive introduction to ASCENSO during the initial treatment phase. This could also prevent most of the technical problems patients experienced (e.g., e-mails that ended up in spam folders).
To improve the program, participants suggest making the modules more personalized and diversifying the monitoring assessments. Also, patients would appreciate the possibility to interact with a therapist from the treatment center where they underwent face-to-face treatment. Finally, it could be promising to initiate the program already during face-to-face treatment and to include clinical contact, even if this contact is minimal. 24 In addition, interactive modules (e.g., discussion boards, blogs) and adjusting the design in order to facilitate the access using mobile devices like smartphones might increase utilization of the program.
The main limitation of this acceptability study is the relatively small sample size. Furthermore, the frequency with which patients accessed the self-care plan, psycho-educational information, news, and emergency modules was not assessed, so that no conclusions on the utilization of these components could be drawn. Strengths include the 100% response rate to the acceptability questionnaire and the fact that the study assessed comprehensive qualitative information on patients' experiences. To our knowledge, this is the first study investigating this kind of intervention in the Chilean healthcare system. In a next step it will be important to conduct a randomized controlled trial to test the efficacy of the program and to investigate whether there are specific subgroups that are more likely to use ASCENSO and benefit from it. Furthermore, cost-effectiveness analyses should be planned as part of future research.
Overall, the present study demonstrates the feasibility and acceptability of ASCENSO as a monitoring and support program for patients with depression. The system complements existing services in several ways. It provides continuous support to patients, helps them to self-monitor, enhances self-care skills, and gives them a space to obtain information and to communicate with professionals during the challenging time following the termination of face-to-face treatment. The combination of automated and personalized modules allows treatment providers to extend their reach at reasonable effort. This increases the chances for a broad and sustained dissemination of ASCENSO in case its efficacy and cost-effectiveness may be demonstrated in future studies.
Footnotes
Acknowledgments
This project was supported by the German Research Foundation (Deutsche Forschungsgemeinschaft) (reference number BA 3352/5-1) and the Fund for Innovation and Competitiveness of the Chilean Ministry of Economy, Development, and Tourism through the Millennium Scientific Initiative (grants NM100018 and IS130005).
Disclosure Statement
No competing financial interests exist.